114
Case Report
ISSN 2465-8243(Print) / ISSN: 2465-8510(Online) https://doi.org/10.14777/uti.2016.11.3.114 Urogenit Tract Infect 2016;11(3):114-117
http://crossmark.crossref.org/dialog/?doi=10.14777/uti.2016.11.3.114&domain=pdf&date_stamp=2016-12-25
Successful Treatment of Seminal Vesicle Abscess with Rectal Fistula after Rectal Decompression: Report of a New Case
Jae-Wook Chung, Yun-Sok Ha, Jun Nyung Lee, Hyun Tae Kim, Eun Sang Yoo Department of Urology, Kyungpook National University School of Medicine, Daegu, Korea
Seminal vesicle abscess is a rare urologic disease. Herein, we report our experience of the first case of a 41-year-old male patient with neurogenic bladder who underwent successful treatment of seminal vesicle abscess with rectal fistula after rectal decompression. Only a simple insertion of the rectal tube with intravenous antibiotics was able to remove the seminal vesicle abscess with rectal fistula without any percutaneous, transvesical, or transurethral drainage of the abscess. Rectal decompression should be considered in advance as a treatment of seminal vesicle abscess with rectal fistula before performing any invasive abscess drainage or fistulectomy.
Keywords: Abscess; Decompression; Fistula; Rectum; Seminal vesicles
Copyright 2016, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 4 August, 2016 Revised: 18 August, 2016 Accepted: 26 August, 2016
Correspondence to: Eun Sang Yoo http://orcid.org/0000-0002-7442-6886 Department of Urology, Kyungpook National University School of Medicine, 680 Gukchaebosang-ro, Jung-gu, Daegu 41944, Korea
Tel: +82-53-420-5841, Fax: +82-53-421-9618 E-mail: [email protected]
Seminal vesicle abscess (SVA) is a rare disease entity.
Due to its non-specific clinical symptoms, SVA is difficult to be suspected. Moreover, to date, the clinical presentation and treatment of SVA with rectal fistula have not been well established. Therefore, we introduce the first case of successful treatment of SVA with rectal fistula after rectal decompression. This study was approved by the institutional review boards of Kyungpook National University Hospital (IRB no. 2016-05-019).
CASE REPORT
A 41-year-old man was admitted to the department of urology through the emergency center. He had a neurogenic bladder due to thoracic-spine injury after a traffic accident 20 years ago. He presented myalgia and chills with low abdominal pain and lower urinary tract symptoms (LUTS), which gradually developed since 1 month prior to being admitted. The patient was febrile (>39.1oC), with otherwise
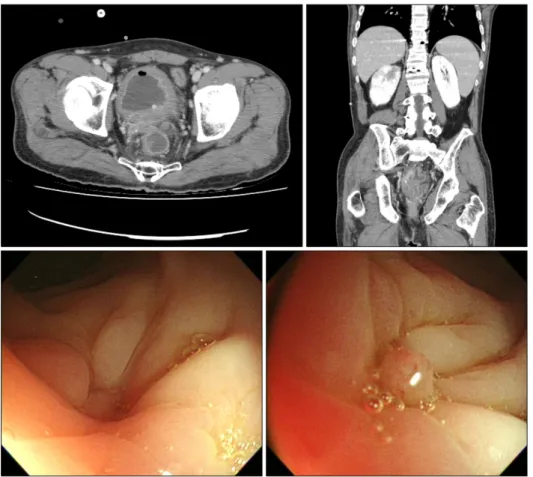
normal vital signs. The initial blood work showed a white blood cell count of 18,700/l. Computed tomography (CT) revealed 8 cm sized thick-walled pelvic abscess and right hydronephrouretersosis due to pelvic abscess (Fig. 1).
Immediate consultation with the department of internal medicine was done, and empirical intravenous (IV) ceftriaxone and aztreonam were injected, and in addition, urethral catheter was inserted. On the following day, percutaneous nephrostomy (PCN) was performed, but high fever still existed. For further imaging workup, on the third day, magnetic resonance imaging (MRI) was performed, and MRI showed 7.7 cm thick-walled abscess in the posterior aspect of the urinary bladder, which was initially thought to be originated from the seminal vesicle and formed the rectal fistula (Fig. 2). Immediately after, sigmoidoscopy was performed, and rectal ulcer with fistula formation was discovered, in which chronic inflammation was confirmed by a biopsy (Fig. 3). However during sigmoidoscopy, transrectal drainage of SVA failed because definite fistula
Jae-Wook Chung, et al. SVA with Rectal Fistula 115
Urogenit Tract Infect Vol. 11, No. 3, December 2016 Fig. 1. Computed tomography revealed 8 cm sized thick-walled pelvic abscess and right hydronephrouretersosis due to pelvic abscess.
Fig. 2. Magnetic resonance imaging showed 7.7 cm thick-walled abscess in the posterior aspect of the urinary bladder, initially thought to be originated from the seminal vesicle and rectal fistula.
