26
통신저자:이 광 복
전북 전주시 덕진구 금암동 634-18 전북대학교병원 정형외과
Tel:063-250-2586ㆍFax:063-271-6538 E-mail:[email protected]
접수: 2011. 7. 4 심사(수정): 2011. 7. 28 게재확정: 2011. 8. 20
Address reprint requests to:Kwang-Bok Lee, M.D., Ph.D.
Department of Orthopaedic Surgery, Chonbuk National University Hospital, 634-18, Geumam-dong, Deokjin-gu, Jeonju 561-712, Korea Tel:82-63-250-2586ㆍFax:82-63-271-6538
E-mail:[email protected]
하지 외상성 혈관 손상 환자에서
컴퓨터 단층 혈관 촬영술이 신뢰할 만한 진단 도구인가?
박종혁ㆍ이광복ㆍ박 혁ㆍ이준모
전북대학교 의학전문대학원 전북대학교병원 정형외과학교실, 임상의학연구소
목 적: 컴퓨터 단층 혈관 촬영술은 하지의 외상성 혈관 손상이 의심되는 환자에서 처음 실시하는 진단적 검사로 혈관 조영술을 대체하고 있다. 후향적 연구를 통해 컴퓨터 단층 혈관 촬영술의 임상적 신뢰도에 대해 연구하고자 한다.
대상 및 방법: 최근 2년간 하지 외상성 혈관 손상 환자에서 수술 전 컴퓨터 단층 혈관 촬영술을 시행했던 17명을 대상으로 하였고 모든 환자에서 수술 소견과 컴퓨터 단층혈관 촬영술을 비교 분석하여 양성 예측도 및 신뢰도를 분석하였다.
결 과: 전체 17명의 환자 중 16명은 혈관 손상, 1명은 구획증후군이었다. 16명의 혈관 손상 중 15명이 수술 전 컴퓨터 단층 혈관 촬영술과 수술소견이 일치하여 93.8%의 양성 예측도를 보였다. 후방 경골 동맥 손상 1명은 컴퓨터 단층 혈관 촬영술에서는 정상으로 보여, 전체 17명 중 15명에서 컴퓨터 단층 혈관 촬영술과 수술 소견이 일치하여 88.2%의 정확도를 보였다.
결 론: 외상성 혈관 손상이 의심되는 환자에서 컴퓨터 단층 촬영술은 진단적 가치가 높은 검사이지만 족관절 주위의 비교적 직경이
작은 혈관 손상이나 구획 증후군 환자의 경우는 정확도가 떨어지므로 혈관 조영술이나 진단적 탐색술 등의 보다 침습적인 검사가 필요할 것으로 생각된다.
색인 단어: 컴퓨터 단층 혈관 조영술, 외상성 혈관 손상, 선별검사
Is CT Angiography a Reliable Tool for Diagnosis of Traumatic Vessel Injury in the Lower Extremities?
Jong-Hyuk Park, M.D., Kwang-Bok Lee, M.D., Ph.D., Hyuk Park, M.D., Jun-Mo Lee, M.D., Ph.D.
Department of Orthopaedic Surgery, Chonbuk National Univeristy Hospital,
Research Institute of Clinical Medicine, Chonbuk National University Medical School, Jeonju, Korea
Purpose: Computed tomographic (CT) angiography is the first choice of diagnosis in traumatic vessel injury in the lower extremities, replacing angiography. The purpose of this study was to investigate the clinical reliability of CT angiography through a retrospective study.
Materials and Methods: Seventeen patients underwent CT angiography before surgery for traumatic vessel injury in the lower extremities from 2009 to 2010, and a comparative analysis of operative findings in all patients with a positive predictive value and sensitivity were measured.
Results: In all patients, 16 artery ruptures and 1 compartment syndrome occurred. In 15 artery ruptures, preoperative findings of CT angiography and surgical findings were consistent, and the positive predictive value was 93.8%. One patient with posterior tibial artery rupture was revealed as normal in CT angiography; thus, sensitivity was 93.8% (15/16 patients), and the accuracy rate was 88.2% (15/17 patients).
