중증 외상성 뇌손상 환자의 급성기 치료
서울대학교 의과대학 신경외과학교실 김정은ㆍ박중철ㆍ강현승ㆍ오창완
Controversies in Acute Care of Patients with Severe Traumatic Brain Injury
Jeong Eun Kim, M.D., Jung Cheol Park, M.D., Hyun-Seung Kang, M.D. and Chang Wan Oh, M.D.Department of Neurosurgery, Seoul National University College of Medicine
Traumatic brain injury (TBI) can be pathophysiologically classified into either primary or secondary injury.
It is an important resuscitation to prevent the secondary injury which includes hypoxia, hypotension, cerebral ischemia, and intracranial hypertension, in the acute management of patients with severe TBI.
However, many aspects of the proper management are controversial. The authors focused on the management of the secondary brain injury after TBI and categorized the acute care of the patients with severe TBI as generalized management and management of the intracranial hypertension. They reviewed the pertinent literatures using evidence-based approach and showed practical recommendations for each items. With knowledge of this evidence-based management, appropriate management with better outcome may be accomplished in acute staged TBI. (Brain & NeuroRehabilitation 2008; 1: 136-142) Key Words: acute, evidence-based, management, traumatic brain injury
교신저자: 김정은, 서울시 종로구 연건동 28
110-744, 서울대학교병원 신경외과 Tel: 02-2072-2354, Fax: 02-744-8459 E-mail: eunkim@snu.ac.kr
서 론
외상성 뇌손상은 일차손상과 이차손상으로 구분 지을 수 있다.1 일차손상이란 두부외상의 원인이 되는 충격에 의한 직접적인 손상으로 뇌 좌상, 미만성 축삭손상, 두개 내 혈관 손상에 의한 뇌출혈 등을 가리키며, 이차손상이란 일차손상에 의해 야기되는 간접적이고, 지속적인 손상으 로 저산소증, 저혈압, 뇌허혈, 뇌부종, 뇌혈류의 변화 및 뇌압항진 등의 병태에 의한 손상을 가리킨다. 대개의 경우 글래스고우 혼수지표(Glasgow coma scale)가 12점 이하의 중등도 이상의 외상성 뇌손상의 경우, 일차손상의 내과적, 외과적 응급 처치에 대해서는 큰 이견이 없는 경우가 많 고, 이견이 있다 하더라도 근거중심의학적 관점에서의 대 규모 전향적 무작위 연구를 시행하는데 윤리적인 문제가 따를 수 있는 반면, 이차손상의 경우는 이에 대한 급성기 치료에 따라 환자의 예후가 크게 달라질 수 있어,1,2 중증 외상성 뇌손상의 급성기 치료에서 중요한 부분을 차지하 며, 적절한 치료에 대한 논쟁의 여지가 많다. 따라서 여기 서는 중증 외상성 뇌손상 환자의 급성기 치료에서의 이차
손상의 치료에 대해 집중적으로 논의하고자 하며, 크게 일 반적인 치료(general management)와 타 장기부위와는 다 른 외상성 뇌손상의 특징인 뇌압항진(intracranial hyper- tension)의 치료로 나누어 정리하고자 한다. 일반적인 치 료에 대해서는 뇌관류압(cerebral perfusion pressure), 과 호흡(hyperventilation), 혈색소(hemoglobin)와 적혈구 용 적률(hematocrit), 영양공급(nutrition), 전해질(electrolyte) 의 관리, 및 steroid와 항전간제(anticonvulsant) 등의 약물 치료로 크게 나누어 정리하였고, 뇌압항진의 치료에 대해 서는 뇌압항진 치료의 수준, mannitol, 고장액(hypertonic saline)의 투여, barbiturate 혼수치료(coma therapy), 저체 온(hypothermia) 치료, 및 두개감압절제술(decompressive craniectomy)로 나누어 근거중심의학(evidence-based me- dicine)적 관점에서 고찰하고자 한다. 각각의 항목에 대해 서 2000년도 발표된 Eastern Association for the Surgery of Trauma (EAST) Ad Hoc Committee on Practice Management Guideline Development (available at: http://
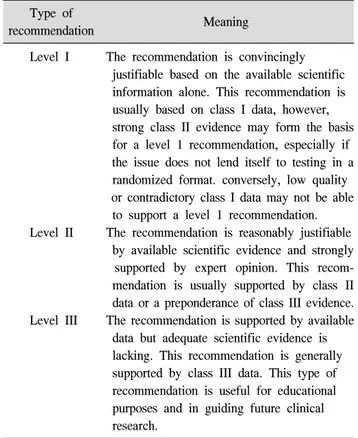
www.east.org/tpg/primer.pdf)에 의하여, 근거수준(strength of evidence, Table 1)과 권고수준(strength of recommen- dation, Table 2)으로 설명하고자 한다.3
Table 2. Level of Recommendation3 Type of
Meaning recommendation
Level I The recommendation is convincingly justifiable based on the available scientific information alone. This recommendation is usually based on class I data, however, strong class II evidence may form the basis for a level 1 recommendation, especially if the issue does not lend itself to testing in a randomized format. conversely, low quality or contradictory class I data may not be able to support a level 1 recommendation.
