Original Article
© 2013 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses /by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Effect of Age and Early Intervention with a Systemic Steroid, Intravenous Immunoglobulin or Amniotic Membrane Transplantation
on the Ocular Outcomes of Patients with Stevens-Johnson Syndrome
Kyeong Hwan Kim1,2, Sung Wook Park1,2, Mee Kum Kim1,2, Won Ryang Wee1,2
1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea
2Laboratory of Corneal Regenerative Medicine and Ocular Immunology, Seoul Artificial Eye Center, Seoul National University Hos- pital Clinical Research Institute, Seoul, Korea
Purpose: This retrospective observational case series of fifty-one consecutive patients referred to the eye clinic with acute-stage Stevens-Johnson syndrome (SJS) or toxic epidermal necrolysis (TEN) from 1995 to 2011 examines the effect of early treatment with a systemic corticosteroid or intravenous immunoglobulin (IVIG) on the ocular outcomes in patients with SJS or TEN.
Methods: All patients were classified by age (≤18 years vs. >18 years) and analyzed by treatment modality and early intervention with systemic corticosteroids (≤5 days), IVIG (≤6 days), or amniotic membrane graft trans- plantation (AMT) (≤15 days). The main outcomes were best-corrected visual acuity (BCVA) in logarithm of the minimum angle of resolution (logMAR) and ocular involvement scores (OIS, 0-12), which were calculated based on the presence of superficial punctate keratitis, epithelial defect, conjunctivalization, neovasculariza- tion, corneal opacity, keratinization, hyperemia, symblepharon, trichiasis, mucocutaneous junction involve- ment, meibomian gland involvement, and punctal damage.
Results: The mean logMAR and OIS scores at the initial visit were not significantly different in the pediatric group (logMAR = 0.44, OIS = 2.76, n = 17) or the adult group (logMAR = 0.60, OIS = 2.21, n = 34). At the final follow-up, the logMAR and OIS had improved significantly in the adult group (p = 0.0002, p = 0.023, respec- tively), but not in the pediatric group. Early intervention with IVIG or corticosteroids significantly improved the mean BCVA and OIS in the adult group (p = 0.043 and p = 0.024, respectively for IVIG; p = 0.002 and p = 0.034, respectively for corticosteroid). AMT was found to be associated with a significantly improved BCVA or OIS in the late treatment group or the group with a better initial OIS (p = 0.043 and p = 0.043, respectively for BCVA;
p = 0.042 and p = 0.041, respectively for OIS).
Conclusions: Our findings suggest that patients with SJS or TEN who are aged 18 years or less have poorer ocular outcomes than older patients and that early treatment with steroid or immunoglobulin therapy improves ocular outcomes.
Key Words: Amniotic membrane graft transplantation, Immunoglobulins, Ocular complication, Steroids, Ste- vens-Johnson syndrome
Received: September 1, 2012 Accepted: January 3, 2013
Corresponding Author: Mee Kum Kim, MD, PhD. Department of Oph- thalmology, Seoul National University College of Medicine, #103 Dae- hak-ro, Jongno-gu, Seoul 110-799, Korea. Tel: 82-2-2072-2665, Fax: 82-2- 741-3187, E-mail: [email protected]
Presented in part at the annual meeting of Korean Ophthalmological Society, Goyang, Korea, November 2011 and the American Society of Cataract and Re- fractive Surgery Symposium on Cataract, Intraocular Lens, and Refractive Sur- gery, Chicago, USA, April 2012.
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are severe blistering diseases of the skin and mucous membranes that are mostly caused by adverse drug reactions. They have a low incidence rate but a high level of mortality [1,2]. SJS is defined by epidermal detach- ment of less than 10% of the body surface area (BSA) and TEN as detachment of more than 30% of the BSA [3,4].
Generally, both SJS and TEN are used as a diagnosis when the lesion involves between 10 and 30% of the skin. Oph- thalmic involvement is common later in the disease, and in severe cases bilateral blinding due to corneal scarring and vascularization may occur [5-7].
Recent research indicates that immunologic activation of cytotoxic CD8 T cells, macrophages, IL-6, TNF-α, soluble Fas ligand (FasL), and others are involved in the pathogen- esis of SJS and TEN [8-11]. Many studies have focused on treatments that modify the immunologic response, such as corticosteroids and intravenous immunoglobulin (IVIG), [12] in an effort to reduce the cytokine storm and Fas-FasL induced apoptosis. Amniotic membrane graft transplanta- tion (AMT) may be an another option for diminishing ocu- lar inflammation in the acute stage [13].
However, no standardized treatment has been estab- lished for SJS or TEN patients with eye involvement. Few studies have compared the effects of different treatments (such as oral steroids or IVIG) on ocular outcomes in the acute stage. Furthermore, according to our clinical experi- ence, the effect of treatment on ocular inflammation tends to be age-dependent. Several studies have reported that prognosis (mortality and treatment outcome) differ be- tween children and adults [4,14-16], but no study has ad- dressed the effect of different treatments on the ocular outcomes in these groups.
Accordingly, the aim of the present study is to assess the effects of different treatments for SJS and TEN on ocular outcomes with respect to patient age.
