KISEP Clinical Research J Korean Neurosurg Soc 29: : : :249-254, 2000
외상성 뇌실질내 혈종에 대한 상측방 키홀을 통한 내시경적 혈종 제거 *
을지의과대학 신경외과학교실
박성진·하호균·정 호·이상걸·박문선
= Abstract =
Endoscopic Removal of Traumatic Intracerebral Hematoma via Superolateral Keyhole
Sung-Jin Park, M.D., Ho-Gyun Ha, M.D., Ph.D., Ho Jung, M.D., Sang-Keol Lee, M.D., Moon-Sun Park, M.D., Ph.D.
Department of Neurosurgery, Eul-Ji University, School of Medicine, Taejon, Korea
bjective:As a minimally invasive strategy, endoscopic technique was introduced for removal of the traumatic intracerebral hematoma.
Material and Method:A 54-year-old man with three-day history of seizure and progressive mental deterio- ration after traffic accident was presented. Computerized Tomography(CT) of the brain showed a huge intracerebral hematoma on the right frontal lobe and ventricle. The operation was performed via right frontal superolateral keyhole with 2cm eyebrow skin incision. Using 0-degree and 30-degree angled lens 4mm rigid endoscopes, nearly all of the hematoma was evacuated under the direct endoscopic visualization and a ventricular catheter was exactly placed into the frontal horn of the right lateral ventricle at the end of procedure.
Results:The seizure was discontinued and neurological status had been improved during postoperative periods.
Postoperative CT demonstrated that most of the hematoma was removed and the ventricular drainge tube was exactly placed in the right foramen of Monro.
Conclusion:With endoscopic technique, the authors successfully evacuated traumatic intracerebral hematoma and exactly placed the ventricular drainage catheter under direct visualization.
This technique may be considered as an another option for removal of traumatic intracerebral hematoma.
KEY WORDS:Traumatic intracerebral hematoma・Endoscope・Superolateral approach・Keyhole surgery.
서 론
외상성 뇌실질내 혈종의 수술적응증은 정확히 정립되어 있지는 않으나 McLaurin 등
22)은 의식수준이 떨어지거나 국소 신경학적 결손이 진행될때 수술의 적응이 된다고 하였 으며, 여기에 혈종의 양, 환자의 전신상태 및 보호자와의 협 의 등이 추가로 고려되어야 한다. 외상성 뇌실질내 혈종의 수술방법으로서는 일반적으로 1) 개두술에 의한 혈종 제거
술과 2) 두개천공후 배액하는 방법 및 3) 뇌정위적 흡인술 에 의한 혈종제거술이 있고, 근자에는 위 2), 3)의 방법에 urokinase을 이용한 도관배액술
7)10)14)18)32)을 시행하는 경 우가 보고되고 있다. 개두술에 의한 혈종 제거술은 지혈이 용이하며 혈종을 완전 제거하여 충분한 감압을 이룰 수 있 고, 필요한 경우 두개골 절제술에 의한 뇌압조절이 용이하 다는 장점
5)21)이 있으나, 광범위한 수술부위로 인해 불필요 한 부위의 노출과 정상 뇌조직의 손상 및 장시간의 마취와 수술에 따르는 단점이 있다
4)20)21)28)30)31). 반면에 두개천공 후 배액술이나 뇌정위적 혈종 제거술은 국소마취하에서 시 행할 수 있어 전신 상태가 불량한 고령의 환자에서 유리하
OOOO
*본 논문의 요지는 1999년 5월 8일 대한 신경손상학 연구회 제6차 정 기학술대회에서 발표되었음.
고, 뇌조직 손상을 최소한으로 줄일 수 있는 장점
7)10)18)이 있으나, 많은 양의 혈종을 빠른 시간내에 제거하지 못함으 로써 즉각적인 감압을 이루지 못하고 수술중 출혈시 지혈이 용이하지 못하다는 단점
19)이 있다. 위와 같은 이유로 본 원 에서는 전신상태가 불량하며 반복되는 전신경련과 지속적인 의식저하를 보인 환자에게 최소침습적 방법의 일환으로 키 홀(keyhole)을 통한 내시경적 혈종 제거술을 시행하고 좋 은 결과를 얻었기에 문헌고찰과 함께 보고하고자 한다.
