척추거대세포종에 대하여 전척추절제술 후에 구조성 동종골을 이용한 척주의 재건
가톨릭대학교 의과대학 정형외과학교실
강용구∙정양국∙유기원∙김기원∙강병민
제1 요추에 발생한 거대세포종을 전, 후방 도달법으로 제 1요추를 전척추절제술(total spondylectomy)로 종양을 광범위 절제하고, 추체 재건을 위하여 냉동(frozen) 보관된 구조성 대퇴 동종골 이식을 시행 한 후 장기 추시를 하여, 만족스러운 결과를 얻었기에, 그 결과를 보고한다.
색인 단어: 거대세포종, 전척추절제술, 구조성 동종골
Structural Allograft for Spinal Column Reconstruction after Total Spondylectomy for Giant Cell Tumor of the Spine
Yong-Koo Kang, M.D., Yang-Guk Chung, M.D., Kee-Won Rhyu, M.D., Ki-Won Kim, M.D., Byung-Min Kang, M.D.
Department of Orthopedic Surgery St. Vincent’s Hospital, The Catholic University of Korea
Giant cell tumor of the spine is very aggressive, thus spondylectomy for Enneking stage 3 giant cell tumor of the spine should be considered. After the resection of the tumor, autograft, structur- al cortical allograft or metallic implant (eg. cage or mesh cylinder) with autograft or allograft is used for reconstruction for the defect of spinal column.
Twenty nine year old lady who was diagnosed to Enneking stage 3 giant cell tumor in the first lumbar vertebra, was treated with total spondylectomy through anterior and posterior combined approach. For spinal column reconstruction, structural cortical allograft was used with anterior Z- plate and posterior CD instruments fixation. At 18 years follow-up, patient showed an excellent clinical results with well maintained spinal column with structural allograft. Anterior column reconstruction with structural cortical allograft proved to be a reliable technique in patients with aggressive spine tumors.
Key Words: Structural allograft, Spine, Giant cell tumor
� Address for Correspondence: Yong-Koo Kang, M.D.
Department of Orthopaedic Surgery, St. Vincent’s Hospital, The Catholic University of Korea, 93 Ji-dong, Paldal-gu, Suwon, Gyeonggi-do, 442-723, Korea
Tel : 82-31-249-7186, Fax : 82-31-254-7186, E-mail : [email protected]
서 론
척추 종양의 광범위 절제술 후에 결손된 척주(
spinal column)의 성공적인 재건은 종양의 재발 여부와 함께 종양치료의 성공적인 결과를 얻는데 필 수적인 과정이다.1-5)
종양의 재발 방지를 위하여 척추체를 완전히 제거 하는 전척추절제술(total spondylectomy)을 시 행하는 경우에 척주를 안전하게 재건하기 위한 방법 으로 결손된 척추체에 자가골 이식, 동종골이식, 금 속 케이지(cage) 혹은 타이타늄 격자형원통(tita- nium mesh cylinder) 등의 금속보형물(metal implant)을 이용하는 방법 등이 있는데, 자가골 이 식은 공여부의 제한으로 작은 결손 례에는 가능하지 만 큰 결손 증례에서는 어려움이 있다. 또한 금속보 형물은 다양한 크기가 있어 선택이 용이하지만, 수 술 후, 장기 추시하는 경우 금속과 생체조직(bio- logic tissue)인 뼈와의 부조화을 예상 할 수 있고, 노년이 되어 골다공증이 발생하였을 때, 삽입된 금 속보형물이 어떠한 역할을 할지 예측하기가 어렵다 는 단점이 있다. 반면에 구조성 피질 동종골(
structural cortical allograft)은 생체조직으로, 이식 후에 일단 생착(incorporation)이 되면 장기 간 사용이 가능하다는 장점이 있는 것으로 알려지고 있다.6,2,7)
저자는 제1 요추에 발생한 거대세포종을 전, 후방 도 달 법 으 로 제 1요 추 를 전 척 추 절 제 술 (total spondylectomy)로 종양을 광범위 절제하고, 추체 재건을 위하여 냉동(frozen) 보관된 구조성 대퇴 동종골 이식을 시행 한 후 장기 추시를 하여, 만족스 러운 결과를 얻었기에, 그 결과를 보고한다.
증 례
29세 여자 환자가 수개월 전부터 시작된 요통, 요 추 운동제한과 양측 하지 방사통을 주소로 내원하였 다. 동통은 최근에 심해져 등을 구부릴 수 없고, 대소 변 볼 때 힘을 줄 수도 없다고 호소하였다. 과거력이 나 가족력에 특이한 병력은 없었다. 입원 후에 시행 한 신체검사에서 척추를 구부리거나, 신전, 좌우 굴 곡이 심하게 제한되었으며, 우측 하지의 근력은 정 상이었으나, 좌측 하지의 운동력 즉, 고관절, 슬관절,
Fig. 1. Twenty nine year old lady with severe back pain and limitation of motion of spine was referred to the hospital.
