J Korean Soc Transplant
2008;22:66-69 □
원 저□
66
책임저자:권오정, 서울시 성동구 행당동 17번지 한양대학교병원 외과, 133-792 Tel: 02-2290-8454, Fax: 02-2281-0224 E-mail: ojkwon@hanyang.ac.kr
고령의 공여자로부터의 신장 이식의 결과
한양대학교 의과대학 외과학교실, 1내과학교실
박 필 경ㆍ권 오 정ㆍ강 종 명1
The Impact of Elderly Donor in Renal Trans- plantation
Pil Kyung Park, M.D., Oh Jung Kwon, M.D. and Chong Myung Kang, M.D.
1Departments of Surgery and 1Internal Medicine, College of Medicine, Hanyang University, Seoul, Korea
Purpose: Kidney transplantation from elderly donors is
controversial because of decline of received renal function and increased risk of perioperative complication. Methods:We retrospectively reviewed the records of the 676 patients from 1985 to 2006 in our center. 42 (6.2%) donors were
≥60 years old, and constitue the group 1, and 634 donors (93.8%) were <60 years old (group 2). We analysis graft survival, preoperative and postoperative creatinine, creatinine clearance, acute rejection rate, infection rate, delayed graft fucntion rate, HLA matching between groups. Results: The average donor age in group 1 is 62.8 yr (60∼73) and 39.3 yr (16∼59) in group 2. Graft survival rate at 1, 5 and 10 years were 92%, 71%, 56% in group 1 vs 92%, 77%, 62%
in group 2 (P=0.0831). There was no difference of graft survival between groups. In preoperative serum creatinine or postoperative days 3, 30 creatinine there was not difference between groups. Infection rate was 9.5% (4 patients) in group 1 vs. 7.3% (46 patients) in group 2. Acute rejection rate was 28.6% (12 patients) vs. 30.9% (196 patients).
Delayed graft function (DGF) rate was 7.1% (3 patients) vs.
9.0% (57 patients). HLA-AB matching was 1.86 vs. 1.78 and HLA-DR matching was 1.12 vs. 1.06. All were not significantly different between groups. But the elderly donor group has a lower creatinine clearance at postoperative 3, 30 days (P=0.0422, 0.0231). Conclusion: The short and long-term survival of kidney transplantation from elderly donors (≥60) are similar to younger donors (<60). We suggest that use of elderly donors may help to expand the donor pool in kidney transplantation. (J Korean Soc Trans-
plant 2008;22:66-69)
Key Words: Kidney transplantation, Elderly donor, Graft sur-
vival rate중심 단어: 신장이식, 고령의 공여자, 이식신 생존률
서 론
당뇨, 고혈압, 노령인구의 증가에 따라 말기 신부전 환자 는 계속해서 증가하고 있다(1). 이런 말기 신부전 환자들에 게 신장 이식은 삶의 질을 높이고 생존률의 향상을 가져다 주는 가장 좋은 치료 방법으로 인정되고 있으며 현재 많은 병원에서 널리 행해지고 있다(2). 그러나 신장 이식이 최적 의 치료 방법임에도 불구하고 신장의 공여자와 수혜자 간 의 수적 차이가 점점 커짐에 따라 신장 이식을 위한 대기시 간이 길어지고 있는 실정이다. 이러한 수요와 공급의 불일 치로 인해 과거에는 금기로 되었던 확장된 기준의 공여자 (expanded criteria donor), 즉 비혈연 관계의 생체 신장 이식, 고령의 공여자로부터의 신장 이식, 잘 관리 되어진 고혈압 환자의 신이식 등도 근래에 들어 많이 이루어지고 있다. 그 러나 고령의 공여자로부터의 신장 이식은 이식신 기능의 감소, 수술 전후의 합병증 증가, 장기 생존률의 저하, 재이 식 가능성 등으로 인해 아직도 논쟁의 여지가 있다. 그래서 본원 이식센터에서는 공여자 확장에 기여할 수 있는 고령 의 공여자로부터의 신장 이식의 결과를 후향적으로 분석하 였다.