증 례
병력 및 이학적 신경학적 검사:3일전 발생한 교통사고 로 타병원에 입원해 있던 54세 남자 환자로 반복되는 전신 경련과 지속적인 의식저하를 주소로 본 원에 전원 되었으며, 내원시 의식은 혼미상태로 글라스고우 혼수계수 7(GCS:
E1V2M4)이었다. 우측 동공의 크기는 5mm, 좌측은 3mm 로 동공부동증(anisocoria)이 있었고, 우측 동공은 대광반 사가 소실되어 있었다. 환자는 알콜성 간염을 앓고 있었으 며 내원시 흡인성 폐렴과 약에 의한 독성 간염이 병발해 있 는 상태였다.
방사선학적 검사:내원당시 검사한 뇌전산화 단층촬영에 서 우측 전두엽에 약 40ml정도되는 혈종이 있었으며, 우측 측뇌실의 전각부에 뇌실내 혈종이 같이 있었다. 뇌부종이나
혈종에 의한 종괴효과는 심하지 않았었다. 혈종이 가장 크며 뇌의 표면에 닿아있는 부위는 상안와연에서 상방으로 2cm, 중심선에서 측방으로 4cm 떨어진 곳이었으며, 이 곳에서 Monro공(foramen of Monro)으로 그은 혈종의 장축은 중 심선에서 약 40도 정도 우측으로 회전되어 있었다(Fig. 1).
수술방법:전신마취하에 앙와위를 취한 후 우측 상안와연 에서 상방으로 2cm, 중심선에서 측방으로 4cm 떨어진 곳 에 천공 부위를 정하고 두부를 좌측으로 40도 회전시켜 천 공부위에서 수직으로 뇌실질내로 진입시 우측 측내실의 전 각에 도달할 수 있도록 하였다(Fig. 2). 약 2cm정도 피부절 개하고 견인기로 고정한 후 두개골 천공하여 경막 절개 후 피질부의 혈종을 제거하였다. 피질내에 어느정도 공간이 형 성되자 직경 1cm 크기의 플라스틱 통을 천공부에 넣어 통 로를 확보 하였다. 직경 4mm 0도 경성 내시경을 플라스틱 통로를 통해 진입시키면서 혈종 제거를 시작하였다. 혈종 제거 는 주로 흡입기(suction catheter)를 통해 이루어졌으며 혈종 이 너무 큰 경우에는 양극전기소작기(bipolar coagulator)로 잘게 부순 후 흡입제거 하였다. 출혈은 양극전기소작기와 Surgicel
®로 충분히 지혈되었으며 뇌실질에 붙어있는 혈종 의 가장자리는 가급적 제거하지 않았다. 이어서 직경 4mm 30도 경성 내시경을 이용하여 혈종의 주변부를 제거하였으 며 생리식염수로 자주 세척하여 출혈여부 확인 및 열에의한 손상을 줄이려 노력했다. 만족할만큼 혈종을 제거한 후 다
Fig. 1. Preoperative computerized tomography of the brain showing a huge intracerebral hematoma on the right frontal lobe and a intraventricular hematoma in the frontal horn of right lateral ventricle. There are no significant brain swelling, edema, or mass effect.
Fi 2 S h ti d i f d i i l t j t Th h d t t d t t l t l id b t 40 d
A A A
A B B B B
박성진 · 하호균 · 정 호 · 이상걸 · 박문선
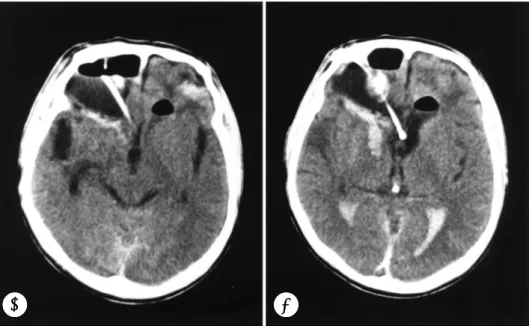
시 0도 경성 내시경을 뇌의 심부로 진입시키면서 혈종을 제 거하자 우측 측뇌실의 전각이 열리면서 뇌척수액이 새나오 기 시작했다. 뇌실내 혈종을 흡입기로 제거(Fig. 3)한 후 내 시경을 전각안으로 진입시키고 직접보면서 뇌실외배액관을 Monro공에 집어 넣었다. 생리식염수로 세척하고 출혈없음 을 확인한 후 천공부위에 Gelfoam
®을 얇게 덮고 그 위에 천공시 모아 두었던 뼈가루를 두껍게 깐 후 다시 얇은 Gel- foam
®을 얹었다. 근육과 피하층을 봉합하고 피부는 6-0 흡수성 봉합사로 연속봉합하여 흉터가 최소한으로 남게하였 다. 수술시간은 피부절개에서부터 피부봉합까지 약 1시간정 도 소요되었다.
