Abstract
Implant placement for the upper anterior teeth is difficult compared to the posterior teeth, therefore careful consideration by the dental practitioner is necessary. To achieve successive implant placement, it is very important to place the implant fixture in the proper position.
An implant prosthesis connected to a properly placed implant fixture can be expected to yield good results with regard to function as well as aesthetics. On the contrary, improper positioning of an implant can result in an unaesthetic, non-functional and weak implant with no bite force. In this case report, the upper central incisor was extracted due to severe root resorption and was restored with a dental implant.
During the surgery, the implant placement was performed with a computer guided stent. After surgery, the aesthetics of the gingiva was adjusted and improved with a provisional restoration. Finally, additional gingival plastic surgery and gingival bleaching was performed and successful aesthetic treatment of the Maxilla central incisor was accomplished. With this case report, we hope to determine the position of implant fixture for functional and aesthetically ideal prosthesis implants and to evaluate the use of computer guided stents to promote the positioning of implants.
Key Words: central incisor, computer guided stent, dental implant, implant location, root resorption
양측 상악 중절치 임플란트 수복 시 Computer Guided Surgical Stent의 이용
이강희1, 김기덕2, 김근희2, 김민유1, 박원서1
1연세해담치과, 2연세대학교 치과대학 통합진료학과
The Use of Computer Guided Surgical Stent in Dental Implant of Maxilla Central Incisor
Kang-Hee Lee1, Kee-Doeg Kim2, Keunhee Kim2, Minyu Kim1, Wonse Park2
1
Yonsei Haedam Dental Clinic, Seoul, Korea
2
Department of Advanced General Dentistry, Yonsei University College of Dentistry, Seoul, Korea
ISSN 1229-5418 Implantology 2016; 20(2): 72~79
Reprint requests: Wonse Park
Department of Advanced General Dentistry, Yonsei University
College of Dentistry, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea Tel: 82-2-2228-8980, Fax: 82-2-2227-8906
E-mail: [email protected]
Received for publication: June 17, 2016 Revised for publication: June 21, 2016 Accepted for publication: June 22, 2016
교신저자: 박원서
(03722) 서울시 서대문구 연세로 50-1 연세대학교 치과대학 통합진료학과
Tel: 82-2-2228-8980, Fax: 82-2-2227-8906 E-mail: [email protected]
원고접수일: 2016년 6월 17일 원고수정일: 2016년 6월 21일 게재확정일: 2016년 6월 22일 Copyright © 2016. The Korean Academy of Oral & Maxillofacial Implantology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits
이 불가피한 경우가 대부분이었다.
Computer guided surgical stent는 1990년대 소개된 이 후 계속적인 기술 개발에 힘입어 정확도와 편의성이 점 점 개선되어 가고 있는 기술이다. 또 cone-beam com- puted tomography (CBCT), laser scanner, three- dimensional (3D) printer 같은 주변 기기의 보편화에 힘 입어 대중성을 얻어가고 있다. 수년 전만 해도 외국 유명 임플란트 회사들만이 서비스를 제공하였기 때문에 고비 용, 제작 기간 소요, 언어 소통의 어려움 등의 문제로 접 근성이 떨어졌지만 최근에는 국내 유수 임플란트 회사들 뿐 아니라, computer guided surgical stent만을 제작하 고 지원하는 전문 업체들이 점점 늘어가고 있는 추세이 다. Computed tomography (CT) 촬영으로 얻어진 환자의 3D skull model 상에서 진단, 계획하여 제작된 computer guided surgical stent를 이용하면 실제 골의 위치와 계획 된 임플란트의 위치가 같아 위와 같은 문제를 해결할 수 있다. 또 주변 치아와의 간격, 잔존 협측골의 두께를 고 려할 수 있을 뿐 아니라 식립 깊이 조절을 통해 제작될 보철물의 출현치은변연(emergence profile)의 두께와 각 도, 치은낭의 깊이까지도 조절할 수 있다는 장점이 있다.
본 연구는 computer guided surgical stent를 이용해 상 악 중절치(#11, #21)를 회복한 증례를 통해 스텐트의 유용 성을 평가하고, 심미적이고 기능적인 전치부 임플란트 치료를 위해 정확한 임플란트의 위치가 가지는 중요성을 논의하고자 한다.
