31
서 론
복강경 담낭절제술의 이점들이 처음 보고된 이후 복강경 수술은 다양한 기구의 개발과 함께 외과 영역에서 급속도 로 발전하고 있다.(1,2) 진단 내시경의 발달과 건강 검진에 대한 일반인의 관심 증가로 전체 위암 중 조기위암이 차지 하는 비율이 증가하고 있으며, 조기위암은 림프절 전이가 드물고 전이가 있더라도 대개 위주변 림프절(perigasstric lymph node)에 국한되므로 여러 가지 다양한 치료법이 제시 되고 있다.(3-7) 최근 조기위암 환자에서 복강경 보조하 위 아전절제술(LADG, Laparoscopy-assisted distal gastrectomy) 이 개복술에 비해 종양학적 손실이 없으면서 복강경 수술 의 여러 이점들을 위암 환자에게 제공함으로써 많은 연구 자들에 의해 시도되고 있으며, 그 결과들이 보고되고 있 다.(8-15)
우리나라 환자의 비만은 서양에 비해 아직 그 정도가 덜 하지만 생활습관 및 여러 가지 환경 요인으로 인하여 점점 더 심각해지고 있다. 비만은 심혈관 질환, 당뇨 등 수술 전 환자의 동반질환의 빈도를 높일 뿐 아니라 수술 중에도 과 다한 지방조직으로 인하여 출혈을 많게 하고 수술시간을 연장시키며 수술 중과 수술 후의 합병증 발생을 증가시키 는 것으로 인식되어 왔다.(16)
이에 저자들은 비만도가 조기위암 환자의 복강경 보조하 위아전절제술에 어떠한 영향을 미치는지를 알아보고자 하 였다.
방 법
1998년 5월부터 2004년 3월까지 동아대학교병원 외과에 서 조기위암으로 복강경 보조하 위아전절제술을 시행 받은
비만도가 조기위암 환자의 복강경 보조하 위아전절제술에 미치는 영향
동아대학교 의과대학 외과학교실, 1내과학교실
최수미․김민찬․이종훈1․김기한․최홍조․김영훈․조세헌․정갑중
The Effects of Obesity for Laparoscopy- Assisted Distal Gastrectomy in Patient with Early Gastric Cancer
Su Mi Choi, M.D., Min Chan Kim, M.D., Jong Hun Lee, M.D.1, Ki Han Kim, M.D., Hong Jo Choi, M.D., Young Hun Kim, M.D., Se Heon Cho, M.D. and Ghap Joong Jung, M.D.
Purpose: Laparoscopy-assisted distal gastrectomy (LADG) has recently been accepted as a feasible and acceptable method for early gastric cancer surgery. Surgeons have long suspected that obesity might increase the intra-operative or postoperative complications. We set out to clarify the effects of obesity on LADG for early gastric cancer treatment.
Methods: We retrospectively reviewed 97 patients who had undergone LADG for early gastric cancer between May 1998 and March 2003. The degree of obesity was based on the Body Mass Index (BMI, kg/m2), with patients assigned to two groups: normal BMI (BMI <23 kg/m2) and high BMI (BMI=
23 kg/m2).
Results: There were no significant differences between the normal and high BMI groups in terms of patients’ charac- teristics, surgical outcomes and postoperative courses, post- operative complication and operation time. However, there was a significant statistical difference in the operation time among the latter four groups (P=0.004). And the male with high BMI group took particularly a longer operation time than female groups with normal BMI (P=0.006) and high BMI (P=0.013).
Conclusion: In LADG patients with early gastric cancer, obesity may affect the operation time, and the male high BMI group takes particularly a longer operation time than the female groups. (J Korean Surg Soc 2005;69:31-35)
Key Words: Laparoscopic gastrectomy, Early gastric can- cer, Obesity
중심 단어: 복강경 위절제술, 조기위암, 비만 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Departments of Surgery and 1Internal Medicine, Dong-A Uni- versity College of Medicine, Busan, Korea
책임저자:김민찬, 부산광역시 서구 동대신동 3가 1번지 ꂕ 602-715, 동아대학교 의과대학 외과학교실 Tel: 051-240-2643, Fax: 051-247-9316
E-mail: [email protected]
접수일:2005년 2월 3일, 게재승인일:2005년 5월 12일 본 논문의 요지는 2004년도 대한위암학회 춘계학술대회에서 포스 터 발표하였음.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 97명의 환자를 대상으로 후향적 조사를 시행하였다.