수술 후 상태 및 추적검사:수술 후 환자는 더 이상 경련 을 일으키지 않았으며 의식의 호전을 보였다. 수술 후 제1 일에 우측동공의 대광반사가 비록 느리기는 하였으나 반응 을 보이기 시작했고, 글라스고우 혼수계수 9(GCS:E3V TM5)로 호전 되었다. 수술 후 제2일에 즉각적인 대광반사 가 이루어졌고, 검사자의 명령에 따르게(obey command) 되어 글라스고우 혼수계수 11(GCS:E4V
TM6)까지 호전 되었다. 수술 후 제3일에 추적검사한 뇌전산화 단층촬영에 서 대부분의 혈종이 제거 되었으며, 뇌실외배액관이 정확히 Monro공에 들어가 있음을 볼 수 있었다(Fig. 4).
고 찰
1910년 L’Espinasse
9)가 뇌수종을 치료하기 위해 방광 경(cystoscope)을 이용하여 측뇌실의 맥락총 응고를 시도 한 이래 내시경을 이용한 신경외과 수술은 꾸준히 발전해오 고 있으며, 최근 최소 침습적 수술방법과 잘 부합되어 장비 의 발전과 그 영역이 급격히 넓어지고 있다.
1922년 Dandy
8)는 경성 뇌실경(ventriculoscope)을 이 용하여 맥락총 응고를 시도하였고, 1923년 Mixter
23)는 수 도관 폐쇄에 의한 뇌수종 환자에게 내시경적 제3뇌실 누공 술을 시도하여 최초로 성공하였다. 그 후, 1936년과 1938 년에 Stern
29)과 Pool
24-26)은 척수경(spinoscope)을 이용 하여 척수강내 병소를 검경하였다. 계속하여 내시경 기술은 발달되어 1973년 Fukushima
11)는 유연한 ventriculofib-
Fig. 2. Schematic drawing of endoscopic surgical trajectory.
The head was rotated to contralateral side about 40 degrees and the superolateral keyhole was placed at 2cm above the right supraorbital ridge and 4cm off the midline. With introduction of the endoscope ver- tically passing through the hematoma cavity from this keyhole, the frontal horn was accessible according to the planned trajectory.
Fig. 3. Intraoperative endoscopic view showing aspiration of intraventricular hematoma using a suction tube(arrow in upper) and the inner surface of the frontal horn of the right lateral ventricle after removal of clots(arrow head in lower).
i 4 i i d h b i d 3
B
B
B
B
A A A
A
erscope을 이용하여 두개강내 조직생검 및 수술을 시행하 여 이전까지 주로 뇌수종 치료에 사용되었던 내시경의 영역 을 넓혔고, Apuzzo 등
1)은 side-viewing telescope을 이용 하여 뇌하수체 종양을 접형동을 통한 수술로 제거하였을 뿐 만 아니라 측두하 접근법을 통한 뇌저동맥 말단의 동맥류를 수술하고 원위부 클립(clip)을 확인하였으며, 또한 요추간판 제거술시 추간판의 잔존량을 직접 눈으로 확인할 수 있었다.
1980년대에는 광학기술의 발전과 기구의 소형화와 유연성 증가 등의 내시경의 기술적 발전이 크게 이루어져
2)3)27)이전 보다 안전하게 수술을 할 수 있게되었고, 최근에는 3차원 영상을 얻을 수 있는 내시경이 연구되고 있다. 현재 내시경 적 제3뇌실 누공술은 많이 보편화 되었으며, 뇌전산화 단층 촬영술의 발달로 1980년에는 뇌정위적 수술에 Jacques
13)가 종양경(tumor scope)을 이용하여 뇌종양, 뇌실질내혈종, 뇌 동정맥 기형을 치료하였으며, Heilbrun
12)도 뇌정위적 혈 종 제거술에 내시경을 이용하였다. 우리나라에서도 점차 그 이용이 증가되어 뇌정위적 내시경술은 1990년에 김성호 등
17)이 보고한 바 있고, 1995년에 최중언
6)은 내시경적 제3뇌실 누공술에 대해 발표한바 있다. 1997년에는 김인영 등
15)은 외상성 시신경 손상 환자에게 내시경적 시신경 감압술을 성 공리에 시행하였고, 1998년에는 김명현 등
16)은 3년동안 시 행한 69예의 내시경적 수술에 대해 발표했으며, 뇌수종, 피 각부출혈, 지주막낭종, 낭미충증, 뇌실내종양, 분엽화된 만 성 경막하혈종, 낭성 두개인두종, 뇌실질내종양, 외부물질제 거 등의 다양한 임상예를 발표한 바 있다.