Level II The recommendation is reasonably justifiable by available scientific evidence and strongly supported by expert opinion. This recom- mendation is usually supported by class II data or a preponderance of class III evidence.
Level III The recommendation is supported by available data but adequate scientific evidence is lacking. This recommendation is generally supported by class III data. This type of recommendation is useful for educational purposes and in guiding future clinical research.
Table 1. Level of Evidence3
Type of evidence Examples
Class I Prospective randomized controlled trials (PRCTs) - the gold standard of clinical trials.
Some may be poorly designed, have inadequate numbers, or suffer from other methodological inadequacies.
Class II Clinical studies in which the data was collected prospectively, and retrospective analyses which were based on clearly reliable data. Types of studies so classified include:
observational studies, cohort studies, prevalence studies, and case control studies.
Class III Studies based on retrospectively collected data. Evidence used in this class indicate clinical series, database or registry review, large series of case reviews and expert opinion.
급성기 중증 외상성 뇌손상 환자의 일반적인 치료
1) 뇌관류압의 관리
(1) 외상성 뇌손상 시에 뇌관류압을 손상 받은 뇌조직에 관류를 증가시키기 위해 높게 유지하는가(>70∼80 mmHg) 혹은 부종 형성을 최소화하기 위해 낮게 유지하는가(50 mmHg) 하는 문제는 이견이 많다. 임상 실험의 class II evidence에서는 뇌 전체의 혈류량(cerebral blood flow, CBF)과 oxygenation에 기초하여 뇌관류압을 60 mmHg로 유지하는 것이 적절하다고 보고하였고,4,5 단일기관 class I evidence에서는 뇌관류압을 높게 유지하는 것이 고혈압과 연관된 이차적 뇌허혈 손상을 줄이기 위해서 필요하다고 보고하였다.2 하지만 뇌허혈 손상 발생시 일시적인 저혈압 에 대한 치료와 비교하여 장기간 신경학적 예후와 차이가 없었으며, 성인 호흡 곤란 증후군(acute respiratory distress syndrome, ARDS) 발생이 다섯 배나 높았다.2
Rosner 등6이 ‘vasodilatory cascade’ 이론에 따라, 뇌압 (intracranial pressure, ICP)를 낮추는 것보다 평균 동맥압 (mean arterial pressure, MAP)를 높임으로써 뇌관류압을 높게 유지하는 것이 좋다는 것을 발표하였고, 무작위 실험 에서는 지지를 받지 못했지만 대체적으로 널리 받아들이 고 있으며 1995년과 2000년 판의 Brain Trauma Foundation’s Head Injury Guidelines에 선택사항으로 채택되었다.7 ‘Lund therapy’에서는 뇌부종을 최소화하기 위해 미세 혈관압을 낮추는 접근법을 강조하였고, 이는 뇌관류압 공
식 (뇌관류압 = 평균 동맥압 − 뇌압)에 의거해 뇌압 치료 에 중점을 두어 뇌관류를 유지하는 데 중점을 두었다.8 다 른 연구에서는 외상성 뇌손상의 다양성에 근거하여 각 환 자의 병태생리에 따라 치료를 달리하여야 한다고 보고한 경우도 있다.9
즉, ‘뇌관류압 = 평균 동맥압 − 뇌압’에 따라 Rosner 등6은 평균 동맥압을 높게 유지하는 것을 강조하였고, Lund therapy에서는 뇌압을 낮추는 것을 강조하였으며8 개별 접근에서는 모든 변수를 정상화하는 것을 강조하였 다.9 일차적인 목표는 모두 손상된 뇌조직에 관류를 증가 시키는 데 있다.
(2) 외상성 뇌손상 후의 뇌관류압의 최소 안전 역치를 구하기 위해 많은 전향적 임상 실험이 시행되었으며, 뇌관 류압 증가에 따른 뇌혈류 또는 oxygenation의 변화가 더 이상 일어나지 않는 뇌관류압 역치는 60∼70 mmHg였 다.5,10 그러나 이 경우에 국소부위의 허혈이 발생할 수 있 는 여지가 있어 60∼70 mmHg 보다 높게 유지하는 것이 국소 뇌 oxygenation을 증가 시킬 수 있다.10 다른 전향적 임상 실험에서는 비록 다른 원인을 배제하지는 못했지만 뇌관류압과 외상성 뇌손상 후의 예후와의 관계를 고려했 을 때 성인에서 60 mmHg의 뇌관류압 최소 역치를 보고하
였다.11,12 이로 인해 일반적으로 최소 60 mmHg로 뇌관류
압을 유지하는 것이 받아들여지고 있지만 이보다 높게 유 지하는 것이 좋은 지에 대해서는 아직 논란이 많은 상태이 나 뇌관류압을 높게 유지하는 것이 이차적 뇌허혈 손상과 뇌압을 낮추는 데 잠재적 이익이 있을 것으로 생각된다.