비만도는 Body Mass Index (BMI, kg/m2)를 이용하여 산출 하였으며, 지수 23 미만을 정상체중군으로 23 이상으로 과 체중군으로 분류하였다. 양 군에서 수술 전 나이, 성별, 원 발 종양의 침습도와 림프절 전이 여부를 비교하였으며 그 외 수술시간, 수혈여부, 절제된 림프절수, 가스배출시기, 수 술 후 2시간 백혈구 수, 술 후 재원일수, 합병증 발생률 등을 비교분석하였다. 수술의 술기는 이미 외과학회지에 발표한 바 있다.(17)
통계분석으로 One-way ANOVA, Fisher's exact test와 unpaired t test를 이용하였고 P값이 0.05 미만일 때를 통계적 으로 유의하다고 판정하였다.
결 과
전체 환자의 평균 BMI는 23.03 kg/m2이었으며, 지수 23을 기준으로 정상체중군은 52명, 과체중군은 45명이었다. 양 군에서 수술 전 나이, 성별, 원발 종양의 침습도와 림프절 전이여부의 차이는 없었다(Table 1).
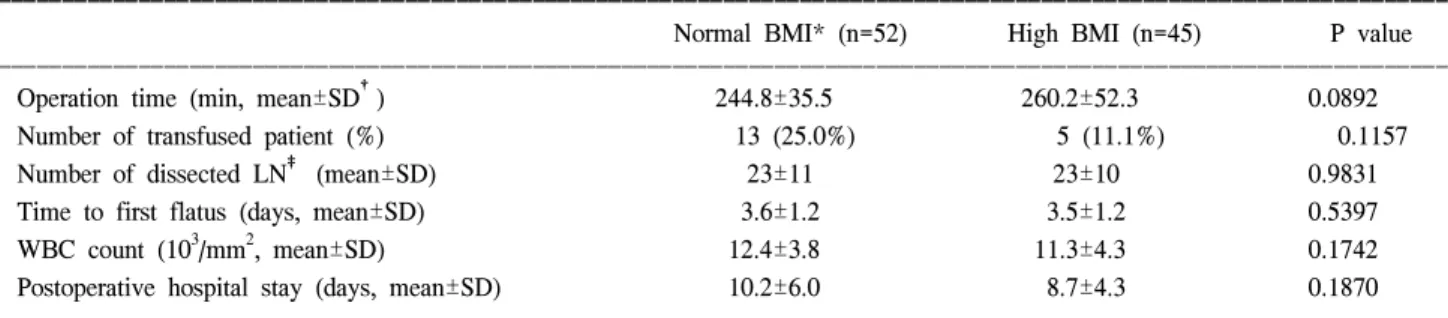
수술 결과들을 비교하면 평균 수술시간은 정상체중군에 서 244.8±35.5분 과체중군에서 260.2±52.3분으로 과체중 군에서 약 15분 가량 길게 나타났으나 양 군간에 통계적으
로 유의한 차이는 없었다(P=0.089)(Table 2). 그러나 비만도 와 남녀 성별에 따른 수술시간의 차이를 알아보기 위하여 환자들을 4군으로 나누어 수술시간을 분석한 결과 과체중 군 남자환자(277.2±52.7분)에서 수술시간이 가장 많이 소 요되었다(P=0.0039). 또한 이는 과체중군 여자환자(P=0.013) 와 정상체중군 여자환자(P=0.006)와 비교했을 때 각각 통계 적으로 유의한 차이를 보였다(Fig. 1). 그 외 수혈여부, 절제 된 림프절의 수, 가스 배출시기, 수술 후 2시간 백혈구 수, 수술 후 재원일수 등은 정상체중군과 과체중군에서 차이가 없었다(Table 2).
