독소루비신과 아이포스파마이드로 치료한 폐전이 된 악성사구종양 1예
진원석ㆍ전인상
가천대학교 의학전문대학원 소아과학교실
A Case of Malignant Glomus Tumor on Shoulder with Pulmonary Metastasis Treated with Doxorubicin and Ifosfamide in a 10-year Old Girl
Won-Seok Jin, M.D. and In-Sang Jeon, M.D., Ph.D.
Department of Pediatrics, Graduate School of Medicine, Gachon University, Incheon, Korea
Malignant glomus tumor is an exceedingly rare neoplasm occurring in the soft tissues.
Controversy exists over whether malignant glomus tumor is a true malignancy due to the rarity of metastasis, however, this neoplasm has been known to show relatively fre- quent metastasis and poor outcome. To improve the outcome of systemic therapy for malignant glomus tumor might be necessary, but the appropriate chemotherapy or radio- therapy has yet to be elucidated. We report a case of malignant glomus tumor with multiple pulmonary metastases treated with total surgical resection and adjuvant chemo- therapy including doxorubicin and ifosfamide; however 7 months after completion of chemotherapy primary lung nodules increased. This case suggests that these chemo- therapeutic agents are not effective for the management of malignant glomus tumor with metastasis.
pISSN 2233-5250 / eISSN 2233-4580 http://dx.doi.org/10.15264/cpho.2016.23.1.65 Clin Pediatr Hematol Oncol 2016;23:65∼69
Received on January 30, 2016 Revised on March 1, 2016 Accepted on March 26, 2016
Corresponding Author: In-Sang Jeon Department of Pediatrics, Graduate School of Medicine, Gachon University, 24, Namdong-daero, 774 beon-gil, Namdong-gu, Incheon 21565, Korea Tel: +82-32-460-8382 Fax: +82-32-460-2362 E-mail: [email protected]
Key Words: Malignant glomus tumor, Chemotherapy
Introduction
The majority of glomus tumors are small benign neo- plasms assumed to stem from modified smooth muscle cells of a glomus body, an anatomic structure thought to play an important role in temperature regulation [1]. The in- cidence of glomus tumor is very low with an estimated rate of approximately 1% among soft tissue tumors [2]. Glomus
tumors rarely show aggressive features suggesting malig- nancy; an unresectable large mass and histological finding such as nuclear atypia, necrosis, and mitotic activity.
Despite exhibiting these features of malignancy, most ma-
lignant glomus tumors including glomangiosarcomas are
rarely known to metastasize [3]. As such, there has been
controversy regarding whether malignant glomus tumor has
a true malignant nature. However, a review of atypical and
malignant glomus tumors showed that 38% show malignant
Fig. 1. Thoracic spine MRI and lung CT. (A) T1 weighted sagittal image of the thoracic spine MRI showing a multi-lobulated and
irregularly branching mass from the upper margin at C3 to the lower margin at T6. (B) Lung view of chest CT showing small nodules on the left lung field. (C) Lung view of chest CT showing the metastatic nodule size in left and right lower lobes increased.features of being located within the dermis, show a size of greater than 2 cm, or exhibit malignant histology accom- panied by metastasis. Moreover, 75% of patients with meta- stasis died within 3 years after diagnosis [4]. Therefore, it seems that systemic therapy is required to improve the out- come of malignant glomus tumor. Surgical resection, how- ever, has been the mainstay of treatment and only a few cases have reported of chemotherapy use [5-8]. For its rarity it is not yet known whether adequate chemotherapy or/and radiotherapy is necessary.
We report a case of a malignant glomus tumor with lung metastasis in a 9-year-old girl who was treated with doxor- ubicin and ifosmamide. An increase in primary lung nodules was observed 7 months after completion of chemotherapy.
This case suggests that a systemic therapy should be applied to improve patient outcome of this rare neoplasm.
Case Report
A 10-year-old Russian Caucasian female visited a hospital in Russia for a mass on her right shoulder incidentally found during a checkup after a fall. She had no significant medical history except for some food allergies. Her grand- mother died from gastric cancer, and none of her other rel- atives had any significant medical history. Initial radiograph showed that she had no fractures, but a mass was found near her right scapula. She denied having any pain, tender-
ness, or sensory change on her shoulder area. Physical ex- amination showed a diffuse soft mass along the right bor- der of the scapula but cervical or axillary lymph node en- largement was not observed. Sonography showed that the mass measured approximately 5.6 cm in longest diameter and had a heterogeneous echogenicity. Given the history of trauma, the mass was initially thought to be a hematoma.
But after a few months’ observation, the size of the mass increased rather than decreasing, prompting additional imaging studies. Magnetic resonance imaging (MRI) showed that the mass was located on her back near the right scapula. The mass measured 11 cm (longitudinal length)×
4.5 cm (transverse length)×3 cm (depth) in size. There was no evidence of metastatic nodules in the lungs.
Incisional biopsy was performed to obtain a pathologic
diagnosis. The pathologic finding was suggestive of
sarcoma. At this point, she was transferred to our hospital
for further evaluation and treatment. Upon her visit to our
hospital, a thoracic MRI was performed, which showed a
large mass located between her scapulas and posterior to
the cervical and thoracic spines. The maximum length of
the mass was 14 cm, which extended from the upper mar-
gin of C3 spine to the lower margin of T6 spine. The trans-
verse diameter of the mass was 4.4 cm, and the thickness
was approximately 2 cm (Fig. 1A). Chest CT showed multi-
ple small nodules on both lungs (Fig. 1B). Additional imag-
ing studies, including bone scan, abdominopelvic CT, and
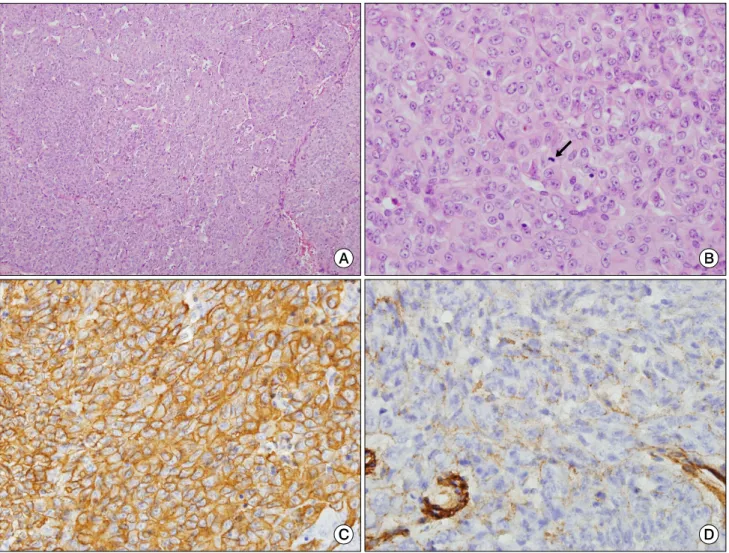
Fig. 2. Photomicrography of a malignant glomus tumor. (A) Solid sheets or trabeculae of tumor cells along with a prominent thin-walled
vascular network (H&E ×100). (B) Tumor cells have ovoid vesicular nuclei with prominent nucleoli. Mitosis (arrow) is seen (H&E×400). (C) Tumor cells are positive for smooth muscle actin (immunostain ×400). (D) Collagen type IV is positive in pericellular areas (immunostain ×400).