ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online)
− 416 −
Received: May 14, 2019, Revised: July 12, 2019, Accepted: July 30, 2019, Published online: December 5, 2019
Corresponding author: Hwan Wook Kim, Department of Thoracic and Cardiovascular Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea
(Tel) 82-2-2258-2858 (Fax) 82-2-594-8644 (E-mail) [email protected]
© The Korean Society for Thoracic and Cardiovascular Surgery. 2019. All right reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/
licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Thromboexclusion Treatment for Recurrent Aortic Aneurysm: Still an Option in Select Cases
Jung Suk Choi, M.D., Hwan Wook Kim, M.D., Ph.D.
Department of Thoracic and Cardiovascular Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Flow reversal and thromboexclusion constitute a valuable alternative for aortic surgeons to have within their technical armamentarium for the treatment of aortic aneurysmal disease. Although not usually a preferred treatment for general aortic pathologies, this technique can be considered as a treatment option in select sit- uations, such as mycotic aneurysm, a hostile surgical field, and a poor condition of the patient. Here, we present a case of extra-anatomic bypass and thromboexclusion for recurrent aortic aneurysm after previous extra-anatomic bypass and thromboexclusion surgery.
Key words: 1. Aortic aneurysm 2. Thromboexclusion
Case report
A 78-year-old man was admitted to Seoul St.
Mary’s Hospital with excruciating chest pain accom- panied by an increasingly large aneurysm located on the proximal anastomosis of an extra-anatomic by- pass graft.
He had successfully undergone a conventional aort- ic graft replacement 30 years prior, with the graft extending from the mid-thoracic aorta to the supra- celiac abdominal aorta through a left thoracoabdo- minal incision. This procedure was performed to treat a thoracoabdominal aortic aneurysm, which was categorized as extent V according to Safi’s mod- ification of the Crawford classification system.
The patient was hospitalized again 1 year later af- ter complaining of fever and massive hemoptysis, which he had been experiencing for 3 days. Computed tomography (CT) imaging showed a newly developed aneurysm above the proximal graft as well as left
lower lobar hemorrhage, suggesting an aortobron- chial fistula; therefore, surgery was decided upon and performed.
Thoracotomy revealed severe pleural adhesion and peri-graft fluid collection with non-viable surrounding mediastinal tissues, as well as an aneurysm adjacent to the proximal graft eroding into the adjacent seg- mental bronchus. After thoracotomy, a left lower lo- bectomy was performed. In addition, to avoid anasto- mosis around the infected area, an extra-anatomic aortic bypass was performed from the mid-descend- ing thoracic aorta above the infected graft to the in- frarenal abdominal aorta. The distal anastomosis was done via a separate midline lower laparotomy. The pathologic and microscopic exams revealed a mycotic aneurysm and an aortobronchial fistula.
The patient was discharged uneventfully, but an- other proximal descending thoracic aortic aneurysm, which had been growing slowly, was detected 2 years after the second operation (Fig. 1). The patient
Korean J Thorac Cardiovasc Surg 2019;52:416-419 □ CASE REPORT □
https://doi.org/10.5090/kjtcs.2019.52.6.416
Treatment for Recurrent Aortic Aneurysm
− 417 −
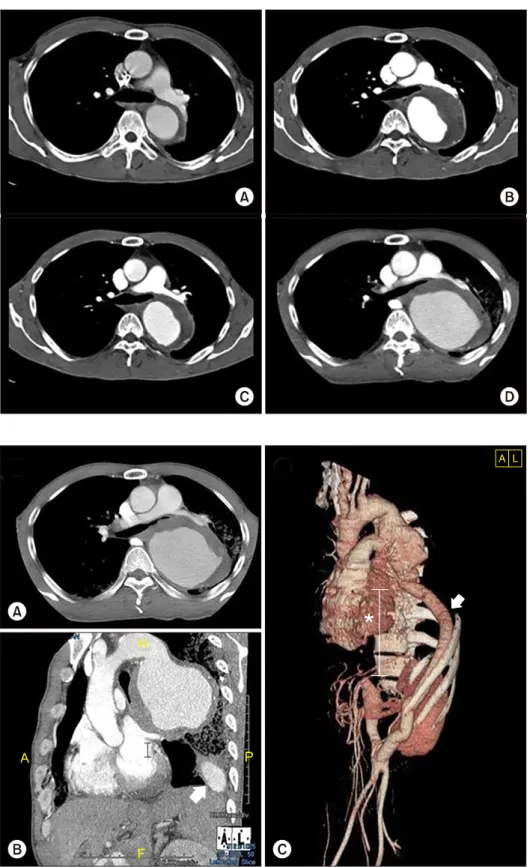
Fig. 1. Follow-up computed tomo- graphic scan 2 years after the sec- ond operation showed a newly de- veloped aortic aneurysm, the size of which increased every year. (A) Image taken 2 years after the sec- ond operation. (B) Image taken 3 years after the second operation.
(C) Image taken 4 years after the second operation. (D) Image taken 5 years after the second operation.
Fig. 2. (A–C) Computed tomographic scan taken 5 years after the second operation. The scan showed a large descending thoracic aortic aneur- ysm with impending rupture. The previous extra-anatomic bypass graft (denoted by the arrow) is accom- panied by the thromboexclused first interposed graft (denoted by the * symbol). A, anterior; P, posterior.
remained asymptomatic over the course of close fol- low-up at our outpatient clinic. However, 5 years lat- er, the patient visited the emergency room again
with severe hemoptysis and chest pain.
