원 저
ISSN 2093-9272 일산병원학술지 2017;16(1):1-3Volume 16 Number 1 June 2017
1
전립선비대증과 전립선암 환자에서 배뇨증상의 차이
국민건강보험 일산병원 비뇨기과
김영식
Comparison of Lower Urinary Tract Symptoms in Benign Prostatic Hyperplasia and Prostate Cancer
Young Sig Kim
Department of Urology, National Health Insurance Service Ilsan Hospital, Goyang, Korea
Background: To investigate whether men with severe voiding symptoms are at increased risk for being diagnosed with prostate cancer.
Methods: We retrospectively analyzed the clinical records of patients (n=1,850) underwent prostate biopsy between 2006 and 2013. The indications for prostate biopsy included elevated PSA level (≥4 ng/mL), abnormal digital rectal examinations (DRE) and abnormal ultrasound findings. Patients using 5 α-reductase inhibitors and other benign prostatic hyperplasia (BPH) medications including a-blockers were excluded from the analysis.
Results: 390 patients were diagnosed with prostate cancer at an initial prostate biopsy. Patients being diagnosed with benign prostate hyperplasia were 590. IPSS (International prostate symptom score) was 9.7 and 10.2 in prostate cancer and BPH, respectively. There was no difference in obstructive symptoms and storage symptoms between prostate cancer and BPH.
Conclusion: The severity of voiding symptoms was not different between benign prostate hyperplasia and prostate cancer. Voiding symptoms should not be a decision tool for deciding prostate biopsy.
Key Words: Voiding symptom; Benign prostatic hyperplasia; Prostate cancer
책임저자 : 김영식
10444 경기도 고양시 일산동구 일산로 100 국민건강보험 일산병원 비뇨기과 전화 : (031)900-0550, 팩스 : (031)900-0343 E-mail : urokim@nhimc.or.kr
*본 연구는 국민건강보험 일산병원의 연구비 지원으로 이루어졌음 (임의연 2013-59).
서 론
많은 중년 남성은 나이가 들면서 전립선비대증 혹은 전립 선암과 같은 전립선 질환을 갖는다. 그러나 전립선비대증과 전립선암은 치료의 방법이나 예후가 전혀 다른 질환이다. 전 립선암 발생률은 남성암 중 2위를 차지하며, 피부암을 제외하 면 가장 흔한 암이다. 암으로 인한 사망원인으로는 폐암 다음 으로 2위를 차지한다1. 일반적으로 PSA가 정상 범위를 벗어 나면 전립선생검을 시행하여 전립선암 진단을 한다. 그러나, 전립선생검은 통증을 수반하는 매우 침습적인 검사다. 또한
전립선암 진단을 위한 PSA 선별검사에 대한 필요성에 대하여 도 이견이 많다. 하지만, 전립선비대증과 전립선암은 나타나 는 증상과 위험인자 측면에서는 겹치는 부분이 상당히 존재 한다. 그러나 전립선암 환자에서 나타나는 배뇨증상과 전립 선비대증 환자의 증상을 비교 분석한 자료는 많지 않다. 흔히 환자들은 배뇨증상이 심하면 전립선암이 있는 것은 아닌지 더 많은 걱정을 한다2,3. 그러나 증상의 심한 정도와 암의 연관 성에 대한 보고는 아직 없다. 이에 이 논문에서는 전립선암으 로 진단받은 환자에서 보이는 배뇨증상과 전립선비대증 환자 에서 보이는 배뇨증상의 양상을 직접 비교하여, 전립선암 환자 에서 비대증 환자에서 보이지 않는 특징이 있는지 알아보고 자 하였다.
대상 및 방법
1. 대상2006년부터 2013년까지 본원에 내원하여 경직장초음파
YS Kim. Comparison of Lower Urinary Tract Symptoms in Benign Prostatic Hyperplasia and Prostate Cancer
2 Medical Journal of National Health Insurance Service Ilsan Hospital Table 2. Comparison of IPSS in BPH and prostate cancer Benign prostate hyperplasia Prostate cancer
IPSS
Mild, % 45 47
Moderate, % 38 36
Severe, % 17 18
IPSS (International prostatic symptom scores)
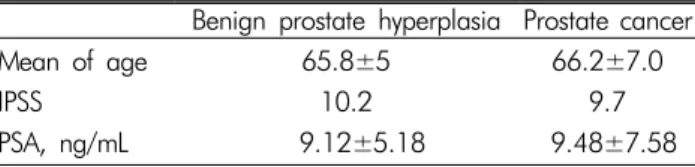
Table 1. Comparison between BPH and Prostate cancer Benign prostate hyperplasia Prostate cancer
Mean of age 65.8±5 66.2±7.0
IPSS 10.2 9.7
PSA, ng/mL 9.12±5.18 9.48±7.58
IPSS (International prostatic symptom scores)
촬영 유도하에 전립선생검을 받은 50세 이상 1,850명 환자를 대상으로 후향적 연구를 하였다. 조직 생검 전에 국제전립선 증상점수(International prostate symptom score)를 측정한 경우 를 대상으로 하였다.