Conclusion: Though CT angiography is a reliable tool for diagnosis in traumatic vessel injury in the lower extremities, a more invasive test will be needed, especially peripheral angiography or diagnostic exploration, in cases of relatively small vessel injuries around the ankle or compartment syndrome because of low accuracy.
Key Words: CT angiography, Traumatic vessel injury, Screening test
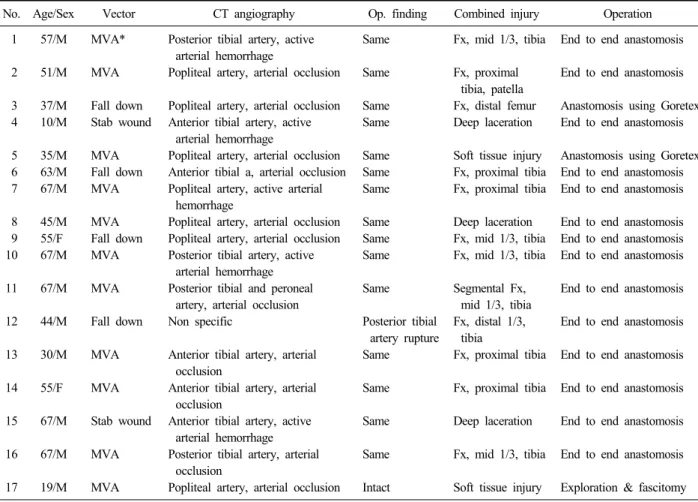
Table 1. Summary of cases
No. Age/Sex Vector CT angiography Op. finding Combined injury Operation
1
2
3 4
5 6 7
8 9 10
11
12
13
14
15
16
17 57/M
51/M
37/M 10/M
35/M 63/M 67/M
45/M 55/F 67/M
67/M
44/M
30/M
55/F
67/M
67/M
19/M
MVA*
MVA
Fall down Stab wound
MVA Fall down MVA
MVA Fall down MVA
MVA
Fall down
MVA
MVA
Stab wound
MVA
MVA
Posterior tibial artery, active arterial hemorrhage
Popliteal artery, arterial occlusion
Popliteal artery, arterial occlusion Anterior tibial artery, active
arterial hemorrhage
Popliteal artery, arterial occlusion Anterior tibial a, arterial occlusion Popliteal artery, active arterial
hemorrhage
Popliteal artery, arterial occlusion Popliteal artery, arterial occlusion Posterior tibial artery, active
arterial hemorrhage Posterior tibial and peroneal
artery, arterial occlusion Non specific
Anterior tibial artery, arterial occlusion
Anterior tibial artery, arterial occlusion
Anterior tibial artery, active arterial hemorrhage
Posterior tibial artery, arterial occlusion
Popliteal artery, arterial occlusion Same
Same
Same Same
Same Same Same
Same Same Same
Same
Posterior tibial artery rupture Same
Same
Same
Same
Intact
Fx, mid 1/3, tibia
Fx, proximal tibia, patella Fx, distal femur Deep laceration
Soft tissue injury Fx, proximal tibia Fx, proximal tibia
Deep laceration Fx, mid 1/3, tibia Fx, mid 1/3, tibia
Segmental Fx, mid 1/3, tibia Fx, distal 1/3,
tibia
Fx, proximal tibia
Fx, proximal tibia
Deep laceration
Fx, mid 1/3, tibia
Soft tissue injury
End to end anastomosis
End to end anastomosis
Anastomosis using Goretex End to end anastomosis
Anastomosis using Goretex End to end anastomosis End to end anastomosis
End to end anastomosis End to end anastomosis End to end anastomosis
End to end anastomosis
End to end anastomosis
End to end anastomosis
End to end anastomosis
End to end anastomosis
End to end anastomosis
Exploration & fascitomy
*MVA: motor vehicle accident.
서 론
컴퓨터 단층 혈관 촬영술은 현재 하지의 외상성 혈관 손 상이 의심되는 환자에서 비침습적인 방법으로 활용이 용이 하고 검사시간이 짧으며 진단의 정확도가 높아 응급실에서 처음 실시하는 진단적 검사로 혈관 조영술을 대체하고 있 다1,2). 또한 컴퓨터 단층 혈관 촬영술은 손상받은 혈관 주 위의 뼈와 연부 조직 손상에 대한 정보를 동시에 제공한다 는 장점을 가지고 있다13).
