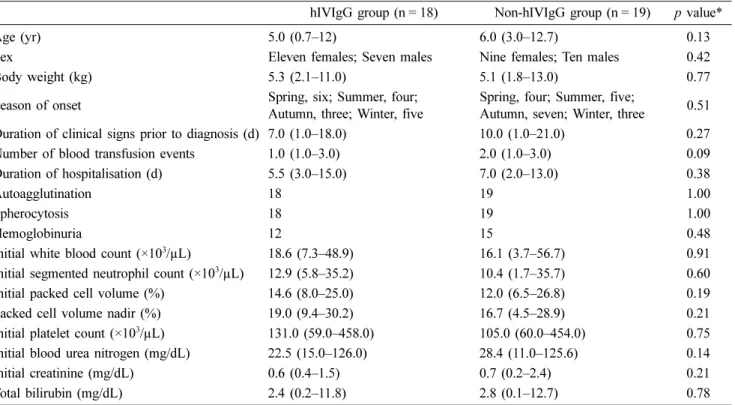
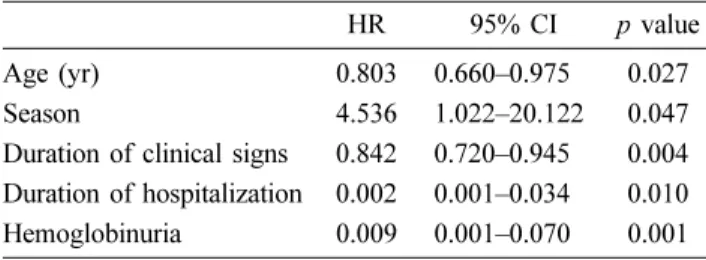
Prognostic factors and efficacy of human intravenous immunoglobulin G in dogs with idiopathic immune-mediated hemolytic anemia: a retrospective study
7
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
수치
관련 문서
The aim of this study was not only to compare the differences of ego-resilience between students with high experience and students with low experience in
In this study, 12 weeks of aerobic exercise was conducted in middle-aged women aged 45 to 55 years with a body fat rate of 30% or more to determine the effects of blood
In the present study we investigated the proliferation effect of human oral cancer KB cell treated with pulsatilla koreana extract.. We analyzed the effects of this
This study was conducted to analyze the effects of obesity on the core stability and metabolic syndrome risk factors of middle - aged women.. The effect
Although van der Waals equation is still less accurate at high
A subsidiary body for implementation shall report regularly to the Conference of the Parties on all outcome, which will be carried out in accordance with Article 7, paragraph 2,
Accordingly, this study aims to verify the effect of human brand attributes, which have the role of brands, on human brand authenticity, human brand attachment, and
The purpose of this study is to identify the leading factors affecting the human error using actor analysis on masters and officers’ responses in the ship navigation field.