Materials and Methods
The institutional review board of Seoul National Univer- sity Hospital (SNUH) approved the study protocol (H-1110- 112-383) and the protocol complied with the tenets of the Declaration of Helsinki.
Patients
In this retrospective observational case series, we exam- ined the medical records of 51 consecutive patients who presented or were referred to the eye clinic at SNUH when they were in acute-stage SJS or TEN from 1995 to 2011.
All medical records were obtained from the SNUH data- base and patients were identified based on the International Classification of Diseases 10th revision using the code L51.1 for SJS and L51.2 for TEN. All diagnoses were based on clinical history or biopsy results and patients were clas- sified by the criteria outlined by Bastuji-Garin et al. [17].
Patients were excluded if there was no ophthalmic in- volvement during the acute stage, no follow-up visit at the eye clinic after the acute stage, no documentation by a cor- neal specialist, if disease onset occurred during corticoste- roid use for control of another disease, or if there was a di- agnosis of erythema multiforme major or minor.
Patients were classified by age (≤18 years vs. >18 years), treatment modality, time from onset of acute symptoms to treatment initiation (≤5 days for steroid, ≤6 days for im- munoglobulin, or ≤15 days for AMT), and severity of ocu- lar involvement at the initial visit (≤6 points of ocular involvement score [OIS] vs. >6 points of OIS, see below).
Disease onset was defined as the day when the mucocuta- neous lesion first developed.
Statistical methods
Statistical analysis was performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). The Wilcoxon signed rank test and the Mann-Whitney U-test were used for continu- ous variables and Pearson’s chi-square test or Fisher’s exact test were used for categorical variables. Logistic regression analysis was used to calculate odds ratios. Statistical sig- nificance was accepted for p-values of <0.05.
Visual acuity and ocular involvement scores
Best-corrected visual acuity (BCVA) was tested at a dis- tance of 5 m using the Snellen chart (Hahn’s standard test chart; Hanil, Seoul, Korea) and results are presented as the logarithms of the minimal angle of resolution (logMAR) values.
All data on ocular involvement, which was documented by a corneal specialist, was reviewed and the OIS was cal-
culated using criteria adapted from Sotozono et al. [18], with some modification. Briefly, OIS considers corneal complications (superficial punctate keratitis, epithelial de- fects, conjunctivalization, neovascularization, corneal opacity, and keratinization), conjunctival complications (hyperemia and symblepharon), and lid complications (tri- chiasis, mucocutaneous junction involvement, meibomian gland involvement, and punctal damage). The presence of each component was valued as 1 point and the sum (0 to 12 points) was used to indicate overall OIS.
Results
Patient characteristics
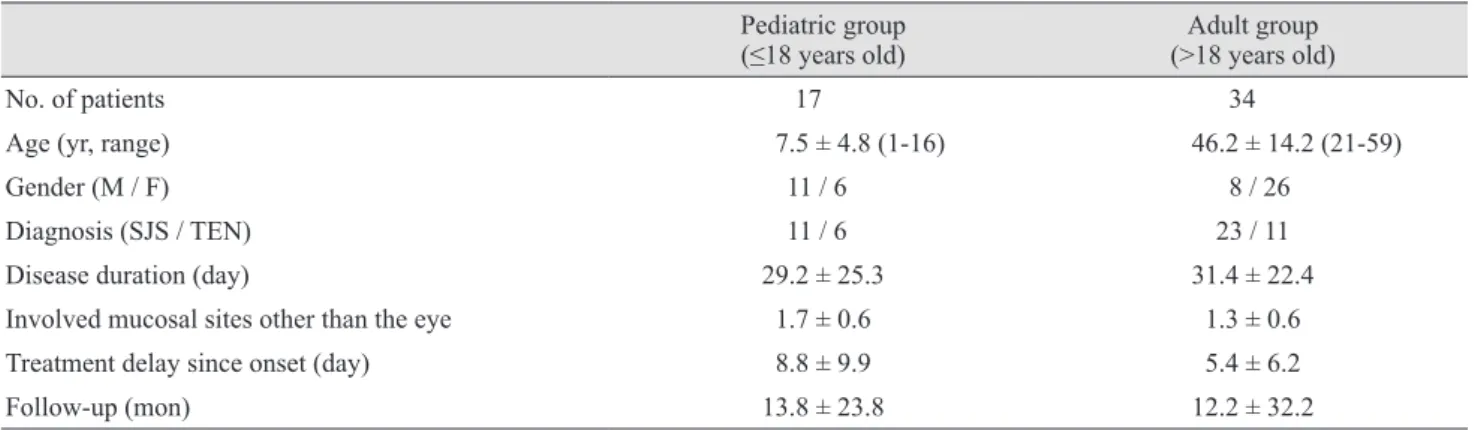
We first examined the demographic and clinical charac- teristics of the 51 enrolled patients (Table 1). Clinical out- comes of representative cases enrolled in this study are shown in Appendix 1. There was a significantly greater proportion of males in the pediatric group and females in the adult group (p = 0.004, Pearson’s chi-square test). Pedi- atric patients had significantly more extraocular mucosal involvement (p = 0.008, Pearson’s chi-square test). There were no other significant demographic differences between the groups.