혈관 조영술은 혈관 손상의 확실한 증상을 보이지 않고 신체 검사상으로 정확한 진단이 힘든 환자에서 불필요한 진단을 위한 수술 시행 건수를 줄인다고 보고되고 있다6). 따라서 혈관 조영술은 검사 결과 정상인 경우가 더 많이 만, 시술 중에 적은 빈도에서 혈전 및 혈관 내막의 손상, 서혜부의 혈종 등 심각한 합병증이 발생될 수 있다6,8). 이 에 따라 최근의 추세는 비침습적인 검사인 컴퓨터 단층 혈 관 촬영술의 사용이 증가되고 있다.
많은 연구에서 컴퓨터 단층 혈관 촬영술이 높은 민감도
와 특이도를 보이고 있음을 보고하고 있다9,11,12). 그러나 저 자들은 몇 예의 문제 증례를 경험하게 되어 이를 통해 컴 퓨터 단층 혈관 촬영술의 한계점에 대해 보고하고자 한다.
대상 및 방법
2008년 2월부터 2010년 10월까지 이학적 검사상 하지 외상성 혈관 손상이 의심되어 컴퓨터 단층 혈관 촬영술을 시행했던 17명을 대상으로 하였다. 혈관 손상이 의심되는 경우는 맥박이 뛰는 출혈 (pulsatile bleeding), 혈종이 커 지는 경우, 맥박이 촉지되지 않을 때, 원위부의 허혈 증상 등이 확인될 때 컴퓨터 단층 혈관 촬영술을 시행하였다.
컴퓨터 단충 혈관 촬영술은 16-채널 다중행 탐지기 컴퓨터 단층 혈관 촬영기인 SOMATOM Definition (Siemens, Berlin, Germany)를 사용하였고, 조영제는 120 mL의 Iopromide 370 mg/mL (Ultrabist 370Ⓡ, Bayer, Toronto, Canada)을 사 용하였으며, 조영제 주사 후 약 10초 후에 컴퓨터 단층 혈 관 촬영을 시행하였다. 평균 나이는 39.2세 (min 10, max
Table 2. Positive predictive value and sensitivity of CT angio- graphy
Artery injury in operative finding (+)
Artery injury in operative finding (−) CT angiography (+)
CT angiography (−)
15 1
1 0
Fig. 1. Case 17.
(A) Plain radiogram shows the comminuted fracture on both femur and tibia shaft.
(B) CT angiography shows soft tissue and muscle swelling on femoral supracondylar area.
(C) CT angiography reveals the abrupt disruption of popliteal artery in the knee area, however, there is no vessel injury in intraoperative finding.
67)였고, 성별은 남자 11명, 여자 6명이었다. 사고 경위는 대부분 고에너지 손상에서 발생하였고, 12명의 환자가 교 통사고 후, 2명이 열상 후, 3명은 낙상 후 발생하였다. 12 명의 환자가 골절이나 탈구가 동반된 환자에서 발생하였고, 5명은 골절 없이 연부 조직 손상만 있었다 (Table 1).
17명 모든 환자에서 혈관 손상의 위치와 혈관 상태에 대해 시행한 컴퓨터 단층 혈관 촬영술과 수술소견을 비교 하여 양성 예측도 및 신뢰도를 분석하고, 위양성과 위음성 을 보인 증례를 보고하고자 하였다.
결 과
전체 컴퓨터 단층 혈관 촬영술을 시행한 17예 중 위양 성 1예, 위음성 1예로 컴퓨터 단층 혈관 촬영술의 정확도 (accuracy)는 88.2% (15예/17예)이었다 (Table 1).
컴퓨터 단층 혈관 촬영술을 시행한 결과 16예의 환자 중 11예에서 동맥 혈관이 폐색되었고, 5예에서 조영제가 혈관 밖으로 유출되는 활동성 출혈을 보여 동맥 혈관 손상 파열이 의심되었으며, 이 환자들 중 수술 소견상에서 슬와 동맥 파열 (popliteal artery rupture) 6예, 후 경골 동맥 파 열 (posterior tibial artery rupture) 4예, 전 경골 동맥 파 열 (anterior tibial artery rupture) 4예, 후 경골 동맥 과
비골 동맥의 파열 1예였다. 따라서 컴퓨터 단층 혈관 촬영 술의 양성 예측도는 93.8% (15예/16예)였다 (Table 2).