Robertson 등2이 평균 동맥압과 뇌관류압을 각각 90 mmHg 이상과 70 mmHg 이상 유지하고 저탄소증을 막기 위해 과호흡을 하지 않은 뇌혈류 겨냥 protocol (CBF targeted protocol)과 평균 동맥압과 뇌관류압을 각각 70 mmHg 이상, 50 mmHg 이상으로 유지하면서 중등도의 과 호흡을 시킨 뇌압 겨냥 protocol (ICP-targeted protocol)을 비교하였다. 몇 가지 제한점이 있지만 이 실험에 의해 뇌 혈류 겨냥 protocol 군에서 경정맥 산소 포화도가 높은 것 으로 보고되었고, 이는 치료 방법에 있어 저혈압과 저탄소 상태를 최소화하는 것이 이차적 뇌허혈 손상을 줄이는 데 도움을 줄 수 있다.
(3) 권고사항: 일반적으로 뇌관류압은 70 mmHg 이상으 로 유지하는 것이 이차적 뇌허혈 손상을 막을 수 있지만, 뇌압을 낮추더라도 신경학적 예후와는 연관이 없는 것으 로 알려져 있다. 따라서, 심한 외상성 뇌손상 환자에서 적 어도 뇌관류압을 60 mmHg로 유지하는 것이 적절하며, 인 위적으로 혈압을 높일 경우 폐기능 저하 등의 합병증이 발생할 우려가 있어 70 mmHg 이상으로 유지하는 것은 국소적 뇌허혈이 있는 경우 등 적응이 되는 경우에 사용할 수 있다(level I recommendation).
뇌관류압을 올림으로써 단기간에 뇌압을 낮추는 것은 환자의 자동조절 능력이 적절히 작용하는 가에 달려있으 며, 작용 시 뇌압은 혈압이 올라갈수록 낮아지며, 반대로 작용하지 않을 시 혈압 상승에 따라 뇌압도 상승하게 된 다. 뇌관류압을 적절한 수준보다 올리는 것은 뇌압의 장기 적 예후에 영향이 없다(level II recommendation).
2) 과호흡
(1) 뇌압항진 환자에서 다른 진단적 혹인 치료 방법이 시작되기 전에 단기간으로 과호흡 치료를 하는 것 이외에 는 효과가 없다. 또한 뇌압항진을 막기 위해 예방적으로 과호흡을 하는 것도 효과가 없으며, 오히려 장기간 과호흡 시 뇌허혈을 조장할 수도 있다(class II and III evidence). 외 상성 뇌손상 환자에서 호기말 양압호흡(positive end ex- piratory pressure, PEEP)을 시행하는 것은 효과가 없으나, 정상압으로 고산소분압 호흡은 어느 정도 효과가 있을 것 으로 생각되고 있다(class III evidence).
(2) Suazo 등13은 과호흡 후 4∼6시간 안에 뇌척수액 pH 조절에 의해 뇌동맥 직경, 뇌압, 뇌혈류가 정상화되거나 오히려 반향적으로 충혈이나 뇌압 상승을 보고하였다.
Muizelaar 등14은 5일간 예방적으로 과호흡을 시행한 환자 에서 3개월과 6개월에 예후가 좋지 않은 것으로 보고하였다.
(3) 권고사항: 예방적 혹은 장기간에 걸친 과호흡 치료 는 피해야 하나, 급격한 뇌압항진에 의한 뇌허탈(brain herniation)이 예측되는 경우 일시적으로 중등도의 과호흡 (PaCO2 >25 mmHg)을 시행할 것을 제시하고 있다(level II recommendation).
3) 혈색소와 적혈구 용적률의 관리
(1) 실험적 연구를 통해 혈액의 점도와 산소 운반 능력 등을 토대로 적혈구 용적률을 30∼35%로 맞추는 것이 외 상성 뇌손상 환자에서 적절하다고 알려져 있다.15 자동 조 절 능력이 작용하는 경우 점도는 뇌혈류에 영향을 적게 미치나, 자동 조절 능력이 소실되어 혈관이 최대한으로 확 장되어 있는 경우에는 점도가 뇌혈류를 결정하는 중요한 요소가 된다. 즉, Hagen-Poiseuille 공식에 의해 적혈구 용 적률을 45∼50%에서 30∼35%로 낮출 경우 뇌혈류는 약 두 배가 된다. 적혈구 용적률을 30% 이하로 낮출 경우에는 산소 운반 능력이 현저히 떨어지며 점도에는 영향이 별로 없게 된다. 임상 시험에서 적혈구 용적률의 상승이 뇌혈류 를 낮추고 경색 부위를 크게 하는데 연관이 있다고 보고되 고 있다(class III evidence).16
(2) 권고사항: 적혈구 용적률은 30∼35%, 혈색소는 10 mg/dl를 유지할 것을 권고하고 있다(level III recommen- dation).