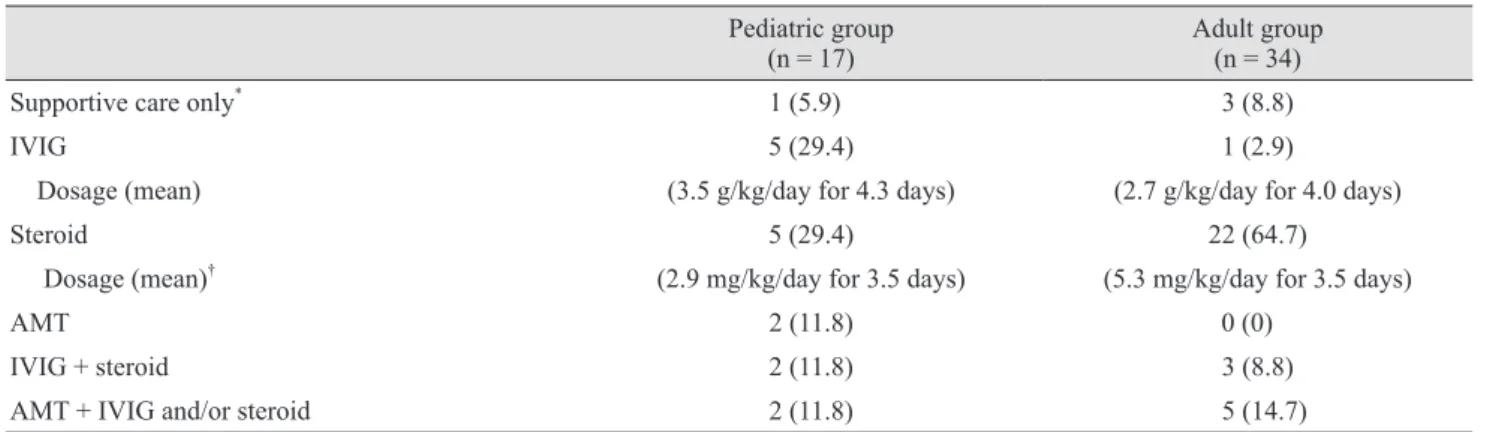
Pediatric patients were more likely to be given IVIG while adult patients were more likely to be given systemic corticosteroid (p = 0.012 and 0.036, respectively; Fisher’s exact test) (Table 2). Corticosteroids were administered at 2.93 ± 1.94 mg/kg/day (interquartile range, 0.75 to 5.09) for 3.50 ± 2.65 days (interquartile range, 1.25 to 6.25) in the
younger group, and 5.28 ± 3.60 mg/kg/day (interquartile range, 3.33 to 5.50) for 3.47 ± 2.09 days (interquartile range, 2.00 to 4.00) in the older group. IVIGs were admin- istered as 3.50 ± 1.52 g/kg/day (interquartile range, 2.00 to 4.50) for 4.33 ± 1.03 days (interquartile range, 3.75 to 5.25) in the younger group, and 2.67 ± 0.58 g/kg/day (interquar- tile range, 2.00 to 3.00) for 4.00 ± 1.00 days (interquartile range, 3.00 to 4.00) in the older group. In these two groups, treatment modality was not found to affect ocular out- comes when compared to supportive care only (as indicat- ed by logMAR and OIS). However, IVIG and corticoste- roid treatment tended to provide some benefit (Table 3).
AMT was first performed in October, 2003 in this case se- ries and cryopreserved amniotic membrane was grafted to the ocular surface to fully cover the lid margins and palpe- bral conjunctiva as described by other authors [19,20]. Sup- portive care performed in this case series includes careful monitoring of fluid balance, respiratory function, nutri- tional requirements, and appropriate wound care [21].
Visual acuities
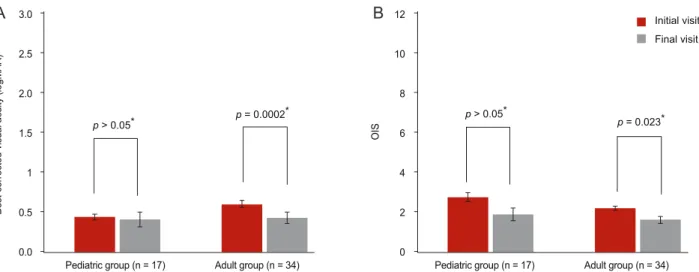
Next, we evaluated whether an improvement in visual acuity could be achieved by intervention, and whether this visual benefit is dependent on the age or the time of treat- ment initiation within each age group. Mean logMAR val- ues in the pediatric group were similar at initial and final visits (0.44 ± 0.28 vs. 0.41 ± 0.77; p = 0.310, Wilcoxon’s signed rank test) (Fig. 1A). Analysis of subgroups of the pediatric patients with respect to treatment modality and time of treatment initiation also indicated no significant
Table 1. Baseline demographic characteristics of enrolled patients
Pediatric group
(≤18 years old) Adult group
(>18 years old)
No. of patients 17 34
Age (yr, range) 7.5 ± 4.8 (1-16) 46.2 ± 14.2 (21-59)
Gender (M / F) 11 / 6 8 / 26
Diagnosis (SJS / TEN) 11 / 6 23 / 11
Disease duration (day) 29.2 ± 25.3 31.4 ± 22.4
Involved mucosal sites other than the eye 1.7 ± 0.6 1.3 ± 0.6
Treatment delay since onset (day) 8.8 ± 9.9 5.4 ± 6.2
Follow-up (mon) 13.8 ± 23.8 12.2 ± 32.2
Values are presented as number or mean ± SD.
SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis.
change in logMAR between initial and final visits (p >
0.05, Wilcoxon’s signed rank test). In contrast, the mean logMAR of the adult patients improved significantly over the same period (0.60 ± 0.57 vs. 0.43 ± 0.84; p = 0.0002, Wilcoxon’s signed rank test) (Fig. 1A). However, mean log- MAR values at initial and final visits were not significantly different in each pediatric or adult groups (p > 0.05, Mann- Whitney U-test) (Fig. 1A).
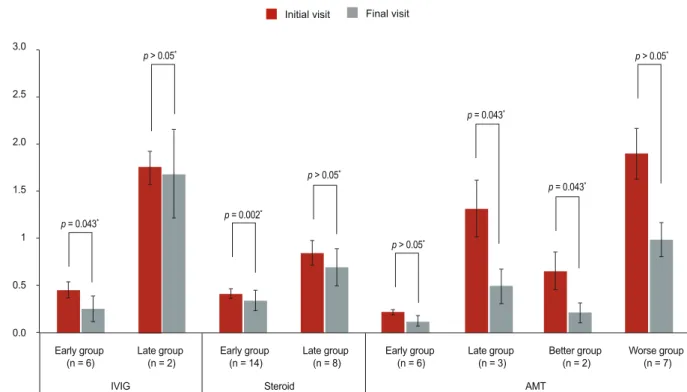
Early treatment of adult patients with IVIG (≤6 days) was found to be associated with a significantly improved logMAR at final visit (initial visit, 0.45 ± 0.41; final visit, 0.25 ± 0.66; p = 0.043, Wilcoxon’s signed rank test) (Fig. 2).
In addition, early treatment in adult patients with systemic corticosteroids (≤5 days) was associated with a significant- ly improved logMAR at final visit (initial visit, 0.41 ± 0.37;
final visit, 0.34 ± 0.80; p = 0.002, Wilcoxon’s signed rank test) (Fig. 2).
All patients with OISs of less than 6 who were treated by
AMT had significantly improved logMAR values (initial visit, 0.65 ± 0.56; final visit, 0.21 ± 0.29; p = 0.043, Wilcox- on’s signed rank test) (Fig. 2). In addition, the mean log- MAR of patients treated with AMT 15 days after disease onset improved significantly (1.31 ± 1.04 vs. 0.49 ± 0.62; p
= 0.043, Wilcoxon’s signed rank test) (Fig. 2).
Ocular involvement
Finally, we assessed whether ocular involvement is im- proved by intervention and whether improvements are de- pendent on age, ocular severity, or the timing or types of interventions. The pediatric group showed no significant difference in mean OIS between initial and final visits (p
= 0.076, Wilcoxon’s signed rank test) (Fig. 1B). However, the adult group showed a significant improvement in mean OIS (p = 0.023, Wilcoxon’s signed rank test) (Fig. 1B).
Comparison of individual components of the OIS in the Table 2. Treatment characteristics of enrolled patients
Pediatric group
(n = 17) Adult group
(n = 34)
Supportive care only* 1 (5.9) 3 (8.8)
IVIG 5 (29.4) 1 (2.9)
Dosage (mean) (3.5 g/kg/day for 4.3 days) (2.7 g/kg/day for 4.0 days)
Steroid 5 (29.4) 22 (64.7)
Dosage (mean)† (2.9 mg/kg/day for 3.5 days) (5.3 mg/kg/day for 3.5 days)
AMT 2 (11.8) 0 (0)
IVIG + steroid 2 (11.8) 3 (8.8)
AMT + IVIG and/or steroid 2 (11.8) 5 (14.7)
Values are presented as number of patients (%) unless otherwise indicated.
IVIG = intravenous immunoglobulin; AMT = amniotic membrane graft transplantation.
*Supportive care includes adequate control of environmental temperature at 30°C to 32°C, proper fluid balance management and wound care. And all other treatment modalities were accompanied by supportive care; †Data are presented as hydrocortisone equivalent dose.
Table 3. Benefits provided by each treatment modality as compared with conservative treatment
BCVA Ocular involvement
Supportive care only 1 1
IVIG 1.2 (0.5-3.0) 1.8 (0.4-9.6)
Steroid 1.3 (0.6-2.9) 2.4 (0.5-12.2)
AMT 0.8 (0.2-3.7) 1.5 (0.2-12.5)
IVIG + steroid 0.7 ( 0.3-1.5) 0.6 (0.1-3.3)
AMT + IVIG and/or steroid 1.1 (0.5-2.8) 2.6 (0.5-13.3)
Data are presented as odds ratio (95% confidence intervals) for improvements in visual acuity and ocular involvement. Logistic regression analysis was used to calculate odds ratios.