Plain L-spine x-rays show vertebral body collapsed in L 1 vertebra and mild paralytic ileus of abdomen.
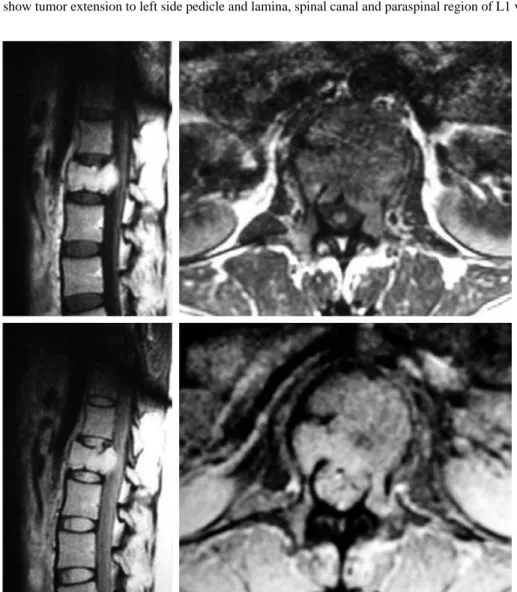
Fig. 2. CTs show tumor extension to left side pedicle and lamina, spinal canal and paraspinal region of L1 vertebra.
Fig. 3. MRIs show collapsed L1 vertebral body, and dural sac around L1 vertebra was surrounded and compressed by tumor.
족관절 및 족지의 근력이 3-4등급으로 약화 된 것을 인지 할 수 있었다. 흉요추 단순 방사선 검사에서 장 (bowel)운동이 저하되어 경도의 장 폐쇄(ileus) 소 견이 인지되었으며, 제1 요추에 경도의 압박 소견이 인지되었다(Fig. 1). 혈액검사에서 특이소견은 없었 다. 요추 컴퓨터단층영상(CT) 검사에서 제1 요추의 추체와 좌측 척추경을 침범하는 종양이 인지되었는 데, 종양이 척추강으로 확산되어 척수를 심하게 압 박(Fig. 2)하는 것을 확인 할 수 있었다. 골주사 (bone scan) 검사에서는 제 1요추의 동위원소 침착 이 증가하였으나, 제1요추 이외의 이상 소견은 발견 되지 않았다. 자기공명영상(MRI) 영상에서 T1에서 저음영(low signal), T2에서 고음영의 종양이 제1 요추 척추체 와 좌측 척추경, 척추강, 척추체 밖으로 확산되고, 척수를 압박하였으며, 전이암보다는 원발 성 악성종양이나 악성에 준하는(aggressive) 종양 을 의심하게 하였다(Fig. 3). 영상의학과와 협진으 로 컴퓨터단층영상 이용한(CT guided) 생검으로 종양은 거대세포종으로 진단되어, Enneking 병기
분류 제 3형으로 판단하였으며, Tomita 척추종양 병기 분류8)제 5형 로 평가하였다.
전척추 절제술(total spondylectomy)을 계획 하여, 먼저 후방도달법으로 후방구조물인 후궁과 극 돌기을 제거하고, 제 11흉추에서 제3 요추에 CD 고 정기구를 삽입하여 후방 구조물을 안정화시키고, 당 일 전방도달법으로 10번째 늑골을 제거하고, 횡격막 을 절개하여, 경흉막, 후복막 도달법(transpleural, retro-peritoneal approach)으로 제11 흉추에서 제3 요추를 노출시키고, 제1 요추의 추체(body)를 한 덩어리로 제거하였다. 종양의 완전 절제 후에 척 주(spinal column)을 재건하기 위하여 동결보관 (frozen)된 원주 모양의 대퇴골 동종골(femoral cortical allograft)을 척추 결손 길이에 맞게 재단 하고 절단하여, 제12 흉추와 제2요추 사이에 끼워 위치시키고, Z-금속판(plate)와 나사못을 이용하 여 제12 흉추와 제 2 요추를 고정하여 전방을 안정 화시키고, 횡격막을 봉합하고, 흉곽 내와 후복막 수 술창에 도관을 삽입하고 수술을 마무리 하였다
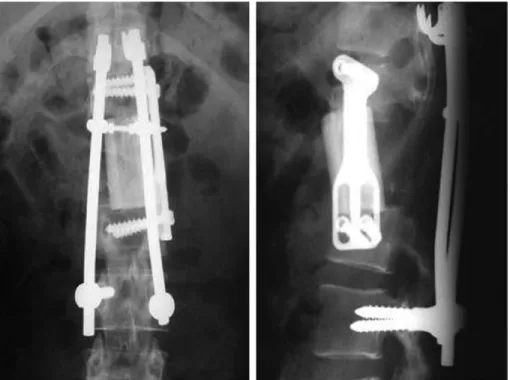
Fig. 4. Post operative x-rays show total spondylectomy with structural allograft fixed with Z-plate and CD instru- ments from D11 to L3 vertebrae.