위양성을 보인 환자는 대퇴 간부의 골절과 동측에 경골 간부의 골절이 동반된 부유 슬관절 손상 환자로 신체 검사 상 하지의 맥박이 촉지되지 않아 컴퓨터 단층 혈관 촬영술 을 시행한 결과, 타박에 의해 과상부와 슬관절부의 연부조 직 및 근육의 부종이 관찰되었고 슬관절 후방부에서 조영 제가 급격히 단절되는 소견을 보여 슬와동맥 손상이 의심 되어 (Fig. 1), 응급으로 탐색술을 시행하였다. 수술 시야에 서 혈관 손상이 보이지 않아, 손상 의심부의 상 ․ 하 10 cm 까지 더 노출시켜 확인하였으나 역시 혈관 손상 없이 맥박 이 정상적으로 촉지되었다. 이것은 구획증후군에 의해 혈 관이 압박된 것으로 컴퓨터 단층 혈관 촬영술상 구획증후 군이 가장 심했던 부분에서 조영제가 급격히 단절된 것으 로 추정된다.
수술시야상에서 혈관 손상이 진단된 환자는 16예, 이 중 컴퓨터 단층 혈관 촬영술에서 혈관 손상 소견을 보인 환자 는 15예이었고, 컴퓨터 단층 혈관 촬영술에서 혈관손상이 의심되지 않았으나, 수술 소견에서 진단된 환자는 1예이었 다. 따라서 컴퓨터 단층 혈관 촬영술의 민감도는 93.8%
(15예/16예)였다 (Table 2).
위음성을 보인 환자는 경골 원위부 개방성 골절 환자로 족관절 후내측의 개방성 창상 및 족부의 부종이 동반되어 후방 경골 동맥 (posterior tibial artery)의 맥박을 정확히 촉지하기 힘들어 컴퓨터 단층 혈관 촬영술을 시행하였으나 조영제의 흐름 (patency)이 저하된 소견 외에 혈관 손상은 없는 소견을 보여 창상 치유만 시행하고 관찰하였다 (Fig. 2).
그러나 수상 일 주일 후에 족부의 괴사가 진행되어 혈관 조영술을 시행하였으며, 전방 및 후방 경골 동맥 파열 소 견이 보여 응급으로 혈관 접합술을 시행하였으나, 족관절
Fig. 2. Case 12.
(A) Plain radiogram shows comminuted ankle fracture.
(B) CT angiography shows that there is no definite vessel injury except the weak patency of dye in the posterior tibial artery.
부의 괴사가 진행되어 하퇴 표준 절단술 (BK amputation) 을 시행하였다.
고 찰
컴퓨터 단층 혈관 촬영술의 적응증은 응급실에서 활력징 후 (vital sign)가 안정적인 환자에서 즉각적인 수술을 시행 할 필요가 없는 경우 사지의 혈관 손상이 의심되는 모든 환자에게 시행하는 첫번째 검사로 받아들여지고 있다10). 즉각적인 수술을 필요로 하는 환자들은 활동성 출혈 (active hemorrhage)과 맥박 소실 (absent distal pulses)이 관찰될 경우 등이 있다.
컴퓨터 단층 혈관 촬영상에서 혈관 손상이 의심되는 소 견은 지속적 조영제 혈관외유출 (active contrast extrava- sation), 혈관외 조영제 결집 (extravascular contrast materi- al containing collection), 동맥 분절의 소실 (loss of opa- cification of an arterial segment), 급격한 혈관 협소 (abrupt vessel narrowing), 혈관내강의 조영 결핍 (intraluminal fill- ing defect) 등이 있다1). 컴퓨터 단층 혈관 촬영술은 여러 연구에서 외상성 혈관 손상의 진단 시 높은 신뢰도와 특이 도를 보고하고 있고3,11,12), 우리 연구에서도 역시 높은 신뢰 도 (93.8%)와 양성 예측도 (93.8%)를 보였다 (Table 2).