BCVA = best-corrected visual acuity; IVIG = intravenous immunoglobulin; AMT = amniotic membrane graft transplantation.
pediatric and adult groups indicated no significant differ- ences at initial and final visits (p > 0.05 for all, Fisher’s ex- act test and chi-square test) (Fig. 1B).
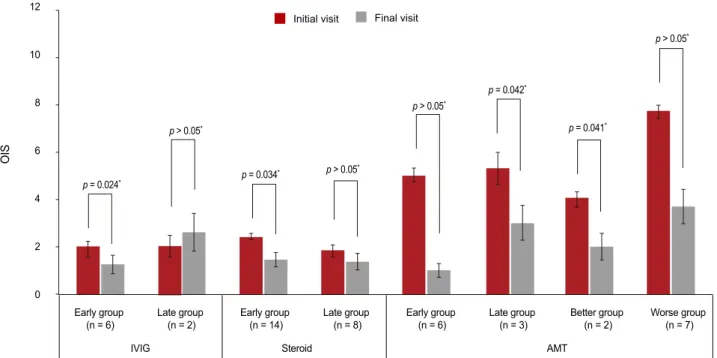
Analysis of treatment modality and time of treatment onset in pediatric patients indicated no significant differ- ences in mean OIS (p > 0.05 for both, Wilcoxon’s signed rank test). However, adult patients treated early (≤6 days) with IVIG showed a significantly better mean OIS than those treated later (2.00 ± 1.13 vs. 1.24 ± 1.86; p = 0.024, Wilcoxon’s signed rank test) (Fig. 3). In addition, adult treated early (≤5 days) with corticosteroids also showed a significantly better mean OIS (2.41 ± 1.00 vs. 1.44 ± 2.13; p
= 0.034, Wilcoxon’s signed rank test) (Fig. 3).
All patients with OISs of <6 who were given AMT treat- ment had a significantly better mean OIS than patients with OISs of >6 (4.00 ± 0.89 vs. 2.00 ± 1.55; p = 0.041, Wil- coxon’s signed rank test) (Fig. 1B). Furthermore, OIS in all patients treated with AMT more than 15 days after disease onset improved significantly (5.29 ± 2.36 vs. 3.00 ± 2.52; p
= 0.042, Wilcoxon’s signed rank test) (Fig. 3).
Discussion
This study shows that pediatric patients with SJS or TEN under 18 years of age had poorer ocular outcomes,
measured via OIS, than adult patients. Furthermore, our findings suggest that early treatment with corticosteroid or immunoglobulin therapy significantly improves ocular outcomes in adult patients. These findings are of impor- tance because they provide information on relative prog- noses based on patient age during the acute stage and be- cause they prompt intervention with systemic anti- inflammatory drugs during the acute stage, which might beneficially modify the ocular course of disease.
SJS and TEN are characterized by marked keratinocyte apoptosis in the epidermis, dermo-epidermal separation, and overall epidermal necrosis [22]. Although their patho- geneses are not fully understood, several lines of evidence indicate that disruption of the immune system is involved.
Viard et al. [11] showed that soluble FasL is elevated in pa- tients with SJS or TEN and that the expression of FasL is upregulated on keratinocytes. Abe et al. [8] found that the peripheral blood mononuclear cells of SJS patients secrete soluble FasL when exposed to drugs. Others have shown that massive apoptosis of keratinocytes is induced by per- forin or granzyme B, which are released by drug-specific cytotoxic T cells [10,23]. Granulysin is secreted by activat- ed CD8+ T cells, NK cells, and NKT cells, and also ap- pears to be involved in keratinocyte apoptosis [9]. Based on the pathogeneses of SJS and TEN, it could be assumed that systemic steroid or IVIG therapy might reduce acute
Initial visit
p > 0.05*
p = 0.023*
p > 0.05* p = 0.0002*
Final visit
Pediatric group (n = 17) 12
10 8 6 4 2 0 3.0
2.5 2.0 1.5 1 0.5 0.0
OIS
Best-corrected visual acuity (logMAR)
Adult group (n = 34) Pediatric group (n = 17) Adult group (n = 34)
Fig. 1. Changes in visual acuities and ocular involvement score (OIS) with respect to patient age. (A) Mean logarithms of the minimal an- gle of resolution (logMAR) values in the pediatric group were similar at initial and final visits. In contrast, the mean logMAR of the adult patients improved significantly over the same period. (B) The pediatric group also showed no significant difference in mean OIS between initial and final visits. However, the adult group showed a significant improvement in mean OIS. There was no significant between group differences in each visits. Pediatric group = who are aged 18 years or less; adult group = who are over 18 years old. *Wilcoxon’s signed rank test.
A B
stage inflammation.