II
증례보고2004년 10월 12일 의과적 병력이 없는 16세 남성 환자 가 상악 중절치가 아래로 내려온다는 것을 주소로 연세
I
서론임플란트는 상실된 치아를 대체하는 인공치아로 서 그 기능과 안정성을 인정 받아, 고정성 보 철 치료를 대체하는 훌륭한 대안으로 인정 받 고 있다1,2. 하지만 임플란트는 수술적 처치가 필요하며, 치조골의 형태와 치은의 성상에 따라 술 후 결과에 제한 을 받는다3. 또 식립 시에 임플란트가 이상적인 위치에 식립되지 않으면 차후 보철이 올라가는 과정에서 어느 정도 보완을 한다 하여도 원하는 결과를 얻기 어려울 수 있다는 단점이 있다. 적합하지 않은 위치에 식립된 임플 란트 치료는 치간부 음식물 함입, 치은 염증, 임플란트- 골 계면의 응력, 교합력 분산 실패 등을 발생시킨다. 전 치부에서는 기능적인 문제 외에도 비심미적인 치아 형태 와 치은 변연, 비정상적인 치아 비율과 간격 등의 심미적 문제를 일으킨다4. 따라서 보철물의 기반이 되는 임플란 트를 이상적인 위치에 식립하는 것은 심미보철, 연조직 형성, 유지관리 등 추후 모든 치료를 성공적으로 진행함 에 있어 매우 중요한 과정이다.
임플란트를 정확한 위치에 심기 위한 노력은 여러 방 식으로 시도되어 왔다. 가장 보편적인 방식은 치아가 상 실된 악궁을 인기한 석고 모형 상에 레진 인공치나 왁스 모형 등을 위치시킨 뒤, 배열된 치아의 축을 따라 드릴 삽입로를 설정하고 아크릴 스텐트를 제작하여 수술 시 보조 장치로 사용하는 것이다. 하지만 이러한 방식의 수 술 스텐트는 치조골의 실제 위치를 모르는 상태에서 계 획하고 제작된다. 그러므로 이 스텐트를 이용해 수술하 게 되면 계획한 임플란트의 위치와 실제 치조골의 위치 가 달라서 치조골의 열개, 천공, 고정 실패 등의 문제가 발생하고, 따라서 수술 중 술자의 역량으로 대량의 수정
Case Report
대학교 치과병원에 내원하였다. 주소 치아는 수년 전 외 상에 의한 탈락과 재식립 병력이 있었다. 치근 외흡수 소 견이 보여 근관치료 후 5년간 경과 관찰을 하였으나 외흡 수가 멈추지 않고 계속하여 진행되는 것이 관찰되었고, 따라서 주소 치아 발치와 교정을 동반한 임플란트 처치 가 추천되었다(Fig. 1). 발치 후 교정 치료를 진행할 경우 교정 치료 기간 동안 발치 부위의 치조골, 특히 순측골의 흡수 가능성이 높기 때문에, 치조골을 유지하기 위하여 상악 좌우 중절치의 발치를 가능한 한 연기하면서 교정 치료를 우선 시행하였고, 임플란트는 악골 성장이 완료 되는 만 20세 이후 식립하는 것을 계획하였다.
교정을 통해 상하악 치아를 배열하면서 상악좌측중절 치(#21; 2011. 11. 7), 상악우측중절치(#11; 2012. 7. 31) 발 치를 순차적으로 시행하였다. 침윤마취(lidocaine 2%, 1:100,00 epinephrine)하에 발치를 시행하였으며 순측골
의 흡수를 최대한 예방하고 치조골 재형성을 돕기 위해 서 발치와 내의 육아 조직을 소파한 후, collagen matrix (Teruplug; Olympus Terumo Biomaterials, Tokyo, Japan)를 넣고 봉합하였다. 발치된 치아는 백악질과 상
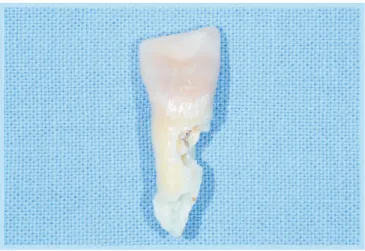
Fig. 1.
Maxilla cental incisor of 21-year-old man. Therewas the past trauma history, and root canal therapy was done. But severe external root resoprtion can be observed. The treatment plan is extraction of central incisor and implant surgery at this site after Orthodontic treatment of adjacent teeth.
Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant of Maxilla Central Incisor. Implantology 2016
Fig. 2.