4) 영양공급의 관리
(1) 외상성 뇌손상 환자에서 영양공급은 감염성 합병증 에 의한 사망률과 유병률을 낮추는 데 있어 중요한 요소이 다. 따라서, 장관 영양(enteral nutrition, EN)을 통해 가능 하면 일찍 섭취하는 것이 장점막의 유지, 장내 세균의 전 위의 최소화 등에서 좋으나, 그렇지 못할 경우에는 장관외 영양(parenteral nutrition, PN)을 손상 후 조기에 시행하는 것이 바람직하다. 장관내 영양의 경우 장관 섭취 장애, 흡 인성 폐렴 등의 문제가 발생할 소지가 있다.17 심한 뇌손상 환자(글래스고우 혼수지수 4∼5점)에서 대사 반응은 체표 면적의 20∼40%에 해당하며, 이는 정상시의 168 ± 53%에 해당한다.18
(2) 권고사항
가) 시작 시기: 영양공급을 언제 시행하는가 하는 여러 가지 실험에서, 일찍 시작한 군에서 대체적으로 감염성 합 병증의 비율이 낮았고 예후가 좋은 것으로 나타났다. 손상 후 48에서 72시간 이내에 시행할 것을 제시하고 있다(level I recommendation).19,20
나) 영양공급 경로: 영양공급의 방법에 있어서는 장관 내 영양과 장관외 영양 사이에 특별한 차이가 없는 것으로 보고되나 장관외 영양에서 주입관과 연관된 합병증, 패혈 증, 전해질 불균형 등의 합병증이 조금 높은 것으로 보고 되고 있다.17,20,21 따라서 장음이 확인되지 않거나 위장 장 애가 있을 경우에 공장 식이(jejunal feeding)를 이용해 일찍 영양공급을 시행할 수 있다(level II recommendation).17 다) 영양공급의 구성: 휴식시의 대사량의 140% 이상이 공급되어야 하며, 칼로리의 15% 이상을 단백질로 공급하 여야 한다(level III recommendation).17,22,23
5) 전해질의 관리
(1) 급성 또는 진행하는 저나트륨혈증과 저삼투압은 뇌 부종, 뇌압상승, 전간(seizure) 등과 연관이 있고,24-26 고나트 륨혈증은 중심성 탈수초증(central myelinolysis)을 유발할 수 있어27 혈중 나트륨은 135 mEq/L에서 150 mEq/L를 유 지해야 한다. 저나트륨혈증의 기전은 손상 후 초기에는 항 이뇨 호르몬의 과다 분비,28,29 이후에는 염류 소실(salt wasting)에 의해 생긴다.30,31 대부분의 저나트륨혈증을 보 이는 뇌손상 환자에서 뇌성 염류 소실이 있으므로, 치료는 수분 제한보다는 고장성의 식염수를 통해 나트륨을 높이 는 것이 안전하고 효과적이다. 나트륨 교정의 속도는 중심 성 탈수초증을 막기 위해 하루에 15 mEq/L 이상 교정하지 말아야 한다.27
(2) 권고사항: 혈청 나트륨은 135∼150 mEq/L를 유지 하며(level III recommendation), 저나트륨혈증에서는 수분 제한 보다는 고장성 식염수, fludrocortisones acetate, urea 를 정맥 주입하며 중심성 탈수초증을 예방하기 위해 하루 에 15 mEq/L 이상 교정하지 말아야 한다. 고나트륨혈증 의 치료는 나트륨 양을 제한한 수분 섭취를 늘리고, 심한 경우에는 신장에서의 수분 배출을 줄이기 위해 항이뇨호 르몬(DDAVP)을 주입할 수도 있다(level III recommen- dation).
6) Steroid의 사용
(1) Steroid는 외상성 뇌손상 환자에서 적응이 되지 않는 다.32 고용량 steroid를 심한 뇌손상을 유발한 실험용 쥐에 주입하였을 때, lipid peroxidation은 억제하나, glutamate- mediated toxicity에는 영향이 없는 것으로 밝혀졌다.33 고 용량 steroid의 합병증으로는 위점막 궤양, 위장관 출혈 및 천공,34 대퇴부의 무혈성 괴사 및 감염성 질환 등35,36이 있 을 수 있다.
(2) 권고사항: 일반적으로 외상성 뇌손상 환자에서 steroid는 효과가 없으며 여러 합병증을 유발하여 전체적
인 예후는 나쁠 수 있다(level I recommendation).