Systemic corticosteroids, which have well-known anti- inflammatory and immunosuppressive effects, have long been used to treat SJS and TEN. Multiple mechanisms have been reported to be involved in immunosuppression, including the stabilization of lysosomal membranes, the suppression of prostaglandin synthesis, the inhibition of the transcriptions of pro-inflammatory cytokines (IL-1, IL- 2, IL-6, IFN-γ, and TNF-α), impairments in monocyte and macrophage function, and reductions in the numbers of circulating CD4+ T cells. However, there is little clinical evidence of their efficacy in reducing ocular disease dur- ing acute stage SJS or TEN. Anecdotal reports indicate a beneficial effect for systemic corticosteroid treatment, but study populations were small [24,25]. On the other hand, others have reported no benefit for systemic corticosteroid treatment [6]. Accordingly, more studies are needed to de- termine whether systemic steroids reduce ocular inflam- mation in SJS and TEN patients. In the present study, we
found that visual acuity and ocular involvement signifi- cantly improved after instituting systemic corticosteroids, especially when administered within 5 days of acute symptom onset. That is, the present study supports previ- ous reports regarding the beneficial effects of steroids in SJS and TEN. Furthermore, previous studies and the pres- ent study support the notion that the control of severe in- flammation as early as possible is associated with fewer ocular sequelae. Inflammation is believed to be a principal pathogenic factor in limbal stem cell deficiency, which manifests clinically as a loss of palisades of Vogt, keratini- zation, and opacity in chronic-stage SJS or TEN [18]. In- flammation is also associated with loss of goblet cells in conjunctivae, which could result in severely dry eyes and ocular surface complications [5,6]. Furthermore, in the present study early treatment appeared to save some cells from total destruction, and thus, reduced ocular surface damage. On the other hand, systemic corticosteroid treat- ment could lead to numerous adverse effects, including
p > 0.05*
p = 0.002*
p > 0.05*
p > 0.05*
p = 0.043* p = 0.043*
p = 0.043*
p > 0.05* 3.0
2.5
2.0
1.5
1
0.5
0.0
Best-corrected visual acuity (logMAR)
Early group
(n = 6) Late group (n = 2)
IVIG Steroid
Early group
(n = 14) Late group
(n = 8) Early group
(n = 6) Late group (n = 3)
AMT
Better group
(n = 2) Worse group (n = 7) Initial visit Final visit
Fig. 2. Changes in visual acuities of the adult group with respect to treatment modality and time of treatment initiation. Early treatment of adult patients with intravenous immunoglobulin (IVIG) or with systemic corticosteroids was found to be associated with a signifi- cantly improved logMAR at final visit. The mean logMAR of patients treated with amniotic membrane graft transplantation (AMT) im- proved significantly by the final visit if patients were treated 15 days after disease onset or if their ocular involvement score was less than 6 at the initial visit. There was no significant between group differences in each visits. Early group = patients with treatment initiation ≤6 days for IVIG, ≤5 days for corticosteroid, or ≤15 days for AMT. Late group = treatment initiation >6 days for IVIG, >5 days for cortico- steroid, or >15 days for AMT. Better group = patients with ocular involvement scores (OIS) of less than 6 at initial visit. Worse group = patients with OIS over 6 at initial visit. *Wilcoxon’s signed rank test.
gastrointestinal bleeding, which is accompanied by a high risk of mortality [26,27]. The more BSA involved, the high- er the risk of mortality. Generally, the risk is considered se- rious in patients with body surface area involvement of more than 30% [28,29]. Therefore, close monitoring is rec- ommended in patients being treated with systemic steroids when BSA involvement exceeds this level.
IVIG has also been used to treat SJS and TEN based on the belief that these antibodies prevent keratinocyte apop- tosis resulting from Fas-FasL interaction [11]. However, the therapeutic efficacy and outcome of IVIG treatment re- mains controversial and no definitive study has addressed the effect of IVIG on ocular outcome. In the present study, we found that IVIG led to significant improvements in vi- sual acuity and ocular involvement, especially when it was administered within 6 days of disease onset. Considering that the level of FasL increases several days before the on- set of clinical manifestations, and decreases rapidly to reach the normal range at 5 days after disease onset in pa- tients with SJS or TEN [30], early IVIG treatment may provide relief by saturating the Fas (CD95) binding site.
Furthermore, the high frequency of infectious complica-
tions associated with corticosteroid treatment may be re- duced by IVIG, which has anti-infectious and immuno- modulatory properties [31,32]. In addition, IVIG could help to prevention of fluid loss, a significant problem in SJS and TEN, because of the osmolal effects of the proteins them- selves [12]. Contrary to our results, Yip et al. [33] conclud- ed that IVIG did not reduce the severity of ocular compli- cations in patients with SJS or TEN. However, they enrolled a small number of patients, and only one patient was treated with IVIG alone; other patients were treated with IVIG either before or after steroid treatment.
We examined the effect of AMT during acute stage SJS and TEN. John et al. [19] initially reported that AMT was an effective treatment in patients with acute-stage TEN, and in subsequent studies found that AMT provides ocular benefits in patients with acute-stage SJS or TEN [20,34,35].
Recently, Gregory [13] found that AMT performed during the 10 days following disease onset reduced the risks of ocular sequelae. In the present study, we found that AMT significantly improved visual acuity and ocular outcome in patients with less severe ocular involvement (OIS <6), which suggests that AMT alone is insufficient to attenuate
p > 0.05*
p = 0.034* p > 0.05*
p > 0.05*
p = 0.041* p = 0.042*
p = 0.024*
p > 0.05* 12
10
8
6
4
2
0
OIS
Early group
(n = 6) Late group (n = 2) IVIG
Early group
(n = 14) Late group
(n = 8) Early group
(n = 6) Late group (n = 3)
AMT Steroid
Better group
(n = 2) Worse group (n = 7) Initial visit Final visit
Fig. 3. Changes in ocular involvement score (OIS) of the adult group with respect to treatment modality and time of treatment initiation.