CT imaging showed a large descending thoracic aortic aneurysm with an impending rupture (Fig. 2),
Jung Suk Choi and Hwan Wook Kim
− 418 −
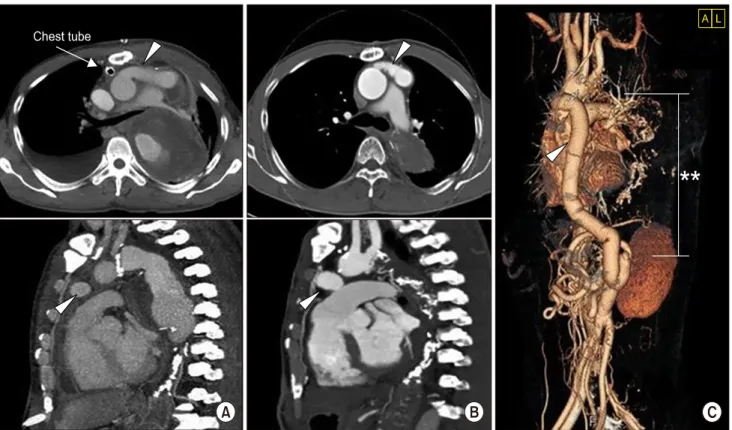
Fig. 3. Follow-up computed tomographic scan with 3-dimensional reconstruction imaging after the third operation. The proximal de- scending thoracic aortic aneurysm and two-thirds of the first previous extra-anatomic bypass graft were completely thromboexcluded (denoted by the ** symbol). The arrowhead shows the second extra-anatomic aortic bypass graft (extending from the ascending aorta to the intraabdominal area of the first previous extra-anatomic bypass graft). (A) Image taken 1 week after the third operation. (B) Image taken 2 years after the third operation. (C) 3-Dimensional reconstruction imaging.
so we opted to perform another extra-anatomic by- pass and thromboexclusion. The patient had no fever, no leukocytosis, and no elevation of C-reactive pro- tein levels, and blood and sputum cultures were negative. Due to the presence of dense pleural adhe- sion from repeated surgery, we decided to perform the second extra-anatomic aortic bypass via sternot- omy, starting from the ascending aorta and extending through the pericardium and diaphragm to the ex- traperitoneal abdominal area, where the previous ex- tra-anatomic bypass graft had been placed. The de- scending thoracic aorta was suture-ligated immedi- ately distal to the left subclavian artery, and a sepa- rate lateral mini-laparotomy was performed at the site of the distal anastomosis.
An immediate postoperative CT scan revealed an incomplete thromboexclusion of the aneurysm at the descending thoracic aorta (Fig. 3A). However, 2 years later, a follow-up CT scan demonstrated complete thromboexclusion of the previous proximal descend-
ing thoracic aortic aneurysm and of two-thirds of the extra-anatomic bypass graft from the second oper- ation (Fig. 3B).
The patient provided written informed consent for the publication of clinical details and images.
Discussion
The extra-anatomic bypass graft provided an alter- native path for blood flow and circumvented the pathological aorta. Therefore, the excluded blind dis- tal aorta, including the diseased aortic segment, ex- hibited stagnant reverse flow leading to progressive thromboexclusion, potentially permitting a period of circulatory adaptation of the spinal cord via collateral vessel formation [1-3]. The main advantages of flow reversal and thromboexclusion are reduced invasive- ness and a lower incidence of postoperative para- plegia than occurs after conventional graft replace- ment [2].
Treatment for Recurrent Aortic Aneurysm
− 419 − Currently, owing to refinements of the surgical technique, meticulous postoperative care, the more widespread use of biologic prosthetic vascular grafts, and increased sophistication of the extracorporeal by- pass, the resection and graft replacement of a dis- eased aorta is typically a standard surgical approach regardless of the site and extent of the condition, particularly in high-risk patients with extensive, com- plex aortic disease [1].
However, in the cases of infected or severely calci- fied aortas that cannot accommodate the suture nee- dle or aortic cross-clamp; hostile surgical fields that cannot be approached directly; or severe concurrent morbidity such as poor cardiac reserve, renal failure, or chronic obstructive pulmonary disease, ex- tra-anatomic bypass and thromboexclusion is still an expedient alternative method of treatment [4,5].
In summary, we report a case of repeated ex- tra-anatomic bypass and thromboexclusion treatment for recurrent aortic aneurysm after initial ex- tra-anatomic bypass and thromboexclusion surgery.
Under certain circumstances, patients might benefit from extra-anatomic bypass and thromboexclusion surgery via sternotomy, especially when graft re- placement via thoracotomy is difficult given a pre- vious history of infection or redo surgery.
Conflict of interest
No potential conflict of interest relevant to this ar- ticle was reported.
ORCID
Jung Suk Choi: https://orcid.org/0000-0001-7733-6408 Hwan Wook Kim: https://orcid.org/0000-0002-5717-9676
References
1. Ku K, Nakayama K, Saitoh Y, et al. Long-term follow-up (8 to 17 years) after thromboexclusion operation for thoracic aortic aneurysms. Ann Thorac Surg 1997;64:399-403.
2. Carpentier A, Deloche A, Fabiani JN, et al. New surgical approach to aortic dissection: flow reversal and thrombo- exclusion. J Thorac Cardiovasc Surg 1981;81:659-68.
3. Elefteriades JA, Hartleroad J, Gusberg RJ, et al. Long- term experience with descending aortic dissection: the complication-specific approach. Ann Thorac Surg 1992;53:
11-20.
4. Crawford ES, Crawford JL, Safi HJ, et al. Thoracoabdominal aortic aneurysms: preoperative and intraoperative factors determining immediate and long-term results of oper- ations in 605 patients. J Vasc Surg 1986;3:389-404.
5. Moon MH, Jo KH, Kim HW. One-stage extra-anatomical to- tal thoracic aorticvrepair. Eur J Cardiothorac Surg 2015;
47:938-9.