2. 방법
전립선생검은 PSA(Prostate specific antigen) 4 ng/mL 이상 혹은 직장손가락검사에서 이상 소견이 보이는 환자를 대상으 로 하였다. 조직 생검은 경직장초음파 유도하에 10-12부위 또는 그 이상으로 하였다. 과거 급성요폐 병력이 있거나, 요도 관련 수술이나 전립선 및 직장수술을 받은 과거력이 있는 환 자는 제외하였다. 조직 생검 전에 알파차단제, 5알파환원효소 억제제, 항콜린제, 안드로겐 억제제, PED-5 억제제 및 desmo- pressin 약제를 복용한 환자는 제외하였다. 조직 생검에서 PIN (Prostatic intraepithelial neoplasia) 혹은 염증소견이 보이는 경우는 제외하였다.
3. 통계 처리
국제전립선증상점수가 0-7점을 경증, 8-19점을 중등도, 20-35점을 심한 증상으로 구분하였다. Student’s T-test를 이 용하여 통계적 유의성을 비교하였다.
결 과
전립선암으로 진단 받은 환자는 390명이었고, 양성 전립선 비대증 환자는 제외 대상을 제외하고 570명이었다. 전립선암 환자의 평균 나이는 66.2±7.0이었고, 전립선비대증 환자는
65.8±5으로 통계학적으로 유의한 차이는 없었다. 국제전립 선증상점수는 전립선암 환자가 9.7이었고, 전립선비대증 환 자는 10.2로 통계적 유의성은 없었다(Table 1). 전립선암 환자 의 경우는 경증이 47%, 증등도의 증상이 36%, 심한 증상은 18%였다. 전립선비대증 환자의 경우는 경증이 45%, 증등도 증상이 38%, 심한 증상은 17%였다. 두 군간에 차이는 보이지 않았다(Table 2).
국제전립선증상점수 중 폐색증상(obstructive symptom)과 저장증상(storage symptom)으로 구분하였을 때, 전립선비대증 환자에서는 각각 8.9±3.9, 4.9±2.5이었고, 전립선암 환자에서 는 8.7±2.5, 4.5±3.4였다. 두 군에서 차이를 보이지 않았다.
PSA는 전립선암 환자에서는 9.48±7.58 ng/mL이었고, 전 립선비대증 환자에서는 9.12±5.18 ng/mL로 유의한 차이는 없었다.
고 찰
본 논문에서는 전립선비대증 환자와 전립선암 환자에서 배뇨증상의 차이를 보이지 않았다. 그러나, PSA가 3 ng/mL 이상 증가된 환자에서 배뇨증상이 없는 경우에 전립선암이 발견되는 경우가 더 높았다는 역상관 관계를 보여주는 보고 도 있다4,5. 반대로 하부요로증상이 심할수록 전립선암이 발 견될 확률이 증가한다는 보고도 있다. 특히, 하부요로증상이 심할수록 국소전립선암 발견가능성이 높다고 하였다6.
전립선 크기가 크면서 배뇨증상이 없는 경우가 배뇨증상 이 있는 경우보다도 전립선암이 발견될 확률이 높다는 흥미 로운 보고도 있다7,8. PSA가 2.0-9.0 ng/mL인 경우 전립선 크 기가 작을수록 전립선암이 발견될 확률이 증가한다는 보고도 있다7. 이유는 전립선이 작은데 PSA가 상승한 경우는 상승의 원인이 전립선비대증 보다는 전립선암일 가능성이 더 높기 때문으로 생각한다. 그러나 나이가 들수록, 전립선의 크기가 클수록 PSA가 증가하고 배뇨증상이 나타날 가능성이 높아, 증상이 없는 환자보다 이런 환자에서 전립선암이 발견될 확 률이 높지 않은데 전립선생검을 하는 경우는 오히려 많아 불 필요한 조직 생검을 하게 되는 경우도 많다9,10. 전립선 크기가 크면 전립선암이 발견되는 확률이 낮은 것은 생검 시 샘플이 잘못되어 암 발견확률이 낮은 것은 아니다11. 실제 전립선 크 기가 큰 경우는 조직 생검을 다시 하였을 때 암이 발견되는 경우가 오히려 적고, 전립선 크기가 작은 경우에 생검을 다시 하였을 때 암이 발견되는 경우가 많아, 생검 시 샘플링의 문제 는 아닌 것으로 알려졌다12,13. 본 논문에서는 전립선 크기와의
김영식. 전립선비대증과 전립선암 환자에서 배뇨증상의 차이
Volume 16 Number 1 June 2017
3 관계는 데이터를 얻지 못하였다.