Early treatment of adult patients with intravenous immunoglobulin (IVIG) or with systemic corticosteroids was found to be associated with a significantly improved OIS at final visit. The mean OIS of patients who were treated with amniotic membrane graft transplantation (AMT) improved significantly in the late group and worse group. There was no significant between group differences in each visits. Early group = patients with treatment initiation ≤6 days for IVIG, ≤5 days for corticosteroid, or ≤15 days for AMT. Late group = treatment ini- tiation >6 days for IVIG, >5 days for corticosteroid, or >15 days for AMT. Better group = patients with OIS of less than 6 at initial visit.
Worse group = patients with OIS over 6 at initial visit. *Wilcoxon’s signed rank test.
ocular inflammation in severe cases. Further study on the effects of AMT in SJS and TEN is necessary.
Interestingly, we found corticosteroid and IVIG provid- ed benefits when compared with conservative treatment.
The odds ratios for improvements in visual acuity and oc- ular involvement in adult patients treated with corticosteri- ods were 1.2 and 1.8, respectively, and 1.3 and 2.4, respec- tively, for adult patients treated with IVIG. Although these findings were not statistically significant, presumably due to the small sizes of the conservative treatment subgroup, they still provide a clue of possible benefit.
Another noteworthy finding of the present study was that prognosis appeared to be dependent on age. In partic- ular, our results indicate that children given different treat- ments showed no significant improvements in visual acuity or ocular involvement relative to patients given best sup- portive care. This finding stands in contrast with those of several other reports that concluded SJS and TEN are milder and associated with lower mortality in children.
However, these findings do concur with a recent study, in which higher long-term complications, including ocular sequelae, were reported in children compared with adults with SJS or TEN [14]. Taken together, it appears that ocu- lar prognoses and treatment outcomes of children are quite different from those of adults. Further larger-scale investi- gations are warranted on this issue.
The main limitation of this study was that it did not have a prospective, randomized, controlled design, which would not be ethically tolerable in practice. Given the disease se- verities involved, we are satisfied with the retrospective design adopted. Second, some patients followed long-term by several examiners were included in the present study, and thus inter-individual measurement bias of ocular sta- tus was not fully excluded. Third, the small numbers of patients involved in the subgroup analyses of AMT and IVIG treatments might have affected our results.
In conclusion, our study indicates that early treatment with corticosteroid or immunoglobulin improves ocular outcomes in elderly patients, and suggests that patients aged 18 years or less with SJS or TEN have poorer ocular outcomes than adult patients.
Conflict of Interest
No potential conflict of interest relevant to this article
was reported.
References
1. Chan HL, Stern RS, Arndt KA, et al. The incidence of ery- thema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis: a population-based study with partic- ular reference to reactions caused by drugs among outpa- tients. Arch Dermatol 1990;126:43-7.
2. Roujeau JC, Kelly JP, Naldi L, et al. Medication use and the risk of Stevens-Johnson syndrome or toxic epidermal necrolysis. N Engl J Med 1995;333:1600-7.
3. Roujeau JC. The spectrum of Stevens-Johnson syndrome and toxic epidermal necrolysis: a clinical classification. J Invest Dermatol 1994;102:28S-30S.
4. Ruiz-Maldonado R. Acute disseminated epidermal necro- sis types 1, 2, and 3: study of sixty cases. J Am Acad Der- matol 1985;13:623-35.
5. Chang YS, Huang FC, Tseng SH, et al. Erythema multi- forme, Stevens-Johnson syndrome, and toxic epidermal necrolysis: acute ocular manifestations, causes, and man- agement. Cornea 2007;26:123-9.
6. Power WJ, Ghoraishi M, Merayo-Lloves J, et al. Analysis of the acute ophthalmic manifestations of the erythema multi- forme/Stevens-Johnson syndrome/toxic epidermal necroly- sis disease spectrum. Ophthalmology 1995;102:1669-76.
7. Yip LW, Thong BY, Lim J, et al. Ocular manifestations and complications of Stevens-Johnson syndrome and toxic epi- dermal necrolysis: an Asian series. Allergy 2007;62:527-31.
8. Abe R, Shimizu T, Shibaki A, et al. Toxic epidermal necrolysis and Stevens-Johnson syndrome are induced by soluble Fas ligand. Am J Pathol 2003;162:1515-20.
9. Chung WH, Hung SI, Yang JY, et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens- Johnson syndrome and toxic epidermal necrolysis. Nat Med 2008;14:1343-50.
10. Nassif A, Bensussan A, Boumsell L, et al. Toxic epidermal necrolysis: effector cells are drug-specific cytotoxic T cells.
J Allergy Clin Immunol 2004;114:1209-15.
11. Viard I, Wehrli P, Bullani R, et al. Inhibition of toxic epi- dermal necrolysis by blockade of CD95 with human intra- venous immunoglobulin. Science 1998;282:490-3.