컴퓨터 단층 혈관 촬영의 결과 판독에 있어서 일반적으 로 혼란을 주는 요소들을 살펴보면, 혈관 안에 조영제의 전달이 불충분한 경우가 있고, 조영제 주사 후 CT촬영시간 이 정확한 시간에 이루어지지 않을 때 혈관의 영상이 정확 히 나타나지 않는 경우가 있다. 또한 혈관 손상 의심부위 보다 근위부에서 혈관 손상이 있는 경우 말단부의 진단이
어렵다. 다른 원인으로 혈관 경련 (vessel spasm), 해부학 적 변이 (anatomic variants), 죽상 경맥 동화증과 같은 기 저질환 (underlying atherosclerosis), 금속 등의 이물질에 의한 영상 오류 (artifact), CT 촬영 시 환자 자세의 불안정 등을 들 수 있다.
위양성 환자를 살펴보면 대퇴골 간부 및 경골 간부의 분 쇄골절이 동반된 부유 슬관절 (floating knee) 손상과 이로 인해 대퇴 과상부와 슬관절부의 연부조직 및 근육에 심한 타박상 및 부종이 광범위하게 관찰되었고, 컴퓨터 단층 혈 관 촬영상 슬와 동맥의 조영제가 급격히 단절 (abrupt dis- ruption)된 소견이 관찰되었으며, 이에 수술적인 탐색술로 혈관 손상 여부 및 혈전의 형성에 의한 혈관의 폐색을 확 인하여 손상혈관을 재접합하려 하였으나, 수술 소견에서 슬와동맥의 맥박은 저명하게 촉지되었고, 말단부인 배족부 동맥 (dorsalis pedis artery) 및 후경골 동맥 (posterior ti- bialis artery)의 맥박도 촉지되는 등 파열된 혈관 및 혈전 의 형성은 확인할 수 없었고, 또한 골절 부위와 슬와동맥 의 단절 부위가 달라 골편에 의한 혈관 압박 소견은 없었 다. 저자들의 생각으로는 술 전에 있었던 연부조직의 광범 위한 부종은 부유 슬관절 손상에 의한 구획 증후군으로 생 각되며, 이는 탐색술 과정에서 근막절개술 (fasciotomy)이 시행됨으로 인해 저절로 감소 및 감압된 것으로 생각된다.
이후 단계적으로 골절 치료 및 상처 봉합술을 시행하였다.
일반적으로 구획 증후군은 미세 혈관의 혈액 순환이 연부 조직의 부종에 의해 차단되어 발생하는 것으로 알려져 있 으며 원인으로는 골절, 연부조직이 손상, 혈관 손상 등이 가장 흔하다4,7). 구획 증후군의 진단은 임상증상이 가장 중 요하며 이외에 구획압을 측정하는것이 보다 중요하고 혈관 조영술 소견은 일반적으로 전체적인 동맥혈의 협착과 함께 혈액 순환이 저하된다8). 본 환자에서는 동맥의 조영제가 급격히 단절되었고, 이에 혈관 파열이나 혈전에 의한 혈관 폐색, 혈관 수축을 의심할 수 있었고, 본 환자에서는 혈관 파열이나 혈전에 의한 혈관 폐색을 확인할 수 없어 구획 증후군과 혈관의 수축이 동시에 발생되어 컴퓨터 단층 혈 관 촬영상 위양성 소견을 보인 것으로 판단된다.
위음성 환자를 살펴보면, 족관절 이하 부위에 골절이 동 반된 경우는 임상적으로 혈종이나 부종에 의해 후경골동맥 의 맥박을 신체검사로 확인하는데는 한계가 있다. 또한 컴 퓨터 단층 촬영 혈관 촬영상에서도 하지의 원위부 동맥혈 관은 혈액의 흐름이 느려서 혈관 차단부위를 확인 (runoff visualization) 하는데 한계점을 보이고 있다. 이러한 한계 점은 컴퓨터 단층 혈관 촬영의 소견으로 동맥혈관의 손상 에 있어서 수술적 치료 (응급 혈관 봉합술)를 결정하기 힘 들게 한다. 따라서 이렇게 작은 직경의 동맥 손상에 대한 검사로는 여전히 일반적인 혈관 촬영술 (conventional peri-
pheral angiography)을 시행하는 것이 바람직하다고 생각 된다5).