Extracted right maxilla central incisor (#21), severe external root resorption extended to cementum, dentin and pulp canal can be seen.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant of Maxilla Central Incisor. Implantology 2016
Fig. 3.
The occlusal view of extracted central incisor after 1 year of orthodontic treatment. At the same time of extraction, socket preservation with collagen matrix was done but narrow alveolar bone was seen due to buccal bone resorption.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant
of Maxilla Central Incisor. Implantology 2016
아질을 포함하여 치수관을 침범하는 흡수 양상을 보였고 (Fig. 2), 외흡수 요인 평가를 위해 발치 부위 조직생검실 험을 의뢰였으나 특이 소견을 발견할 수 없었다.
이후 교정 처치 마무리를 진행하였고, 2013년 8월 12일 임플란트 식립을 위한 CT 촬영과 구강 검사를 시행하였 다. 검사 결과 순설측 치조골 흡수로 폭경이 좁아 심미적 보철치료가 어려울 것으로 예상되었다(Fig. 3, 4). 치조 골의 재형성과 정교한 임플란트 식립을 위해서 동종골과 흡수성 차폐막을 사용하는 골유도 재생술을 동반한 computer guided implant surgery를 계획하였다.
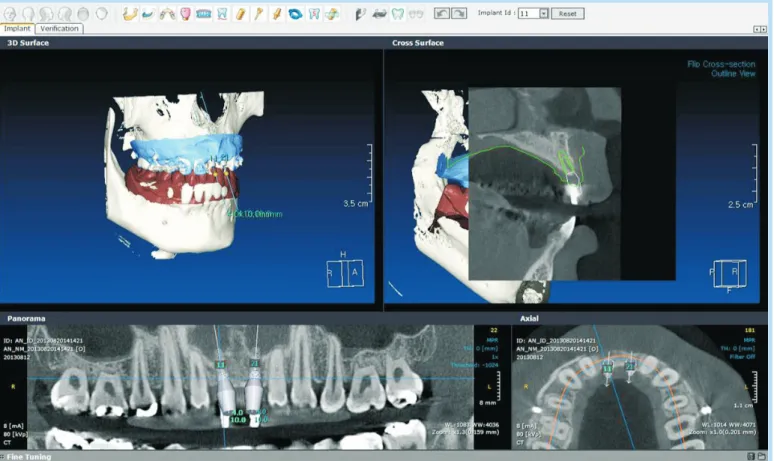
In2Guide program (CyberMed, Seoul, Korea)을 사용 하여 CT로 얻은 3D skull model 상에 implant surgery planning을 하였다(Fig. 5). 계획된 임플란트는 수직적으 로 인접치의 cement-enalmel junction보다 1 mm 하방에
implant coronal top이 위치하며, 협설로 치조골을 벗어 나지 않고 1 mm 구개측에 위치하여 순측으로 충분한 치 조골과 치은을 남겨야 자연스러운 치은 형태를 얻고 이 후 saucerization을 예방할 수 있다4. 3D printer로 아크 릴 재질의 computer guided surgical stent를 제작하였다 (Fig. 6).
2013년 9월 26일, In2Guide surgical stent (CyberMed) 를 사용하여 임플란트(Dentium superline FX4010SE;
Dentium, Seoul, Korea)를 식립하였고, 식립 부위 순측 치조골 흡수가 예상되는 부위에 동종골과 흡수성 차폐막 을 사용하여 골이식을 시행했다(Fig. 7).
2013년 11월 29일, 식립체와 지대주를 연결하기 위한 임플란트 2차 수술을 시행했으며, 동시에 레진 임시 치관 을 장착하여 환자의 심미성과 기능성을 회복하였고 치은
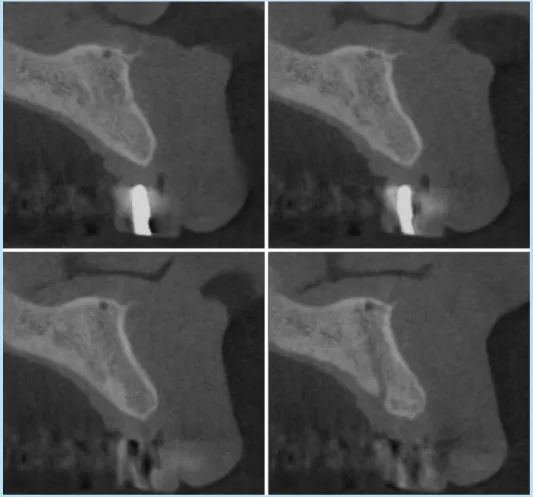
Fig. 4.