이처럼 내시경의 신경외과 영역에서의 응용은 최근 급격 히 증가되고 있는 추세이나 아직 외상성 뇌실질내 혈종에 대해서는 그 이용이 극히 미약한 편이다. 외상성 뇌실질내 혈종의 경우 일반적으로 개두술에 의한 혈종제거술이 가장 많이 이용되고 있으며 그 외 천공술이나 뇌정위적 혈종 제 거술 후 urokinase을 이용한 배액술이 있으며, 이들의 장・
단점에 대해서는 이미 서론에서 기술한 바 있다. 최소 침습 적인 방법으로서의 외상성 뇌실질내 혈종에 대한 키홀 (keyhole)을 통한 내시경적 혈종 제거술은, 비록 뇌부종이 심한 경우에는 시행할 수 없으나, 짧은 수술시간으로 전신 상태가 좋지 않아 장시간의 마취가 곤란한 환자에게 도움이 될 수 있으며, 수술에 불필요한 정상 뇌조직을 최대한 보존 할 수 있어 개두술에 의한 혈종 제거술의 단점을 보완할 수 있다. 또한 직접 혈종부위를 보면서 지혈과 혈종 제거가 가 능하여 천두술과 뇌정위적 혈종 제거술의 단점도 보완할 수 있다. 본 예의 경우에서도 환자는 반복적인 전신경련과 지 속적인 의식 저하 때문에 최대한 많은 양의 혈종을 빠른 시 간내에 제거할 필요가 있다고 판단 되었으나, 환자의 폐렴 및 독성 간염은 장시간의 마취에 의해 더욱 더 악화될 가능 성이 있었고, 천공술이나 뇌정위적 혈종 제거술은 충분한 양의 혈종을 빠른 시간 내에 다 제거할 수 없다는 판단하에 내시경적 혈종 제거술을 시행하게 되었다. 이처럼 부종이 심하지 않은 뇌실질내 혈종 환자에게서, 짧은 시간에 대량 의 혈종 제거가 필요한 경우에는, 내시경적 혈종 제거술이 매우 효과적이며 간단한 방법이라고 생각된다.
Fig. 4. Postoperative computerized tomography obtained 3 days after operation revealing that most of the hematoma was removed and the ventricular drainge tube was exactly placed in the right foramen of Monro.
A A
A A B B B B
박성진 · 하호균 · 정 호 · 이상걸 · 박문선
결 론
내시경을 이용한 최소 침습적 방법으로 내시경하에서 혈 종부위를 보면서 외상성 뇌실질내 혈종을 제거하였으며, 뇌 실외 배액관을 정확히 위치하고 좋은 결과를 얻었기에 문헌 고찰과 함께 보고하는 바이며, 추후 더 많은 경험과 장비의 개발이 필요하다고 생각한다.
•
논문접수일:1999년 8월 25일•
심사완료일:1999년 10월 25일•
책임저자:하 호 균301-070 대전광역시 중구 목동 24-14번지 을지의과대학 신경외과학교실
전화:042) 259-1269, 1277, 전송:042) 256-3461 E-mail:[email protected]
References
1) Apuzzo MLJ, Heifetz MD, Weiss MH, et al:Neurosurgical
endoscopy using the side-viewing telescope. J Neurosurg 46
:398-400, 1977
2) Auer LM, Deinsberger W, Niederkorn K, et al:Endoscopic
surgery versus medical treatment for spontaneous intracere- bral hematoma
:A randomized study. J Neurosurg 70
:530- 535, 1989
3) Auer LM, Holzer P, Ascher PW, et al:Endoscopic neuro-
surgery. Acta Neuchir 90
:1-14, 1988
4) Baek SC, Choi BY, Kim OL, et al:The clinical study of
stereotaxic aspiration in spontaneous intraparenchymal hema- toma. J Kor Neurosurg Soc 16
:695-708, 1987
5) Cho TG, Nam DH, Cho BM, et al:Stereotactic evacuation of
spontaneous intracerebral hemorrhage. J Kor Neurosurg Soc 28
:237-245, 1999
6) Choi JU:Endoscopic third ventriculostomy. J Kor Neurosurg
Soc 24
:1226-1234, 1995
7) Choo WH, Cho JH, Whang BW, et al:Stereotactic evacu-
ation and urokinase irrigation in the management of sponta- neous intracerebral hemorrhage. J Kor Neurosurg Soc 24
:248-251, 1995
8) Dandy WE:Cerebral ventriculoscopy. Bull Johns Hopkins
Hosp 33
:189, 1922
9) Davis L:Neurological surgery. Philadelphia. Lea and Febi-
ger, 1936, pp405
10) Eun JP, Jung N, Shin MS:Stereotactic surgical management
of traumatic intracerebral hematoma. J Kor Neurosurg Soc 24
:1024-1029, 1995
11) Fukushima T:Endoscopy of Meckel’s cave, cisterna magna
and cerebello-pontine angle. J Neurosurg 48
:302-306, 1978
12) Heilbrun MP:Computed tomographic stereotaxy. Clin Neu-rosurg 31
:564-581, 1984