12. Prins C, Kerdel FA, Padilla RS, et al. Toxic epidermal necrolysis-intravenous immunoglobulin: treatment of toxic epidermal necrolysis with high-dose intravenous immuno-
globulins: multicenter retrospective analysis of 48 consecu- tive cases. Arch Dermatol 2003;139:26-32.
13. Gregory DG. Treatment of acute Stevens-Johnson syn- drome and toxic epidermal necrolysis using amniotic mem- brane: a review of 10 consecutive cases. Ophthalmology 2011;118:908-14.
14. Finkelstein Y, Soon GS, Acuna P, et al. Recurrence and outcomes of Stevens-Johnson syndrome and toxic epider- mal necrolysis in children. Pediatrics 2011;128:723-8.
15. Koh MJ, Tay YK. Stevens-Johnson syndrome and toxic epidermal necrolysis in Asian children. J Am Acad Derma- tol 2010;62:54-60.
16. Prendiville JS, Hebert AA, Greenwald MJ, Esterly NB.
Management of Stevens-Johnson syndrome and toxic epi- dermal necrolysis in children. J Pediatr 1989;115:881-7.
17. Bastuji-Garin S, Rzany B, Stern RS, et al. Clinical classifi- cation of cases of toxic epidermal necrolysis, Stevens-John- son syndrome, and erythema multiforme. Arch Dermatol 1993;129:92-6.
18. Sotozono C, Ang LP, Koizumi N, et al. New grading sys- tem for the evaluation of chronic ocular manifestations in patients with Stevens-Johnson syndrome. Ophthalmology 2007;114:1294-302.
19. John T, Foulks GN, John ME, et al. Amniotic membrane in the surgical management of acute toxic epidermal necroly- sis. Ophthalmology 2002;109:351-60.
20. Kobayashi A, Yoshita T, Sugiyama K, et al. Amniotic membrane transplantation in acute phase of toxic epider- mal necrolysis with severe corneal involvement. Ophthal- mology 2006;113:126-32.
21. Rohrer TE, Ahmed AR. Toxic epidermal necrolysis. Int J Dermatol 1991;30:457-66.
22. Roujeau JC, Stern RS. Severe adverse cutaneous reactions to drugs. N Engl J Med 1994;331:1272-85.
23. Nassif A, Bensussan A, Dorothre G, et al. Drug specific
cytotoxic T-cells in the skin lesions of a patient with toxic epidermal necrolysis. J Invest Dermatol 2002;118:728-33.
24. Araki Y, Sotozono C, Inatomi T, et al. Successful treatment of Stevens-Johnson syndrome with steroid pulse therapy at disease onset. Am J Ophthalmol 2009;147:1004-11, 1011.e1.
25. Yagi T, Sotozono C, Tanaka M, et al. Cytokine storm aris- ing on the ocular surface in a patient with Stevens-Johnson syndrome. Br J Ophthalmol 2011;95:1030-1.
26. Ginsburg CM. Stevens-Johnson syndrome in children. Pe- diatr Infect Dis 1982;1:155-8.
27. Halebian PH, Shires GT. Burn unit treatment of acute, se- vere exfoliating disorders. Annu Rev Med 1989;40:137-47.
28. Mockenhaupt M, Viboud C, Dunant A, et al. Stevens-John- son syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs:
the EuroSCAR-study. J Invest Dermatol 2008;128:35-44.
29. Yamane Y, Aihara M, Ikezawa Z. Analysis of Stevens- Johnson syndrome and toxic epidermal necrolysis in Japan from 2000 to 2006. Allergol Int 2007;56:419-25.
30. Murata J, Abe R, Shimizu H. Increased soluble Fas ligand levels in patients with Stevens-Johnson syndrome and toxic epidermal necrolysis preceding skin detachment. J Allergy Clin Immunol 2008;122:992-1000.
31. Dwyer JM. Manipulating the immune system with im- mune globulin. N Engl J Med 1992;326:107-16.
32. Kazatchkine MD, Kaveri SV. Immunomodulation of auto- immune and inflammatory diseases with intravenous im- mune globulin. N Engl J Med 2001;345:747-55.
33. Yip LW, Thong BY, Tan AW, et al. High-dose intravenous immunoglobulin in the treatment of toxic epidermal necroly- sis: a study of ocular benefits. Eye (Lond) 2005;19:846-53.
34. Muqit MM, Ellingham RB, Daniel C. Technique of amniotic membrane transplant dressing in the management of acute Stevens-Johnson syndrome. Br J Ophthalmol 2007;91:1536.
35. Tandon A, Cackett P, Mulvihill A, Fleck B. Amniotic
membrane grafting for conjunctival and lid surface disease in the acute phase of toxic epidermal necrolysis. J AAPOS 2007;11:612-3.
Appendix 1. Clinical outcomes of representative cases enrolled in this study. (A-C) Gross and slitlamp photographs of 7-year-old girl with Stevens-Johnson syndrome at initial visit (A,B) and last visit (C). (D-F) Slitlamp photograph of a 59-year-old woman with toxic epi- dermal necrolysis at initial visit (D,E) and at last visit (F). (G-I) 31-Year-old man with Stevens-Johnson syndrome at initial visit (G) under- went amniotic membrane graft transplantation (H), which resulted in clinical improvement at last visit (I).
A
D
G
B
E
H
C
F
I