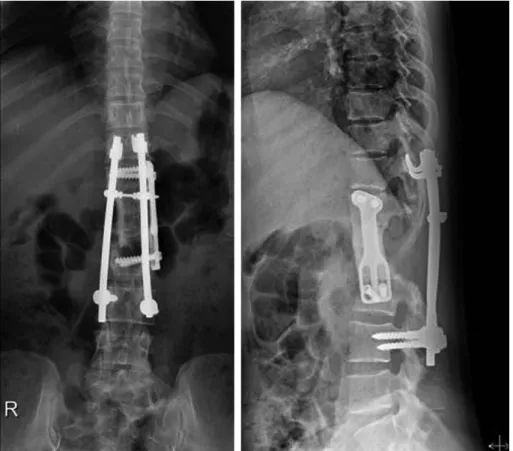
(Fig. 4). 수술 후에 환자는 특별한 합병증 없이 회 복되었으며, 신경학적 증상도 회복되었다. 수술 약 1 개월 후에 환자는 원래의 직업으로 복귀하였으며, 수술 후 현재 18년이 경과하였으며, 이식된 동종골 은 골흡수(bone resorption)나 동종골의 골절없이 척추체의 역할을 잘 수행하고 있으며, 척추 안정화 를 위하여 고정 중인 Z- 금속판, CD 기구(instru- ment) 등도 잘 유지 되고 있다(Fig. 5). 환자는 일 상생활에 아무런 제한 없이, 원래의 직장에서 근무 중이다.
토 론
척추 거대세포종의 수술적 치료에서 국소 소파술 (curettage)을 시행하는 경우에는 재건술에 어려 움이 없으나, 재발 방지를 위한 추체절제 혹은 추체
전적출술(total spondylectomy) 후에는 척추체 (vertebral body)에 대하여 완고한 재건이 필수적
이다.6,1,2,9) 척추의 거대세 포종이나 악성 종양의 치
료에서 국소재발을 예방하는 것은 일차적인 과제인 데, 재발 방지를 위한 광범위 절제 후에는 재건술의 어려움이 남는다. 척추체의 복원을 위하여 자가 장 골이식, 금속보형물인 금속 케이지(metal cage), 타이타늄 격자원통(titanium mesh cylinder)와 자가 혹은 동종해면골의 혼합이식의 방법이 흔히 이 용되는데, 추체의 부분 절제 시에는 자가 장골(iliac bone) 골이식 만으로도 가능하지만, 추체의 전적출 (total spondylectomy) 후에는 자가골 이식만으 로는 어렵다. 그리하여 임상에서는 자연스럽게 금 속게이지 혹은 금속원통 을 이용하게 된다.7,3-5)
Matsumoto 등10)(2011)은 전척추절제술(total en bloc spondylectomy)에 대한 척추재건술 후에
Fig. 5. Last follow-up x-rays at post-operative 18 years show well maintained Z-plate and CD instruments with remodelling of structural allograft to host vertebral bone.
평균 42개월 추시에서 약 40%의 환자에서 척추고정 술의 실패를 보고하며, 케이지 침강(subsidence), 수술 전 방사선조사(preoperative irradiation), 4 개 이상의 척추체 고정, 종양의 국소 재발 등이 원인 이었다고 보고하며, 실패 양상은 척추고정봉(rod) 의 골절(breakage), 케이지 골절(breakge) 등이었 다고 보고하였다. 이와 같이 금속보형물의 이식은 많은 례에서 생체조직과의 부조화에 따른 합병증이 빈발한 문제점으로 지적되고 있다.
한편, 구조성 동종골(structural allograft)이식 은 장관골의 골간부 피질골을 이용하므로 기계적 강 도가 척추체와 유사하게 강하고, 동종골은 금속과 달리, 생체조직(biologic tissue)으로 한번 생착이 되면 장기간 추시 할 때 재형성(remodelling) 이 기대되어, 장기 사용이 가능하고, 추체의 결손 크기 와 길이에 맞게 재단하고(tailoring), 절단하여 이 식할 수 있다는 장점이 있다.11)
2003년 Faro 들은 송아지 척추뼈를 이용한 생역 학 실험으로 척추체 절제 후 구조성 동종골의 이식 시에 전방의 금속판고정을 보강하면 이식골 생착에 도움이 된다고 보고하였다.12)또한 Lewandrowski 등은 30예의 원발 혹은 전이성 척추종양환자의 척추 적출술 후에 93%의 환자에서 6개월 이내에 동종골 의 유합을 얻었다고 보고하였다.3)그러나 이들의 보 고는 환자의 중간 생존(median survival)이 14개 월로 대부분의 환자들이 장기 생존하지 못하여 이식 후 생착한 동종골의 장기 추시 결과를 알 수 없었다.