7) 예방적 항전간제의 사용
(1) 심한 외상성 뇌손상 환자의 약 20∼25%에서 적어도 한번은 외상 후 경련을 경험하게 된다.37 외상성 뇌손상 후 항전간제의 사용으로 초기 경련을 줄일 수 있다는 보고가 많이 있다.38 초기 외상 후 경련의 위험이 높은 환자에서 phenytoin, carbamazepine 혹은 phenobarbital을 약 1주일 간 사용하는 것이 합당하다.39 그러나 현재까지의 연구에 서 초기 경련의 예방이 이차적 뇌손상이나 신경행동(neuro- behavioral) 예후에 영향이 있는지는 알려져 있지 않다. 이 런 이유로 초기 경련의 예방이 사망률, 유병률, 후기 외상 후 경련을 낮추는가에 대한 증거는 없다. 약 25%의 초기 경련 환자에서 후기 경련이 나타났으며 후기 경련의 예방 을 위해 뇌손상 후 1주일 넘어서 항전간제를 쓰는 것은 권고되고 있지 않다.39
(2) 권고사항: 초기 외상 후 경련을 낮추기 위해 1주일 간 예방적 항전간제 치료를 시행한다(level I recommen- dation). 1주일간 항전간제 사용이 사망률이나 유병률을 줄이지는 않는다(level III recommendation). 1주일 이후에 항전간제를 사용하는 것은 후기 외상 후 경련을 예방하지 못하므로 권고되지 않는다(level I recommendation).
급성기 중증 외상성 뇌손상 환자의 뇌압항진에 대한 치료
1) 뇌압항진 치료의 적정 수준
(1) 치료를 시작해야 하는 뇌압은 20 mmHg이나, 두개 감압절제술을 시행한 경우나 측두엽에 종양병변이 있는 경우 15 mmHg에서 치료를 시작할 것이 제시되고 있
다.40,41 Marmarou 등42은 뇌압과 예후의 관계를 조사하여,
나쁜 예후 인자로 뇌압이 20 mmHg 이상인 것을 확인하였 으며, 이는 나이, 입원시의 상태, 동공반응의 소실보다 더 예후와 연관이 있는 것을 보고하였다. Saul과 Ducker41는 뇌압이 15 mmHg 이상에서 치료를 한 결과 사망률이 28%
를 보고하여, 20 mmHg 이상에서 치료한 환자군보다 사망 률(46%)이 낮은 것을 확인하였다.
(2) 권고사항: 20 mmHg 이상에서 치료를 시작한다 (level II recommendation). 하지만 20 mmHg에서 치료를 시작한 군과 15 mmHg에서 치료를 시작한 군 사이에 예후 의 차이가 있는지에 대한 연구가 필요하다. 측두엽에 종양 병변이나 두개감압절제술을 시행한 경우에는 15 mmHg 에서 치료를 시작한다(level III recommendation).
2) Mannitol의 사용
(1) Mannitol의 작용 기전은 주로 혈류역학적 작용에 의 하며, 뇌압에 대한 직접적 영향이 적음에도 불구하고 뇌혈 류에 상당한 영향을 미친다.43
(2) 권고사항: 신경학적 검사나 CT 검사의 결과로 초기 에는 경험적 고용량 mannitol (1.8∼2.1 g/kg)을 사용한다 (level I recommendation). 뇌압 모니터링이 시작되면 20%
mannitol을 0.25∼1.0 g/kg 용량으로 bolus로 주입한다 (level II recommendation). 갑작스런 저혈압을 예방하기 위 해 0.25∼1.0 g/kg을 15분 이상 천천히 지속적으로 주입한 다. Mannitol은 뇌관류압이 70 mmHg 이하일 때 효과적이 며, 수분 손실을 막기 위해 적절한 수분 보충이 필요하다.
혈장 osmolar gap은 55 mOsm/L 이하, 혈장 삼투압은 320 mOsm/L 이하로 유지한다(level III recommendation).
3) 고장액의 사용
(1) 고장성 식염수를 뇌압상승의 치료로 사용할 수 있 다. 또한 mannitol의 대체로 고장성 식염수를 쓸 수 있다.
그러나, 고장성 식염수의 사용이 예후에 영향을 주는 지는 아직 밝혀지고 있지 않다. 중심성 교 탈수초증(central pontine myelinolysis)나 급성 신부전 등의 고장성 식염수 치료시 나타나는 중요 합병증은 잘 일어나지 않으나, 반향 적으로 뇌부종이 진행되거나 사망률이 증가한다고 보고 된 바도 있다.44
(2) 권고사항: 심한 외상성 뇌손상 후, 뇌척수액 배액, 과호흡, mannitol, furosemide 등의 치료에 불응하는 경우 고장성 식염수의 주입이 어느 정도 효과가 있는 것으로 알려져 있다. 가장 흔히 사용되는 고장성 식염수는 3% 식 염수로 초기 용량은 1.5∼3.0 ml/kg이 가장 적당하다. 혈장 나트륨 농도는 155∼160 mEq/L 이하를 유지하는 것이 좋 다(level III evidence).