본 논문에서는 배뇨증상을 폐색증상과 저장증상으로 구분 한 경우도 전립선암과 전립선비대증 환자에서 유의한 차이가 없었다.
결론적으로 전립선비대증 환자와 전립선암 환자에서 유의 한 배뇨증상의 차이는 없었다. 또한 배뇨증상이 심하다고 하 여 전립선암이 더 많이 발견되지도 않았다. 따라서 배뇨증상 만으로 전립선 조직 생검 여부를 결정하기는 어려울 것으로 생각되며, PSA와 전립선 크기와 배뇨증상과의 연관성에 대한 보다 많은 연구가 필요할 것으로 생각된다.
REFERENCES
1. Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 2007;18(3):581-92.
2. Brown CT, O’Flynn E, Van Der Meulen J, Newman S, Mundy AR, Emberton M. The fear of prostate cancer in men with lower urinary tract symptoms: should symptomatic men be screened? BJU Int 2003;91(1):30-2.
3. ai T, Clements A, Bukach C, Shine B, Austoker J, Watson E. What influences men’s decision to have a prostate-spe- cific antigen test? A qualitative study. Fam Pract 2007;24(4):
365-71.
4. Frånlund M, Carlsson S, Stranne J, Aus G, Hugosson J.
The absence of voiding symptoms in men with a prostate- specific antigen (PSA) concentration of ≥3.0 ng/mL is an independent risk factor for prostate cancer: results from the Gothenburg Randomized Screening Trial. BJU Int 2012;
110(5):638-43.
5. Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, et al. Comparison of digital rectal exami- nation and serum prostate specific antigen in the early de-
tection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol 1994;151(5):1283-90.
6. Godley PA, Carpenter WR. Case-control prostate cancer screening studies should not exclude subjects with lower urinary tract symptoms. J Clin Epidemiol 2007;60(2):176- 80.
7. Al-Azab R, Toi A, Lockwood G, Kulkarni GS, Fleshner N.
Prostate volume is strongest predictor of cancer diagnosis at transrectal ultrasound-guided prostate biopsy with prostate- specific antigen values between 2.0 and 9.0 ng/mL. Urology 2007;69(1):103-7.
8. Stamey TA, Johnstone IM, McNeal JE, Lu AY, Yemoto CM.
Preoperative serum prostate specific antigen levels between 2 and 22 ng/mL. correlate poorly with post-radical prostatec- tomy cancer morphology: prostate specific antigen cure rates appear constant between 2 and 9 ng/mL. J Urol 2002;167(1):
103-11.
9. Matsubara A, Yasumoto H, Teishima J, Seki M, Mita K, Hasegawa Y, et al. Lower urinary tract symptoms and risk of prostate cancer in Japanese men. Int J Urol 2006;13(8):
1098-102.
10. Porter CR, Kim J. Low AUA symptom score independently predicts positive prostate needle biopsy: results from a raci- ally diverse series of 411 patients. Urology 2004;63(1):90-4.
11. Djavan B, Zlotta AR, Ekane S, Remzi M, Kramer G, Roume- guère T, et al. Is one set of sextant biopsies enough to rule out prostate Cancer? Influence of transition and total pros- tate volumes on prostate cancer yield. Eur Urol 2000;38(2):
218-24.
12. Zackrisson B, Aus G, Lilja H, Lodding P, Pihl C, Hugosson J. Follow-up of men with elevated prostate-specific antigen and one set of benign biopsies at prostate cancer screening.
Eur Urol 2003;43(4):327-32.
13. van Leeuwen P, van den Bergh R, Wolters T, Schröder F, Roobol M. Screening: should more biopsies be taken in larger prostates? BJU Int 2009;104(7):919-24.