Cone-beam computed tomography, cross-sectional view at the implant placement site (#21, maxilla left central incisor).Kang-Hee Lee et al. : The Use of Computer Guided
Surgical Stent in Dental Implant of Maxilla Central
Incisor. Implantology 2016
Case Report
형성을 유도하였다. 치간유두의 재형성을 유도하기 위해 서 치조골의 높이와 치은의 두께를 고려해 임시 치관의 인접면 접촉점을 치조골 5 mm 상방에 형성하였다4,5. 1개 월 간격으로 순측 치은변연과 치간 유두의 높이와 형태 를 확인하고 레진 임시 치관을 계속해서 수정하여서 심 미적인 치은 형태가 얻어지도록 노력하였다(Fig. 8).
2차 수술 4개월차에 잘 유도된 치은형태에 따라 맞춤 지대주(custom abutment)와 심미보철물(porcelain fused zirconia crown)을 제작하여 장착하였다(Fig. 9).
2014년 6월 3일에 환자가 치아와 치은의 심미, 기능에 대해 만족하였으나 치은 착색에 대해 개선을 요구하여
Fig. 5.
Implant placement planning was done using various images, In2Guide implant planning progam (CyberMed, Seoul, Korea). 3D skull, cross-sectional view, horizontal view, etc., with consideration of width and depth of the alveolar bone, length of abutment, a relationship with lower teeth and gingival thickness.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant of Maxilla Central Incisor. Implantology 2016
Fig. 6.
A computer guided surgical stent made of acryl using three-dimensional print.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant
of Maxilla Central Incisor. Implantology 2016
Fig. 9.
After gingival molding, gingival impression taking and Installation of the custom abutment and porcelain fused zirconia crown was done. The black triangle was successfully filled, and symmetrical marginal gingiva was achieved. At the upper attached gingiva, stains due to smoking and postoperative scar can be observed.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant
Fig. 7.
Cone-beam computed tomography, cross-sectional view of implanted right maxilla central incisor using surgical guide stent. Within narrow alveolar ridge, placement of implant was seen without any invasion of adjacent structure. Bone graft was done at the buccal site, to compensate narrow alveolar ridge.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant of Maxilla Central Incisor. Implantology 2016
Fig. 8.
Clinical photo with installation of abutment and resin temporary crown after second surgery. There is a black triangle due to recession of an incisive papilla, and irregular and thin marginal gingiva can be observed.Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant
of Maxilla Central Incisor. Implantology 2016
Case Report
반흔조직 제거와 치은 미백을 위한 2차 치은성형수술을 한 차례 시행하였다. 치은성형수술 1주일 후 반흔과 착색 이 현저히 감소되었으며 후에도 계속해서 유지되고 있다 (Fig. 10).
III
총괄 및 고찰상악중절치의 상실은 환자에게 심미적, 기능적 장애를 발생시킬 뿐 아니라 그로 인해 심미적 장애가 동반될 수 도 있다. 임플란트 치료는 상실된 치아를 대체하는 아주 좋은 치료이지만 식립체가 일단 식립되고 나면 제거나 교체가 어렵다는 단점이 있다. 전치부 치료에서 부적절 한 위치에 식립된 임플란트 식립체는 비심미적인 치관과 치은을 만들기 때문에 환자의 만족도와 치료의 완성도를 떨어뜨린다. 또 전치 유도에 적합하지 못한 기울어진 치 축이나 교합 형태는 교합력을 적절히 분산하지 못하기
때문에 기능적인 문제 외에도 스크류의 풀림, 치관의 반 복적인 파절, 임플란트 찢김과 같은 불량한 결과를 초래 하기도 한다. 또한 지나치게 깊게 식립된 식립체는 깊은 치주낭을 형성하여 임플란트 주위염을 지속적으로 유발 하기도 하고, 반대로 낮게 식립된 식립체는 식립체나 지 대주의 노출, 검게 음영이 드리운 치은과 같은 심각한 심 미적 문제를 일으키기도 한다. 따라서 전치부 임플란트 치료 시에는 인접 치아와의 간격, 협설측 잔존골의 두께 뿐 아니라, 식립 각도, 식립 깊이, 대합치과의 교합 양상, 주변 치아들과 교합의 조화 등 모든 요소를 고려하여 식 립되어야 할 것이다3-5.