방 법
본원 이식센터에서 1985년부터 2006년까지 시행한 676건 의 신장이식을 후향적으로 분석하였다. 60세 이상의 공여 자 군과 60세 미만의 공여자 군으로 나누었으며, 60세 이상 은 42명(6.2%), 60세 미만은 634명(93.8%)이었다. 각 군의 이식신 생존율, 수술 전후 혈청 크레아티닌 수치, 크레아티 닌 청소율, 급성 거부 반응, 감염, DGF (delayed graft function), 조직 적합 항원 일치수를 비교하였다. 1987년까지 의 수혜자들에게는 imuran과 steroid가 사용되었고 그 이후 에는 cyclosporine 혹은 tacrolimus, immuran이나 mycopheno- late mefetil, steroid의 삼중 면역억제제를 시행 하였다. 급성
박필경 외
:고령의 공여자로부터의 신장 이식의 결과 67
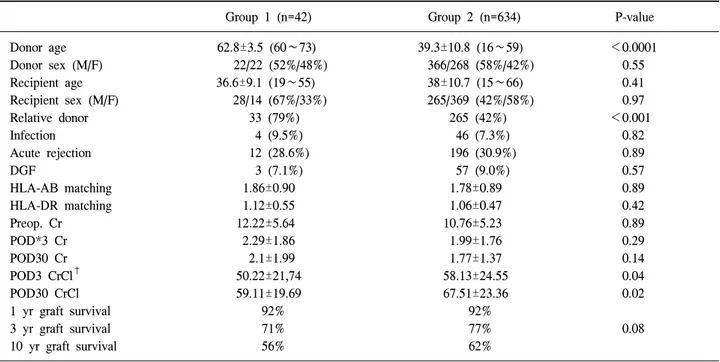
Table 1. Chracteristics of elderly group donor and younger donor group
Group 1 (n=42) Group 2 (n=634) P-value
Donor age 62.8±3.5 (60∼73) 39.3±10.8 (16∼59) <0.0001
Donor sex (M/F) 22/22 (52%/48%) 366/268 (58%/42%) 0.55
Recipient age 36.6±9.1 (19∼55) 38±10.7 (15∼66) 0.41
Recipient sex (M/F) 28/14 (67%/33%) 265/369 (42%/58%) 0.97
Relative donor 33 (79%) 265 (42%) <0.001
Infection 4 (9.5%) 46 (7.3%) 0.82
Acute rejection 12 (28.6%) 196 (30.9%) 0.89
DGF 3 (7.1%) 57 (9.0%) 0.57
HLA-AB matching 1.86±0.90 1.78±0.89 0.89
HLA-DR matching 1.12±0.55 1.06±0.47 0.42
Preop. Cr 12.22±5.64 10.76±5.23 0.89
POD*3 Cr 2.29±1.86 1.99±1.76 0.29
POD30 Cr 2.1±1.99 1.77±1.37 0.14
POD3 CrCl
†50.22±21,74 58.13±24.55 0.04
POD30 CrCl 59.11±19.69 67.51±23.36 0.02
1 yr graft survival 92% 92%
3 yr graft survival 71% 77% 0.08
10 yr graft survival 56% 62%
*POD = postoperative day;
†CrCl = creatinine clearance.
Fig. 1. Comparision of graft survival between two groups.
거부 반응은 임상적으로 발열, 수술 부위 압통, 부종, 소변 량 감소, 몸무게 증가 등의 증상과 혈청 크레아티닌 상승, 도플러 초음파를 이용한 저항지수(resistance index), 이식신 조직 검사 등을 이용해 진단하였으며 급성 거부 반응이 일 어난 경우 치료로는 steroid 강화 요법과 항림프구 항체요법 을 시행하였다. 통계 처리는 SPSS 12.0을 사용하였고 이식 장기 생존율은 Kaplan-Meier 방법을 이용하여 비교 분석하 였으며, log-rank 검사법을 이용하여 P<0.05인 경우 통계적 으로 의미가 있다고 판정하였다.
결 과
1985년부터 2006년까지 본원 이식센터에서 신이식을 받 은 676명의 환자 중 60세 이상의 공여자로부터 받은 환자 42명을 1군, 60세 미만의 공여자로부터 받은 환자 634명으 로 2군으로 하고 비교하였다(Table 1). 공여자의 평균 나이 는 1군은 62.8세(60∼73세), 2군은 39.3세(16∼59세)였으며, 수혜자의 평균 나이는 1군은 36.6세(19∼55), 2군은 38.0세 (15∼66세)로 차이가 없었다(P=0.41). 공여자와 수혜자의 성 비 또한 두 군에 유의한 차이가 없었다(P=0.55, 0.41). 혈연 관계로부터 받은 경우는 고령의 공여자가 부모에게서 받은 경우가 많은 1군에서 33명(79%), 2군에서는 265명(42%)로 1군에서 유의하게 많았다(P<0.001). 요로 감염, 상기도 감 염, 창상 감염, 편도선염 등 수술 후 감염율은 1군에서 4명 (9.6%), 2군에서 46명(7.3%), 급성 거부 반응 비율은 1군에 서 12명(28.6%), 2군에서 196 (30.9%)으로 차이가 없었다
(P=0.83, 0.89). DGF (delayed graft function) 비율도 1군에서 3명(7.1%), 2군에서 57명(9.0%)로 차이가 없었으며(P=0.57), 조직 적합 항원 일치수는 HLA-AB 항원 일치수는 1군과 2 군에서 각각 1.86과 1.78, HLA-DR 항원 일치수는 1.12와 1.06으로 모두 의미 있는 차이는 없었다(P=0.89, 0.43). 수술 전 혈청 크레아티닌은 1군에서 12.22, 2군에서 10.76으로 차 이가 없었으며(P=0.89), 수술 후 3일째, 30일째 혈청 크레아 티닌 또한 각각 2.29와 1.99, 2.1과 1.77로 2군에서 다소 낮기 는 하나 통계적인 차이는 없었다(P=0.29, 0.14). 그러나 수술 후 3일째, 30일째 크레아티닌 청소율은 60세 미만의 공여자 로부터 받은 군에서 통계적으로 유의하게 높았다(P=0.04,
68 대한이식학회지
:제 22 권 제 1 호 2008
0.02). 이식신의 생존율은 1년, 3년, 10년 생존율을 비교하였 다. 1군에서는 1년, 3년, 10년 이식신 생존율이 92%, 71%, 56%, 2군에서는 92%, 77%, 62%로 두 그룹 간의 유의한 차 이가 없음을 볼 수 있었다(P=0.08)(Fig. 1).