본 증례는 제1요추의 거대세포종이 확산되어, Enneking 병기분류 3형, Tomita 척추종양 병기 분류 제5기로 국소 소파술로는 완전한 종양절제가 불가능하여, 전적출술(total spondylectomy)이 필요하였는데, 제1 요추를 완전히 제거한 후에 구조 성 동종골 이식으로 척주를 재건하였다. 수술전 사 전 계획 수립 시에 자가골 이식이나 케이지 삽입으 로는 안정된 척주 재건이 불가능하다고 판단하였고, 다만 타이타늄 격자원통을 삽입하여 재건하거나, 구 조성 동종골 이식으로 재건하는 방법 중에서 선택하 여야 하는 상태이었다. 저자들은 구조성 동종골이식 과 전, 후방 고정술로 보강하는 방법이 더 완고하고, 효과적인 재건술이 될 것으로 기대하고 수술을 시행
하였으며, 환자는 수술 후 18년 추시하는 동안 특별 한 합병증 없이 만족스러운 치료 결과를 보였다.
결 론
제1요추의 거대세포종을 전척추절제술로 제거한 후에 척주를 재건하는데, 동결보관(frozen) 구조성 피질 동종골(structural cortical allograft)을 이 용하여 척추체를 복원하고, 척추 고정기기를 보강하 여, 장기간의 추시에서 비교적 만족스러운 임상 결 과를 얻었기에 보고한다.
참고문헌
01. Boriani S, Saravanja D, Yamada Y, Varga PP, Biagini R, Fisher CG. Challenges of local recur- rence and cure in low grade malignant tumors of the spine. Spine. 34(22 suppl):s48-57.
02. Chung JY. Spinal tumor. J Korean Spine Surg.
2009, 6(2);316-25.
03. Lewandrowski KU, Hecht AC, DeLaney TF, Chapman PA, Hornicek FJ, Pedlow FX.
Anterior spinal arthrodesis with structural cortical allografts and instrumentation for spine tumor surgery. Spine 2004, 15;29(10);1150-8.
04. Rao G, Suki D, Chakrabarti I, Feiz-Erfan I, Mody MG, McCutcheon IE, Gokaslan Z, Patel S, Rhines LD. Surgical management of primary and metastatic sarcoma of the mobile spine. J Neurosurg Spine 2008, 9(2);120-8.
05. Yamazaki T, McLoughlin GS, Patel S, Rhines LD, Fourney DR. Feasibility and safety of en bloc resection for primary spine tumors: a system- atic review by Spine Oncology Study Group.
Spine 2009, 15;34(22 suppl):S31-8.
06. Boriani S, Bandiera S, Casadei R, Boriani L, Donthineni R, Gasbarrini A, Pignotti E, Biagini R, Schwab JH. Giant cell tumor of the mobile spine: a review of 49 cases. Spine. 2012. 37(1):
E37-45.
07. Kandziora F, Schnake KJ, Klostermann CK, Haas NP. Vertebral body replacement in spine
surgery. Unfallchirurg. 2004. 107(5):354-71.
08. Tomita K, Kawahara N, Murakami H. Primary and metastatic tumors of the spine; total en bloc spondylectomy. In Malawer M, Wittig JC, Bickels J. Ed. Operative techniques in orthopedic surgical oncology. p 152-160, Wolters Kluwer/Lippincott Williams&Wilkins, 2012.
09. Kang Y-K, Rhyu K-W, Rhee S-K, Bahk W-J, Chung Y-G, Park C-G. Surgical treatment of giant cell tumor of the spine. J Korean Bone Joint Tumor Soc. 2009, 15(2);135-42.
10. Matsumoto M, Watanabe K, Tsuji T, Ishii K, Nakamura M, Chiba K, Toyama Y. Late instru-
mentation failure after total en bloc spondylecto- my. J Neurosurg Spine 2011, 15(3):320-7.
11. Huang P, Gupta MC, Sarigul-Klijn N, Hazewood S. Two in vivo surgical approaches for lumbar corpectomy using allograft and a metallic implant: a controlled clinical and biomechanical study. Spine J. 2006. 6(6):648-58.
12. Faro FD, White KK, Ahn JS, Oka RS, Mahar AT, Bawa M, Farnsworth CL, Garfin SR, Newton PO. Biomechanical analysis of anterior instrumentation for lumbar corpectomy. Spine 2003, 15;28(22);E468-71.