213 CASE REPORT
DOI 10.4070 / kcj.2009.39.5.213
Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright ⓒ 2009 The Korean Society of Cardiology
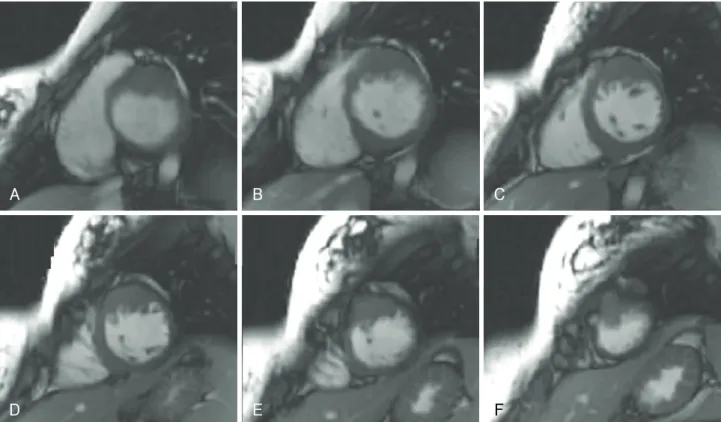
An Unusual Type of Hypertrophic Cardiomyopathy
Hye-Sun Seo, MD
1, Dong Hun Kim, MD
2, Eun Jung Kim, MD
1, Hee Yong Yoo, MD
1, Chul Kim, MD
1, Chan Hyun Lee, MD
1, Bo Yeon Kim, MD
1, Chul Ho Chung, MD
1, Jon Suh, MD
1, Yoon Haeng Cho, MD
1and Nae-Hee Lee, MD
11