13) Jacques S, Shelden CH, McCann GD, et al:Computerized
three-dimensional stereotaxic removal of small central nervous system in patients. J Neurosurg 53
:816-820, 1980
14) Jo HR, Rho DS, Lee CR, et al:The use of urokinase in tr-
aumatic intracerebral hematoma treatment. J Kor Neurosurg Soc 18
:723-732, 1989
15) Kim IY, Kim JH, Lee JK, et al:Endoscopic optic nerve de-
compression in traumatic optic neuropathy. J Kor Neurosurg Soc 26
:874-878, 1997
16) Kim MH, Song JH, Park HK, et al:3 year experience of
neuroendoscopic procedures-69 cases. J Kor Neurosurg Soc 27 Supplement, 1998, pp331
17) Kim SH, Doh ES, Ko SK, et al:The role of stereotactic
endoscopy in ventricular and juxtaventricular lesions. J Kor Neurosurg Soc 19
:1361-1368, 1990
18) Kwon Y, Kim CJ, Rim SC, et al:Comparative clinical
analysis of stereotaxic surgery vs conservative treatment for spontaneous intracerebral hematoma. J Kor Neurosurg Soc 19
:995-1000, 1990
19) Lee JC, Min BK, Park K, et al:The clinical analysis of stere-
otactic aspiration of spontaneous intracerebral Hemorrhage.
J Kor Neurosurg Soc 26
:347-353, 1997
20) Luessenhop AJ, Shelvlin WA, Ferrero AA, et al:Surgical
management of primary intracerebral hematoma. J Neurosurg 27
:419-427, 1967
21) McKissock W, Richardson A, Taylor J:Primary intracere-
bral hemorrhage
:A controlled trial of surgical and conser- vative treatment in 180 unsellected cases. Lancet 2
:221-226, 1966
22) Mclaurin R, Mcbribe BH:Traumatic intracerebral hema-
toma. -Review of 16 surgically treated cases-. Ann Surg 143
:294-305, 1956
23) Mixter WJ:Ventriculoscopy and puncture of the floor of the
third ventrcle. Boston Med Surg J 188
:277-278, 1923
24) Pool JL:Direct visualization of dorsal nerve roots of thecauda equina by means of a myeloscope. Arch Neurol Psychiat 59
:1308-1312, 1938
25) Pool JL:Myeloscopy:
Diagnostic inspection of the cauda equina by means of endoscope
(Myeloscope
). bull Neurol Inst.
New Work 7
:178-189, 1938
26) Pool JL:Myeloscopy:
Intraspinal endoscopy. Surgery 2
:169-182, 1942
27) Powell MP, Torrens MJ, Thomson JLG, et al:Isodense coll-
oid cysts of the third ventricle
:A diagnostic and therapeutic problem resolved by ventriculoscopy. Neurosurgery 13
:234- 237, 1983
28) Romodanov AP, Pedachenko GA:Hemorrhagical Stroke
Kiev
:Zdorowje, 1971
29) Stern EL:The spinoscope:
A new instrument for visualizing the spinal canal and its contents. Med Rec 143
:31-32, 1936
30) Vigouroux RP, Gondin OS, Guillemain P:The choice of themanagement in spontaneous brain hematomas
(258 cases from
Marseille’s neurosurgeons since CT scan use
):Abstracts of the seventh European Congress of Neurosurgery. Brussels, pp132
(Abstract
), 1983
31) Weisberg LA:Computerized tomography in intracranial he-
morrhage. Arch Neurol 36
:422-426, 1979
32) Yamamoto F, Eguchi G, Yoshimura K, et al:Massive trau-