97명의 환자 중 2명은 술 후 각각 510일과 44일에 병원에 서 사망하였다. 이 중 한 명은 복강 내 출혈과 여러 번의 재수술로 인한 다발성 장기부전으로 사망하였으며, 다른 한 명은 비장경색으로 재수술을 시행한 후 폐부전으로 호 흡기 치료 중 기도폐색으로 사망하였다. 그 외 합병증은 Table 3과 같이 발생하였고 양 군 간 통계적으로 유의한 차 이는 없었다.
Table 2. Surgical outcomes and postoperative course
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Normal BMI* (n=52) High BMI (n=45) P value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Operation time (min, mean±SD†) 244.8±35.5 260.2±52.3 0.0892
Number of transfused patient (%) 13 (25.0%) 5 (11.1%) 0.1157
Number of dissected LN‡ (mean±SD) 23±11 23±10 0.9831
Time to first flatus (days, mean±SD) 3.6±1.2 3.5±1.2 0.5397
WBC count (103/mm2, mean±SD) 12.4±3.8 11.3±4.3 0.1742
Postoperative hospital stay (days, mean±SD) 10.2±6.0 8.7±4.3 0.1870
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*BMI = body mass index; †SD = standard deviation; ‡LN = lymph node.
Table 1. Patients’ characteristics
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Normal High
BMI* BMI P value
(n=52) (n=45)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ BMI (kg/m2, mean±SD†) 21.0±1.3 25.3±1.8
Age (years, mean±SD) 56±12 55±11 0.5728
Sex (male/female) 29/23 25/20 1.0000
Depth of invasion (m‡/sm§) 39/13 25/20 0.0545 LN∥ metastasis (present/absent) 4/48 3/42 1.0000 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*BMI = body mass index; †SD = standard deviation; ‡m =
mucosa; §sm = submucosa; ∥LN = lymph node. Fig. 1. Analysis of operation times among four groups.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
고 찰
비만은 각종 성인병의 주요 요인일 뿐 아니라 수명을 단 축시키는 중대한 건강 문제이다.(18) 식생활 습관의 서구화 로 우리나라에서도 비만 인구가 점차 증가함에 따라 비만 이 국민건강의 중요한 문제로 대두되고 있다. 비만도의 측 정에는 BMI (Body Mass Index)가 흔히 사용되는데 BMI는 남녀에 공통으로 사용할 수 있고 실제 체지방을 잘 반영하 면서도 체중과 신장만으로 구할 수 있는 매우 간단한 방법 으로 실제 비만에 관한 역학조사에 흔히 사용되고 있 다.(19) 현재 제시되고 있는 비만 판정기준은 2000년 세계보 건기구의 아시아 태평양 지역지침(20)을 기준으로 BMI (kg/m2)가 18.5 미만을 저체중, 18.5∼23이면 정상체중, 23∼
25는 과체중, 25 이상이면 경증비만으로 정의하고 있다. 본 연구에서는 환자들의 평균 BMI가 23.03 kg/m2인 점과 위의 비만 판정기준에 기초하여 지수 23을 기준으로 정상체중군 과 과체중군으로 분류하였다.