Fig. 3. Sigmoidoscopy showed rectal ulcer with fistula formation.
opening was not detected. Conservative treatment went on and follow-up CT on the 10th day showed a decreased size of the abscess cavity and slightly improved right hydronephroureterosis. The department of general surgery was consulted, and nothing per os (NPO) with total parenteral nutrition (TPN) was started. Rectal decompression through the rectal tube insertion was
performed. Blood and urine cultures showed no bacterial growth after 5 days. Rectal decompression through the rectal tube insertion maintained only for 5 days. Follow-up CT and sigmoidoscopy on the 20th day showed an improved state of abscess cavity and rectal fistula (Fig. 4). PCN was removed and the water intake was permitted. Patient defecated well after a soft diet, and on the 30th day he
116 Jae-Wook Chung, et al. SVA with Rectal Fistula
Urogenit Tract Infect Vol. 11, No. 3, December 2016
Fig. 4. Follow-up computed tomography and sigmoidoscopy on the 20th day showed an improved state of abscess cavity and rectal fistula.
was discharged with urethral catheter inserted. Two weeks after discharge, he visited the outpatient department of our urologic center and had the urethral catheter removed.
Urodynamic study showed low Pdet compliance (15.2 ml/cmH2O) and low detrusor pressure at maximal peak flow (PdetQmax 13 cmH2O). The alpha blocker with anticholinergic was prescribed without clean intermittent catheterization. Now, he is free from symptoms related to SVA with rectal fistula and showed a clear urinalysis.
DISCUSSION
SVA is a rare urologic disease [1,2]. A case of SVA was first reported in 1978 by Rajfer et al. [3]. To the best of our knowledge, only less than 30 cases of SVA have ever been reported in the literature [4-6].
The exact etiology of SVA is unclear but predisposing factors include diabetes mellitus, human immunodeficiency virus infection, urinary tract infection, indwelling urethral catheter or urologic instrumentations, intraabdominal carcinoma, and anatomical abnormalities [7,8]. In this case, neurogenic bladder and history of previous clean intermittent
catheterization are thought to be the cause of SVA.
SVA is difficult to diagnose because its bizarre clinical symptoms are non-specific. The symptoms of SVA can be fever, LUTS, urinary retention, hematospermia, rectal discomfort, and perineal, abdominal or inguinal pain. In this case, our patient presented with high fever, LUTS, and low abdominal pain.
The diagnostic imaging modalities of SVA include transrectal ultrasound (TRUS), CT or MRI. Although CTs are most frequently used as the chosen diagnostic method, the most recent study showed that TRUS may be the most cost-effective diagnostic tool [5]. At our center, CT was performed firstly, and MRI was also used secondly because the origin of the pelvic abscess was unclear—could either be from the prostate or the seminal vesicle.
Furthermore, rectal fistula formation with SVA abscess is extremely rare, and only a few cases were reported in the English literature. To the best of our knowledge, this is the first reported case of a successful treated SVA abscess with rectal fistula without any invasive abscess drainage or fistulectomy. Usually, it is thought that SVA treatment, such as tranvesical, transperineal, transgluteal or transure-
Jae-Wook Chung, et al. SVA with Rectal Fistula 117
Urogenit Tract Infect Vol. 11, No. 3, December 2016
thral abscess drainage, is needed. However, in this case, the fistula opening was not detected during a sigmoido- scopy, and according to the consultation from department of internal medicine and general surgery, the conservative treatment was chosen instead of the invasive procedure.
Although the periods of NPO with TPN was long, the patient was well tolerated and he was able to overcome SVA only with the conservative treatment, such as IV antibiotics and rectal decompression through rectal tube insertion.
Therefore, rectal decompression should be considered as the treatment of SVA with rectal fistula before performing invasive abscess drainage or fistulectomy.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Eastham JA, Spires KS, Abreo F, Johnson JB, Venable DD.
Seminal vesicle abscess due to tuberculosis: role of tissue culture in making the diagnosis. South Med J 1999;92:328-9.
2. Frye K, Loughlin K. Successful transurethral drainage of bilateral seminal vesicle abscesses. J Urol 1988;139:1323-4.
3. Rajfer J, Eggleston JC, Sanders RC, Walsh PC. Fever and prostatic mass in a young man. J Urol 1978;119:555-8.
4. Pandey P, Peters J, Shingleton WB. Seminal vesicle abscess: a case report and review of literature. Scand J Urol Nephrol 1995;29:521-4.
5. Sağlam M, Uğurel S, Kilciler M, Taşar M, Somuncu I, Uçöz T.
Transrectal ultrasound-guided transperineal and transrectal management of seminal vesicle abscesses. Eur J Radiol 2004;52:329-34.
6. Dewani CP, Dewani N, Bhatia D. Case report: tubercular cold abscess of seminal vesicle: minimally invasive endoscopic management. J Endourol 2006;20:436-42.
7. Zagoria RJ, Papanicolaou N, Pfister RC, Stafford SA, Young HH 2nd. Seminal vesicle abscess after vasectomy: evaluation by transrectal sonography and CT. AJR Am J Roentgenol 1987;149:137-8.
8. Gulanikar A, Clark J, Feliz T. Prostatic abscess: an unusual presentation of metastatic prostate cancer. Br J Urol 1998;82:309-10.