4) Barbiturate 혼수 치료
(1) Barbiturate가 심한 외상성 뇌손상 환자에서 사망률 과 유병률을 낮춘다는 증거는 없다. 하지만 일부 환자에서 다른 일반적인 치료에 불응인 경우 뇌압을 낮추는 한 방법 으로 여겨지고 있다.45 Pentobarbital의 경우 10 mg/kg을 30 분에 걸쳐 주입하고, 이후 3시간 동안 5 mg/kg/hr의 속도 로 주입한다. 만약 이 경우 혈압이 떨어지면, 주입 속도를 늦춘다.45 Barbiturate 혼수 치료의 한가지 절대적 금기는 저혈압을 포함하는 심혈관 기능저하이다.40 또 한가지 주 의해야 할 점은 barbiturate 혼수 치료를 받는 환자에서 면 역성 결여와 체온 유지가 안되어 백혈구과다증(leuko-
cytosis), 열감(febrile sensation), 심계 항진(palpitation) 등의 초기 감염 증상이 억제될 우려가 있다는 것이다.46 (2) 전향적 무작위 실험에서 pentobarbital이 뇌압 조절 하는데 있어 mannitol 보다 덜 효과적이라고 밝혀졌다. 모 든 외상성 뇌손상 환자에서 예방적으로 pentobarbital을 사 용할 경우 예후는 변화가 없이 혈압 하강만을 가져온다.40 (3) 권고사항: 뇌압을 낮추기 위해 다른 방법들을 최대 한 동원하고 있는 경우 고용량의 barbiturate가 뇌압을 낮 추는 치료법이 될 수 있다. 이 경우 저혈압을 동반하고 있 지 않아야 한다(level II evidence). 뇌압 상승을 막기 위해 예방적으로 barbiturate를 사용하는 것은 적응증이 되지 않 는다(level I evidence).
5) 저체온 치료
(1) 입원 당시 저체온증이 있으며 45세 미만의 심한 외 상성 뇌손상 환자중 23%에서 저체온을 유지하였을 때, 예 후가 좋다는 보고가 있다.47 대체로 손상 후 3시간 이내에 저체온 치료를 시작하는 것이 예후에 좋은 영향을 미친다.
다른 보고에서는 정상 체온을 유지한 경우와 저체온 치료 를 한 경우에 있어 예후의 차이는 없으나, 저체온 치료를 한 경우 뇌압 상승의 최고치를 무디게 한다고 하였다.47 (2) 권고사항: 저체온 치료를 심한 외상성 뇌손상 환자 에서 치료법으로 사용하는 가에 대해서는 아직 논란이 많 은 편이다. 그러나 저체온 치료시 뇌압 상승의 최고치를 낮추는 것으로 알려져 있다. 이런 목적으로 저체온 치료를 한 경우 예후와 연관이 있는지는 임상적으로 알려져 있지 않다(level I evidence).
6) 두개감압절제술
(1) 두개감압절제술 후 첫 24시간 동안 뇌압이 35 mmHg 이상 지속적으로 상승되어 있을 경우 거의 100%
사망률을 보인다.48 두개감압절제술 시행시 중뇌주위 수조 (perimesencephalic cistern) 부위의 감압을 최대화 하기 위 해 중두개와(middle cranial fossa) 바닥이 노출될 정도로 내 려서 시행한다. 골편은 1∼3개월 후 정상 뇌혈류와 대사를 복구하고 두통, 어지러움, 피로, 기억력 저하, 우울증 등의
‘syndrome of trephined’12를 막기 위해 두개성형술을 시행 하여 재위치 시킨다.49
(2) 권고사항: 뇌압 모니터링을 시행하고 있는 환자에 서 다른 일반적인 치료에 반응하지 않는 뇌압 상승이 지속 될 경우, 뇌관류가 손상 받기 전에 즉각적으로 두개감압절 제술이 고려되어야 한다(level II evidence). Level III. 두개 감압절제술의 지연이 진행하는 국소적 또는 전반적인 뇌 허혈 손상에 대한 감압술 후 효과가 없는 가장 중요한 원
인이다(level III evidence). 뇌부종의 분포에 따라 골편 제거 술은 일측성, 양측성 또는 양측 전두골 등을 사용할 수 있 다(level III evidence).
결 론
중증 외상성 뇌손상 환자의 급성기 치료는 일차손상 및 이차손상의 치료로 나눌 수 있다. 지연성의 추가 손상을 방지하기 위해서는 이차손상의 예방이 필수적이다. 이차 손상의 예방에는 급성기의 일반적인 치료와 뇌압항진에 대한 치료가 포함된다. 각각의 치료에 대해서는 논란의 여 지가 있을 수 있으므로, 근거중심의학적 접근에 의한 권고 사항에 대해서 잘 알고 접근함으로써 적절한 치료로써 보 다 나은 예후를 기대할 수 있다.
감사의 글
본 논문은 2008년 춘계 대한뇌신경재활학회에서 발표되 었음.
참 고 문 헌
1) Chesnut RM, Marshall LF, Klauber MR, Blunt BA, Baldwin N, Eisenberg HM, Jane JA, Marmarou A, Foulkes MA. The role of secondary brain injury in determining outcome from severe head injury. J Trauma. 1993;34:216-222
2) Robertson CS, Valadka AB, Hannay HJ, Contant CF, Gopinath SP, Cormio M, Uzura M, Grossman RG.