이 연구의 제한점은 컴퓨터 단층 혈관 촬영술의 민감도, 특이도 및 정확도를 정확히 분석하기 위해서는 컴퓨터 단 층 혈관 촬영술 소견상 정상이었던 환자들을 모두 침습적 인 혈관 조영술이나 탐색술을 시행하여 두 검사 방법을 비 교해야 하지만, 현실적으로 컴퓨터 단층 혈관 촬영술 상 정상으로 나온 경우 혈관조영술을 시행하는 것이 윤리적으 로나 경제적인 문제로 인해 검사를 진행하기 어려워 이러 한 후향적 검사로서 한계를 가지고 있어, 이에 대한 보완 연구가 필요하리라 생각된다.
결 론
외상성 혈관 손상이 의심되는 환자에서 컴퓨터 단층 촬 영술은 진단적 가치가 높은 검사이지만 족관절 주위의 비 교적 직경이 작은 혈관 손상의 진단이 어렵고 구획 증후군 환자의 경우 혈관 파열과 감별이 어려워 혈관 조영술이나 진단적 탐색술 등의 보다 정확한 검사가 필요할 것으로 생 각된다.
참 고 문 헌
1) Anderson RJ, Hobson RW 2nd, Lee BC, et al: Reduced dependency on arteriography for penetrating extremity trauma: influence of wound location and noninvasive vas- cular studies. J Trauma, 30: 1059-1063, 1990.
2) Bergstein JM, Blair JF, Edwards J, et al: Pitfalls in the use of color-flow duplex ultrasound for screening of sus- pected arterial injuries in penetrated extremities. J Trauma, 33: 395-402, 1992.
3) Busquéts AR, Acosta JA, Colón E, Alejandro KV, Rodríguez P: Helical computed tomographic angiography for the diagnosis of traumatic arterial injuries of the extremities. J Trauma, 56: 625-628, 2004.
4) Lee SJ: Posterior thigh compartment syndrome as a result
of pseudoaneurysm of the popliteal artery in the distal femoral fracture: a case report. J Korean Fracture Soc, 20:
277-281, 2007.
5) Miller-Thomas MM, West OC, Cohen AM: Diagnosing traumatic arterial injury in the extremities with CT angiog- raphy: pearls and pitfalls. Radiographics, 25(1 Suppl):
S133-142, 2005.
6) Pieroni S, Foster BR, Anderson SW, Kertesz JL, Rhea JT, Soto JA: Use of 64-row multidetector CT angiog- raphy in blunt and penetrating trauma of the upper and lower extremities. Radiographics, 29: 863-876, 2009.
7) Pyo YB, Shin DM, Kim PO: Treatment of acute com- partment syndrome with tibial fracture. J Korean Fracture Soc, 9: 614-621, 1996.
8) Reuss PM, Rosen RJ, Adelman M: Compartment syn- drome complicating lower extremity thrombolysis. J Vasc Interv Radiol, 10: 1075-1082, 1999.
9) Rieger M, Mallouhi A, Tauscher T, Lutz M, Jaschke WR: Traumatic arterial injuries of the extremities: initial evaluation with MDCT angiography. AJR Am J Roentgenol, 186: 656-664, 2006.
10) Shah N, Anderson SW, Vu M, Pieroni S, Rhea JT, Soto JA: Extremity CT angiography: application to trau- ma using 64-MDCT. Emerg Radiol, 16: 425-432, 2009.
11) Soto JA, Múnera F, Cardoso N, Guarín O, Medina S:
Diagnostic performance of helical CT angiography in trau- ma to large arteries of the extremities. J Comput Assist Tomogr, 23: 188-196, 1999.
12) Soto JA, Múnera F, Morales C, et al: Focal arterial in- juries of the proximal extremities: helical CT arteriography as the initial method of diagnosis. Radiology, 218: 188-194, 2001.
13) Uyeda JW, Anderson SW, Sakai O, Soto JA: CT an- giography in trauma. Radiol Clin North Am, 48: 423-438, 2010.