고 찰
만성 신부전 환자에서 신장 이식은 투석 요법에 비해 생 활의 질적 우수성, 합병증 감소, 장기 생존율을 높이는 등 최적의 치료로 인정되고 있지만 현재 공여자 수가 부족한 실정이다. 당뇨, 고혈압, 노령 인구의 증가에 따라 만성 신 부전 환자 수는 늘어나고 이 환자들을 위한 사체 공여자 또는 혈연간 공여자의 수적 차이가 커 공여자 수를 늘이기 위한 많은 노력이 이루어지고 있다. 사체이식, 고위험군 공 여자의 이식, 확장된 기준의 공여자(ECD)의 이식, 혈액형이 불일치하는 공여자의 이식, 본원에서 시행하고 있는 교환 이식 프로그램 등이 모두 공여자 증가를 목적으로 시행 되 고 있는 방법들이다. 특히 고령화 사회에 접어 듦에 따라 고령의 공여자로부터의 이식이 여러 병원에서 점차 시행되 고 있다(3). 그러나 일반적으로 20대 이후에 신기능은 점차 적으로 감소되는 것으로 감소되는 것으로 되어 있어 고령 의 공여자로부터의 신장 이식은 현재까지도 논의의 대상이 되고 있고(4,5), 불충분한 신원 질량(nephron mass)을 가진 고령의 공여자로부터의 이식은 초기 과여과(hyperfiltration), 이식신 손상, 이식신 생존율을 낮춘다고 보고되고 있다(6, 7) 고령의 공여자를 이용한 사체 신장 이식에 대한 DGF, 거부 반응, 이식신 생존율 등에 대해서는 Teraski 등(8)이 발 표했는데, 이러한 이식의 결과가 좋지 않음에도 불구하고 현재 생체 신장 이식의 경우는 고령의 공여자로부터의 이 식이 여러 센터에서 시도되고 있고 결과가 발표되고 있다.
Kerr 등(9)은 55세 이상의 공여자로부터의 신장 이식이 55 세 미만의 공여자와 비교해서 이식신 생존에 차이가 없다 고 발표했고, Invanovski와 Hydjiyannakis와 Tanaka 등(10-12) 은 60세 이상의 공여자로부터의 생체 신장 이식은 통계적 으로 생존율의 차이가 없다고 발표했다. 고령의 공여자로 부터의 신장 이식은 일반적인 수술에서와 마찬가지로 수술 후 생기는 합병증의 유병율이 증가된다는 것이다(13,14).
Edwards 등이 발표한 자료에 따르면 55세 이상의 공여자들 에게서 수술후 합병증이 높게 나타났다고 보고하고 있다 (15). 하지만 대부분의 합병증은 경미하고 자가 회복되었으 며, Invanovski와 Kumar 등(10,16)은 고령의 공여자군에서 수술 전후 합병증의 증가율이 의미있게 높지 않았다고 발 표했다.
본 연구에서는 수술 후 3일째, 30일째 크레아티닌 청소율 은 60세 이상의 군에서 낮게 나왔지만 수술 후 생길 수 있는 중요한 합병증인 감염, 급성 거부 반응, DGF 등이 두 군에 서 통계적인 차이가 없었다. 특히 조 등(17)이 발표한 이식
신의 장기 생존율을 예측하는 중요한 요소인 이식 후 1개월 의 혈청 크레아티닌 수치는 두 군에서 차이가 없었으며 실 제 이식신의 1년, 3년, 10년 생존율 또한 차이가 없었다.
결 론
고령의 공여자로부터의 신장 이식은 앞에서 설명한 여러 가지 이유로 인해 과거에는 금기시 되었지만 본원에서 시 행한 신장 이식의 결과를 분석한 결과 크레아티닌 청소율 이 고령의 공여자군에서 의미있게 낮았음에도 불구하고 실 제 이식신의 단기 및 장기 생존율은 통계적으로 차이가 없 어 고령의 공여자가 공여자 확장에 도움을 줄 수 있을 것이 라 생각한다.