Prevention of secondary ischemic insults after severe head injury. Crit Care Med. 1999;27:2086-2095
3) Eastern association for the surgery of trauma (east) ad hoc committee on practice management guideline development.
Utilizing evidence-based outcome measures to develop practice management guidelines: a primer. Website of the Eastern Association for the Surgery of Trauma. 2000;
Available at: http://www.east.org/tpg/primer.pdf
4) Cruz J, Jaggi JL, Hoffstad OJ. Cerebral blood flow, vascular resistance, and oxygen metabolism in acute brain trauma:
Redefining the role of cerebral perfusion pressure? Crit Care Med. 1995;23:1412-1417
5) Bruzzone P, Dionigi R, Bellinzona G, Imberti R, Stocchetti N. Effects of cerebral perfusion pressure on brain tissue po2 in patients with severe head injury. Acta Neurochir.
1998;71:111-113
6) Rosner MJ, Rosner SD, Johnson AH. Cerebral perfusion pressure: management protocol and clinical results. J Neurosurg. 1995;83:949-962
7) The Brain Trauma Foundation. The american association of neurological surgeons. The joint section on neurotrauma and
critical care. Guidelines for cerebral perfusion pressure. J Neurotrauma. 2000;17:507-511
8) Eker C, Asgeirsson B, Grande PO, Schalen W, Nordstrom CH. Improved outcome after severe head injury with a new therapy based on principles for brain volume regulation and preserved microcirculation. Crit Care Med. 1998;26:
1881-1886
9) Miller JD, Piper IR, Dearden NM. Management of intracranial hypertension in head injury: Matching treatment with cause. Acta Neurochir (Wien). 1993;57:152-159 10) Stocchetti N, Chieregato A, De Marchi M, Croci M, Benti
R, Grimoldi N. High cerebral perfusion pressure improves low values of local brain tissue o2 tension (ptio2) in focal lesions. Acta Neurochir. 1998;71:162-165
11) Struchen MA, Hannay HJ, Contant CF, Robertson CS. The relation between acute physiological variables and outcome on the glasgow outcome scale and disability rating scale following severe traumatic brain injury. J Neurotrauma.
2001;18:115-125
12) Chambers IR, Treadwell L, Mendelow AD. Determination of threshold levels of cerebral perfusion pressure and intracranial pressure in severe head injury by using receiver-operating characteristic curves: an observational study in 291 patients. J Neurosurg. 2001;94:412-416 13) Carmona Suazo JA, Maas AI, van den Brink WA, van
Santbrink H, Steyerberg EW, Avezaat CJ. Co2 reactivity and brain oxygen pressure monitoring in severe head injury. Crit Care Med. 2000;28:3268-3274
14) Muizelaar JP, Marmarou A, Ward JD, Kontos HA, Choi SC, Becker DP, Gruemer H, Young HF. Adverse effects of prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J Neurosurg. 1991;75:
731-739
15) Muizelaar JP. Cbf and management of the head-injured patient. In: Narayan RK, Wilberger JE, Povlishock JT, eds.
Neurotrauma. New York: McGraw-Hill; 1996:553-561.
16) Harrison MJ, Pollock S, Kendall BE, Marshall J. Effect of haematocrit on carotid stenosis and cerebral infarction.
Lancet. 1981;2:114-115
17) Grahm TW, Zadrozny DB, Harrington T. The benefits of early jejunal hyperalimentation in the head-injured patient.
Neurosurgery. 1989;25:729-735
18) Robertson CS, Clifton GL, Grossman RG. Oxygen utilization and cardiovascular function in head-injured patients.
Neurosurgery. 1984;15:307-314
19) Taylor SJ, Fettes SB, Jewkes C, Nelson RJ. Prospective, randomized, controlled trial to determine the effect of early enhanced enteral nutrition on clinical outcome in mechanically ventilated patients suffering head injury. Crit Care Med. 1999;27:2525-2531
20) Young B, Ott L, Twyman D, Norton J, Rapp R, Tibbs P, Haack D, Brivins B, Dempsey R. The effect of nutritional support on outcome from severe head injury. J Neurosurg.
1987;67:668-676
21) Borzotta AP, Pennings J, Papasadero B, Paxton J, Mardesic
S, Borzotta R, Parrott A, Bledsoe F. Enteral versus parenteral nutrition after severe closed head injury. J Trauma.
1994;37:459-468
22) Clifton GL, Robertson CS, Grossman RG, Hodge S, Foltz R, Garza C. The metabolic response to severe head injury. J Neurosurg. 1984;60:687-696
23) Clifton GL, Robertson CS, Contant CF. Enteral hyper- alimentation in head injury. J Neurosurg. 1985;62:186-193 24) Doczi T, Tarjanyi J, Huszka E, Kiss J. Syndrome of
inappropriate secretion of antidiuretic hormone (siadh) after head injury. Neurosurgery. 1982;10:685-688
25) Unterberg A, Kiening K, Schmiedek P, Lanksch W. Long-term observations of intracranial pressure after severe head injury.