본 교실은 1998년부터 복강경 위암 수술을 시행하여 그 결과들을 보고하였으며,(21) 조기위암 환자에서 복강경 보 조하 위아전절제술에 대한 개복술을 비교 연구하여 최근 발표하였다.(17) 개복 및 복강경 위암 수술을 비교한 외국 연구 결과들을 보면 복강경 위암 수술이 수술 중 출혈량이 적으며, 수술 후 통증이 덜하고, 장운동의 회복이 빨라 조기 에 식이 진행이 가능하여 수술 후 재원 일수가 짧다는 장점 과 개복술에 비해 수술시간이 길고 고가의 여러 가지 장비 가 필요하다는 단점을 보고하였다.(8-15) 본 교실의 연구에 서는 복강경 위암 수술이 수술 시간은 길었으나 제거된 림 프절 수와 합병증 발생에서 개복술과 비교하여 차이가 없 으면서 창상의 크기가 작고, 추가 진통제 투여가 적고, 수술
후 알부민 감소가 적었으며, 백혈구 증가가 작았고, 재원일 수가 짧은 장점을 나타내었다.(17)
일반적으로 외과의의 입장에서 환자의 비만은 수술 중 출혈을 많게 하며, 수술시간이 연장되고, 수술 후 합병증 발 생도 증가하는 것으로 인식되어 왔다. 특히 위암수술의 경 우 수술의 근치성를 고려할 때 림프절 절제가 매우 중요하 다. 복강내 과도한 지방조직은 림프절 절제시 많은 기술적 인 어려움을 야기하며 출혈을 증가시키며 이로 인해 수술 시간이 연장된다. 그러나 현재까지 위절제술과 비만도에 관한 연구는 대부분 개복수술에 국한된 것이었고 복강경 위절제술과 비만도에 관한 연구는 미비한 상태이다.
일본에서 시행된 개복 위암수술 연구들에서는 환자의 비 만이 광범위 림프절 절제술과 예후에 영향을 미친다고 보 고하고 있다.(22-24) Inagawa 등에 따르면 BMI 25 이상의 과 체중군에서 수술 후 합병증(Leakage, abscess, postoperative bleeding) 발생률이 22.2%로 BMI 20 미만과 20∼25인 군의 3.3%와 5.6%와 비교하여 현저히 높은 것으로 나타났다.
Dhar 등의 연구에서는 T2/T3환자를 대상으로 분석했을 때 과체중군에서 정상체중군보다 무병 생존율(recurrence- free survival)이 유의하게 짧은 것으로 나타났다(50 vs. 69 months, P=0.0297). 그러나 일부 다른 연구들에서는 비만이 위암수술 에 크게 영향을 미치지 않는다고 보고하였다.(25-27) Noshiro 등(28)은 복강경 보조하 위아전절제술을 시행한 조기위암 환자에서 BMI 24.2을 기준으로 후향적으로 연구 하였으며. 수술시간은 정상체중군의 317±58분과 과체중군 의 370±61분으로 과체중군에서 수술시간이 유의하게 길며 (P=0.015), 가스 배출시기도 정상체중군의 2.6±1.0일에 비 해 과체중군에서는 3.5±1.0일로 의미 있게 지연되는 것으 로 보고하였다(P=0.007). 반면에 본원에서 시행한 연구 결 과는 정상체중군과 과체중군에서 수술시간과 가스 배출시 기가 통계적으로 유의한 차이를 보이지 않았다. 그러나 비 만도와 성별에 따른 수술시간을 살펴보면 남자 과체중군에 서 가장 수술시간이 길었고 여자 정상체중군과 비교하면 약 40분의 수술시간이 더 걸리는 것으로 나타났으며 이는 통계적으로 유의하였다. Noshiro 등의 발표와 달리 본 연구 에서는 정상체중군과 과체중군에서 수술시간의 차이를 보 이지 않았는데, 이는 과체중군에서 Noshiro 등의 남녀 비 1 8:1과 비교하여 본 연구에서는 29:23으로 여성의 비율이 상대적으로 월등히 많았으며 여성에서는 정상체중군과 과 체중군의 수술시간이 차이가 없었던 점이 이유가 될 수 있 을 것이다. 이와 같은 결과에 대한 주요한 원인은 성별에 따른 비만의 양상 차이라고 생각된다. 즉 남자는 내장 비만 이 흔한 반면에 여자는 주로 복벽 비만이 흔하기 때문이다.