하지만 술자가 수술 중에 이런 모든 것을 살피며 식립 한다는 것은 현실적으로 어려움이 있어 전치부 수술을 위해서는 식립체의 위치를 유도해 줄 수 있는 surgical stent가 필수다. 기존 방식의 스텐트는 인접치와의 간격 이나 이상적인 보철의 위치를 알려줄 수는 있지만, 치조 골의 협설 폭경과 높이에 대한 고려가 없기 때문에 수술 중 수정이 불가피 했다. 삼차원의 CBCT data를 이용하는 computer guided surgical stent system은 치조골의 분석 이 가능할 뿐 아니라, 수술 계획 컴퓨터 프로그램상에서 가상의 보철도 제작해 볼 수 있기 때문에 임플란트 치료 에 필요한 모든 면을 다각도로 분석하여 정밀한 치료 계 획을 세울 수 있게 해준다. Computer guided surgical stent를 사용하면 수술 중 수정이 거의 필요 없고 따라서 미리 제작해 놓은 지대주와 임시 치관을 식립 후 바로 연 결하여 전치부의 심미, 기능을 회복하여 줄 수도 있다.
또 flapless로 수술을 할 수도 있고, 수술 시간을 줄여 술 중 감염 가능성과 출혈, 통증, 술 후 부종을 줄여준다6.
이전 연구들에 따르면 computer guided surgical stent 를 이용해 수술하면 0.5~1.5 mm의 수평적 평균 오차를 보인다7,8. 이러한 오차는 최종 보철의 사전 제작은 불가 능한 수치이지만, 레진으로 된 임시 치관을 사전 제작해
Fig. 10.
One month check-up after gingival plasticsurgery and bleaching. The pinkish-red and smooth attached gingiva can be seen, and proper preservation of interproximal papillae and marginal gingiva was observed.
Kang-Hee Lee et al. : The Use of Computer Guided Surgical Stent in Dental Implant
of Maxilla Central Incisor. Implantology 2016
놓고 식립 당일에 임시 치관의 내면을 소량 삭제하거나 재이장하여 장착하는 방식으로 충분히 조정이 가능한 정 도의 수치다.
Computer guided surgical stent를 이용한 수술에서는 스텐트와 치아의 적합성이 떨어지면 유격이 생겨 수술 중 장치가 움직일 수 있다. 또 스텐트에 있는 metal sleeve와 drill 사이의 유격에 의해서도 수평적 오차나 식 립 각도 오차가 생기기도 한다. 기술이 개선되어 감에 따 라 수술의 오차도 줄어들어가는 추세이지만, stent의 정 확도 외에도 술자에 의한 오차라는 변수가 있기 때문에 정확한 수술을 위해서는 술자의 숙련도 역시 중요하다.
최근에는 다양한 computer guided surgical stent system 이 있기 때문에 술자에게 맞는 시스템을 선택하는 것 역 시 중요하다.
본 케이스에서는 computer guided surgical stent를 이 용해 임플란트 식립체를 이상적인 수평, 수직적 위치에 자리하고 치조골 이식을 통해 치조골 형태를 개선하였으 며, 임시 치관을 4개월간 유지하며 심미적인 치은의 외 연과 치간 유두 형성을 유도하였다. 이러한 넓은 면적의 수술은 반흔조직, 치은 착색을 형성하는 경우가 있기 때 문에 반흔조직 제거, 치은변연 성형, 치은 미백 치료를 통해 전치부 치료의 완성도를 보다 높일 수 있었다.
IV
결 론교정을 통하여 중절치가 위치할 간격을 확보한 뒤 발치 시기를 조정하여 치조골 이식을 동반한 식립이 이루어졌 고 computer guided surgical stent를 사용하여 이상적인 임플란트의 위치를 얻을 수 있었다. 이상적인 임플란트 의 위치 덕분에 심미적이고 기능적인 보철 치료가 가능
하였고, 추후 주기적인 검사에서 골소실이나 보철물 손 상 없이 전치부가 잘 유지되는 것을 관찰하였다.
완성도 있는 전치부 치료를 위해서는 수술 전 정확한 진단과 계획이 필요하고, 계획한 대로 식립하는 것이 중 요하다. Computer guided surgical stent는 이것을 가능 하게 해주는 유용한 수술 보조 장치다.
References