The phenomenon of secondary rise of intracranial pressure.
Neurosurgery. 1993;32:17-23
26) Arieff AI. Hyponatremia, convulsions, respiratory arrest, and permanent brain damage after elective surgery in healthy women. N Engl J Med. 1986;314:1529-1535
27) Soupart A, Decaux G. Therapeutic recommendations for management of severe hyponatremia: current concepts on pathogenesis and prevention of neurologic complications.
Clin Nephrol. 1996;46:149-169
28) Davis BP, Matukas VJ. Inappropriate secretion of antidiuretic hormone after cerebral injury. J Oral Surg. 1976;34:609-615 29) Imbert Y, Peroua JJ, Coomans D, Haissaguerre M, Henrion
P, Leng B. Inappropriate secretion of antidiuretic hormone (isadh) after head injury (author's transl). Sem Hop. 1982;
58:1151-1154
30) Peters JP, Welt LG, Sims EA, Orloff J, Needham J. A salt-wasting syndrome associated with cerebral disease. Trans Assoc Am Physicians. 1950;63:57-64
31) Cort JH. Cerebral salt wasting. Lancet. 1954;266:752-754 32) Bracken MB, Collins WF, Freeman DF, Shepard MJ, Wagner
FW, Silten RM, Hellenbrand KG, Ransohoff J, Hunt WE, Perot PL Jr. Efficacy of methylprednisolone in acute spinal cord injury. JAMA. 1984;251:45-52
33) Uhler TA, Frim DM, Pakzaban P, Isacson O. The effects of megadose methylprednisolone and u-78517f on toxicity mediated by glutamate receptors in the rat neostriatum.
Neurosurgery. 1994;34:122-127
34) Weiner HL, Rezai AR, Cooper PR. Sigmoid diverticular perforation in neurosurgical patients receiving high-dose corticosteroids. Neurosurgery. 1993;33:40-43
35) Keogh P, Masterson E, Quinlan W. Bacterial arthritis in the neurosurgical patient: report on four cases. Neurosurgery.
1994;34:364-367
36) Nagashima G, Suzuki R, Asai J, Fujimoto T, Atsumi T.
Avascular necrosis of the femoral head caused by steroid treatment in neurosurgery. No Shinkei Geka. 2000;28:
523-528
37) Jennett B. Epilepsy after Non-missile Head Injuries. Chicago:
Year Book Medical Publishers; 1975
38) Young B, Rapp RP, Norton JA, Haack D, Walsh JW. Failure of prophylactically administered phenytoin to prevent post- traumatic seizures in children. Childs Brain. 1983;10:185-192 39) Temkin NR, Dikmen SS, Anderson GD, Wilensky AJ, Holmes
MD, Cohen W, Newell DW, Nelson P, Awan A, Winn HR.
Valproate therapy for prevention of posttraumatic seizures: a randomized trial. J Neurosurg. 1999;91:593-600
40) Eisenberg HM, Frankowski RF, Contant CF, Marshall LF, Walker MD. High-dose barbiturate control of elevated intracranial pressure in patients with severe head injury. J Neurosurg. 1988;69:15-23
41) Saul TG, Ducker TB. Effect of intracranial pressure monitoring and aggressive treatment on mortality in severe head injury. J Neurosurg. 1982;56:498-503
42) Marmarou A, Anderson RL, Ward JD, Choi SC, Young HF, Eisenberg HM, Foulkes MA, Marshall LF, Jane JA. Impact of instability and hypotension on outcome in patients with severe head trauma. J Neurosurg. 1991;75:S59-S66
43) Muizelaar JP, Lutz HA 3rd, Becker DP. Effect of mannitol on icp and cbf and correlation with pressure autoregulation in severely head-injured patients. J Neurosurg. 1984;61:
700-706
44) Qureshi AI, Suarez JI, Bhardwaj A. Malignant cerebral edema in patients with hypertensive intracerebral hemorrhage associated with hypertonic saline infusion: a rebound phenomenon? J Neurosurg Anesthesiol. 1998;10:188-192 45) Cormio M, Gopinath SP, Valadka A, Robertson CS. Cerebral
hemodynamic effects of pentobarbital coma in head-injured patients. J Neurotrauma. 1999;16:927-936
46) Schalen W, Messeter K, Nordstrom CH. Complications and side effects during thiopentone therapy in patients with severe head injuries. Acta Anaesthesiol Scand. 1992;36:369-377 47) Clifton GL, Miller ER, Choi SC, Levin HS, McCauley S,
Smith KR Jr, Muizelaar JP, Wagner FC Jr, Marion DW, Luerssen TG, Chesnut RM, Schwartz M. Lack of effect of induction of hypothermia after acute brain injury. N Engl J Med. 2001;344:556-563
48) Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975;1:480-484
49) Yamaura A, Makino H. Neurological deficits in the presence of the sinking skin flap following decompressive craniectomy.
Neurol Med Chir (Tokyo). 1977;17:43-53