저자들의 경험에 의하면 과체중 환자에서 복강경 보조하 위아전절제술을 시행하는 데에는 많은 기술적인 어려움이 있다. 그 원인은 잘 발달된 대망(omentum)으로 인하여 절제 범위와 거리가 멀고, 충분한 시야가 확보되지 않는다는 점 Table 3. Postoperative complications
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Normal High
BMI* BMI P value
(n=52) (n=45)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total (%) 8 (15.4%) 3 (6.7%) 0.2132
Duodenal stump leakage 1 0
Bleeding 3 2
Anastomotic site 2 1
Intraabdominal 2 1
Wound infection 1 0
Wound seroma 0 1
Intraabdominal abscess 1 0
Dumping syndrome 1 0
Pleural effusion 1 0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*BMI = body mass index.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 과 림프절 절제 시 과도한 지방축적으로 수술시간이 연장
되며 출혈이 많아지기 때문이다. 뿐만 아니라 과체중 남자 환자의 경우 여자 환자에 비해 상복부 기복강 형성에 있어 서 더 제한이 있을 것으로 생각된다.(29,30)
우리나라에서도 비만 인구가 점차 증가함에 따라 위암 환자에서도 비만은 수술을 비롯한 치료계획을 세우고 합병 증을 예방하는데 있어서 중요하게 고려해야 할 것이다.
결 론
조기위암 환자에서 시행될 수 있는 복강경 보조하 위아 전절제술에 있어서 환자의 비만도는 성별에 따라 수술시간 에 영향을 미치며 특히 과체중의 남자 환자에서 가장 많은 수술시간이 소요되므로 이러한 결과는 처음 본 시술을 시 작하는 이들에게 많은 도움이 되리라 생각한다.
REFERENCES
1) McIntyre RC Jr, Zoeter MA, Weil KC, Cohen MM. A com- parison of outcome and cost of open vs. laparoscopic cholecys- tectomy. J Laparoendosc Surg 1992;2:143-8.
2) Peters JH, Ellison EC, Innes JT, Liss JL, Nichols KE, Lomano JM, et al. Safety and efficacy of laparoscopic cholecystectomy.
A prospective analysis of 100 initial patients. Ann Surg 1991;
213:3-12.
3) Asao T, Hosouchi Y, Nakabayashi T, Haga N, Mochiki E, Kuwano H. Laparoscopically assisted total or distal gastrec- tomy with lymph node dissection for early gastric cancer. Br J Surg 2001;88:128-32.
4) Yamashita Y, Maekawa T, Sakai T, Shirakusa T. Transgastros- tomal endoscopic surgery for early gastric carcinoma and sub- mucosal tumor. Surg Endosc 1999;13:361-4.
5) Ohgami M, Otani Y, Kumai K, Kubota T, Kim YI, Kitajima M. Curative laparoscopic surgery for early gastric cancer: five years experience. World J Surg 1999:23:187-92.
6) Ohta J, Kodama I, Yamasaki K, Iauchi YY, Takeda J, Shirouau K. Efficacy of transgastrostomal endoscopic surgery (TGES) for early gastric cancer. Int Surg 1997;82:382-5.
7) Shiraishi N, Adachi Y, Kitano S, Bandoh T, Katsuta T, Mori- moto A. Indication for and outcome of laparoscopy-assisted Billoth Ⅰ gastectomy. Br J Surg 1999;86:541-4.
8) Shimizu S, Uchiyama A, Mizumoto K, Morisaki T, Nakamura K, Shimura H, et al. Laparoscopically assisted distal gastrec- tomy for early gastric cancer: is it superior to open surgery?
Surg Endosc 2000;14:27-31.
9) Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy- assisted Billroth I gastrectomy. Surg Laparosc Endosc 1994;4:
146-8.
10) Nagai Y, Tanimura H, Takifuji K, Kashiwagi H, Yamoto H, Nakatani Y. Laparoscope-assisted Billroth I gastrectomy. Surg
Laparosc Endosc 1995;5:281-7.
11) Adachi Y, Shiraishi N, Shiromizu A, Bandoh T, Amamaki M, Kitano S. Laparoscopy-assisted Billroth I gastrectomy com- pared with conventional open gastrectomy. Arch Surg 2000;
135:806-10.
12) Watson DI, Devitt PG, Game PA. Laparoscopic Billroth II gastrectomy for early gastric cancer. Br J Surg 1995;82:661-2.
