접수일 : 2008 년 6 월 11 일 , 게재승인일 : 2008 년 7 월 17 일
책임저자 : 김준성 , 경기도 수원시 팔달구 지동 93
442-729, 가톨릭대학교 성빈센트병원 재활의학과
Tel: 031-249-7650, Fax: 031-251-4481 E-mail: [email protected]
Table 1. Pathological Conditions Detectable by Ultrasound Joints
Synovitis Bone erosion Osteophytes Subluxation Peri-articular soft tissue
Tenosynovitis
LHB tendon subluxation/dislocation Tendon tears
Tendinitis Tendinosis Calcification Bursitis
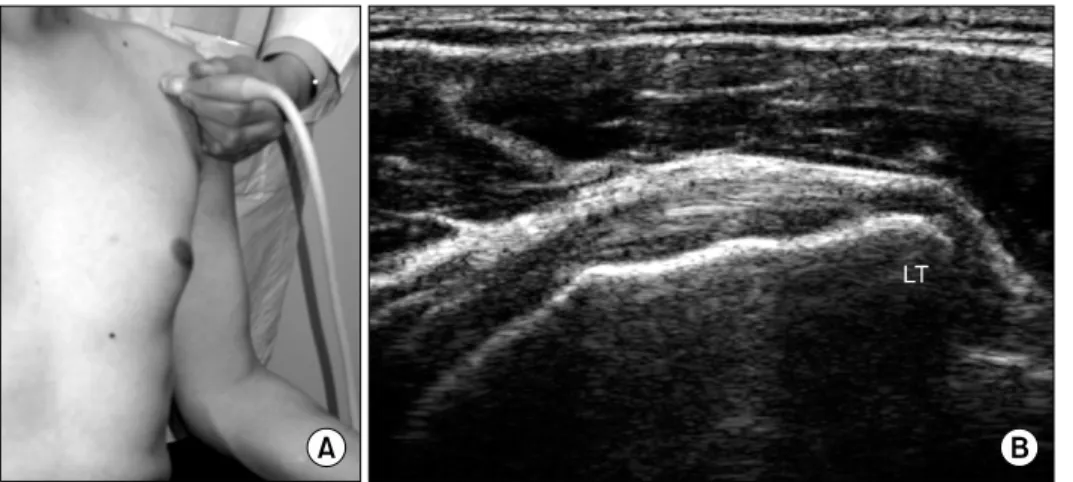
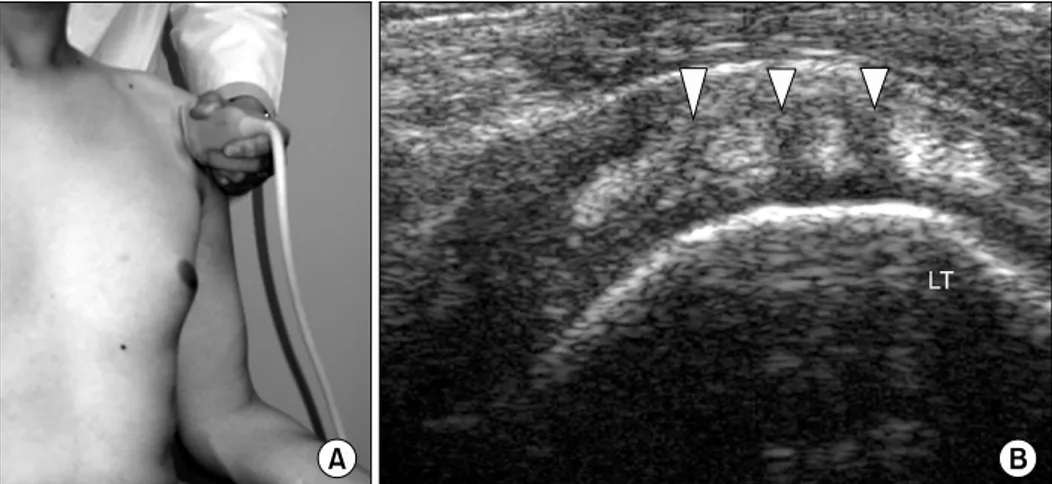
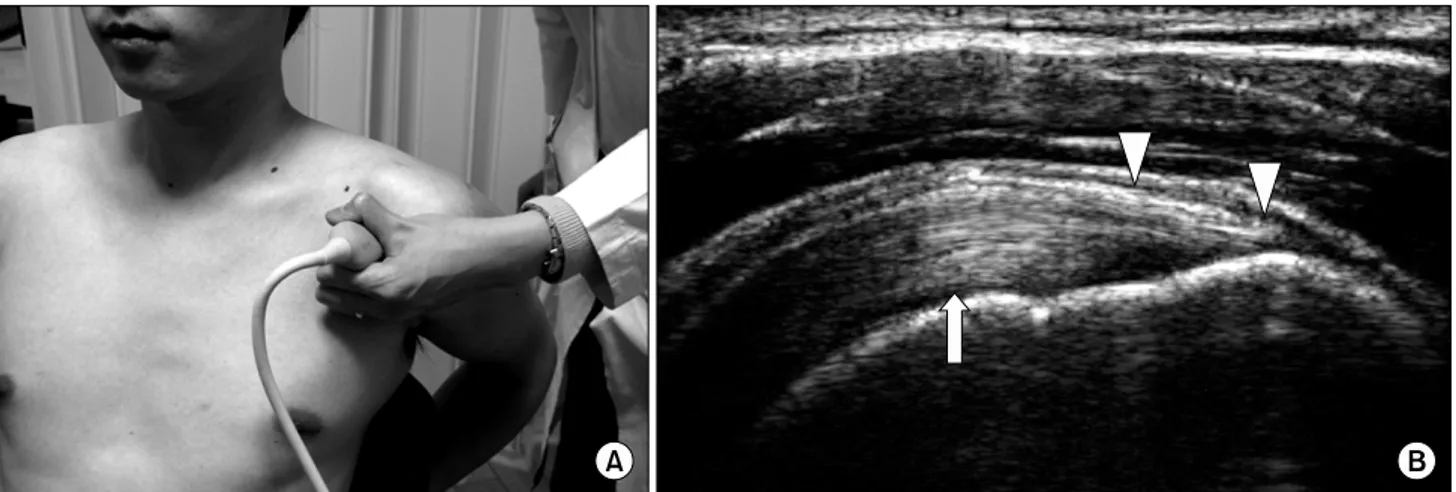
견관절의 정상 초음파 소견
가톨릭대학교 의과대학 성빈센트병원 재활의학교실
김 준 성