13) Adachi Y, Suematsu T, Shiraishi N, Quality of life after laparoscopy-assisted Billroth I gastrectomy. Ann Surg 1999;
229:49-54.
14) Yano H, Monden T, Kinuta M, Nakano Y, Tono T, Matsui S, et al. The usefulness of laparoscopy-assisted distal gastrec- tomy in comparison with that of open distal gastrectomy for early gastric cancer. Gastric Cancer 2001;4:93-7.
15) Migoh S, Hasuda K, Nakashima K, Anai H. The benefit of laparoscopy-assisted distal gastrectomy compared with conven- tional open distal gastrectomy: a case-matched control study.
Hepatogastroenterology 2003;50:2251-4.
16) Abdel-Moneim RI. The hazards of surgery in the obese. Int Surg 1985;70:101-3.
17) Kim MC, Lee SG, Jung IK, Jung GJ, Kim HH. Comparison of laparoscopy-assisted by conventional open distal gastrec- tomy and extraperigastric lymph node dissection in early gastric cancer. J Korean Surg Soc 2005;68:24-9.
18) Bae MK, Lee WK, Song CH, Lee KM, Jung SP. The factors associated with body mass index of adults. J Korean Acad Fam Med 1999;20:906-16.
19) Ko SS, Kim SK, Kim SI, Park BW, Lee KS. Body mass index as a risk and prognostic factor of breast cancer. J Korean Surg Soc 2002;63:449-57.
20) World health organization western pacific region. The asia- pacific perspective; redefing obesity and its treatment. 2000.
21) Lee TM, Kwon Y, Kim MC, Jung GJ, Kim HH. Operative outcome of laparoscopy-assisted gastrectomy with lymph node dissection in 117 consecutive patients with gastric cancer: A single-center experience. J Korean Surg Soc 2004;67:106-11.
22) Inagawa S, Adachi S, Oda T, Kawamoto T, Koike N, Fukao K. Effect of the fat volume on postoperative complications and survival rate after D2 dissection for gastric cancer. Gastric cancer 2000;3:141-4.
23) Dhar DK, Kubota H, Tachibana M, Kotoh T, Tabara H, Masunaga R, et al. Body mass index determines the success of lymph node dissection and predicts the outcomes of gastric carcinoma patients. Oncology 2000;59:18-23.
24) Moriwaki Y, Kunisaki C, Kobayashi S, Harada H, Imai S, Kasaoka C. Does body mass index (BMI) influence morbidity and long-term survival in gastric cancer patients after gastrec- tomy? Hapato-Gastroenterology 2003;5:284-8.
25) Park CM, Kim MC, Kim KH, Kim JM, Choi HJ, Kim YH, et al. Body mass index and outcome of gastrectomy with D2 lymphadenectomy. J Korean Surg Soc 2004;67:31-5.
26) Grestschel S, Christoph F, Bembenek A, Estevez-Schwarz L,
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Schneider U, Schlag PM. Body mass index does not affect
systematic D2 lymph node dissection and postoperative mor- bidity in gastric cancer patients. Annal of Surgical Oncology 2003;10:363-8.
27) Kodera Y, Ito S, Yamamura Y, Mochizuki Y, Fujiwara M, Hibi K, et al. Obesity and outcome of distal gastrectomy with D2 lymphadenectomy for carcinoma. Hepatogastrenterology 2004;51:1225-8.
28) Noshiro H, Shimizu S, Nagai E, Ohuchida K, Tanaka M.
Laparoscopy-assisted distal gastrectomy for early gastric cancer: Is it beneficial for patients of heavier weight? Ann Surg 2003;238:680-5.
29) Eltabbakh GH, Piver MS, Hempling RE, Recio FO. Laparo- scopic surgery in obese women. Obstet Gyneco 1999;94:704-8.
30) Eltabbakh GH, Shamonki MI, Moody JM, Garafano LL. Hys- terectomy for obese women with endometrial cancer: laparo- scopy or laparotomy? Gynecol Oncol 2000;78:329-35.