대한소화기학회지 2005;46:1-3
□ IMAGE OF THE MONTH □
증례: 42세 남자가 내원 9개월 전부터 시작되고 점차 악화 되는 식후 상복부 통증과 상복부 포만감 및 식욕부진을 주 소로 내원했다. 과거력, 개인력, 가족력은 특이소견이 없었 으며 최근 과로로 5 kg 정도의 체중 감소가 있었다. 체중이 42 kg, 신장이 175 cm로 매우 마른 체형이었다. 신체 활력징 후는 정상이었으며, 신체검사에서 경도의 복부 팽만과 상복 부 압통이 있었다. 말초혈액검사는 백혈구 12,600/mm3, 혈색 소 13.6 g/dL, 혈소판 458,000/mm3이었고, 총 단백 6.7 g/dL, 알부민 4.0 g/dL, AST 16 IU/L, ALT 29 IU/L, 총 빌리루빈 0.5 mg/dL이었으며 갑상선기능 검사도 정상이었다.
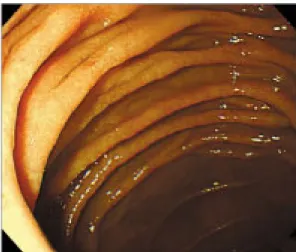
상부위장관 내시경은 십이지장 구부 및 2부가 심하게 확 장되었으나 그 외 특이소견은 없었다(Fig. 1). 복부 CT에서 복강 내에 지방이 거의 관찰되지 않았고, 십이지장 구부 및 2부의 확장과 함께 대동맥과 상장간막동맥 간격이 매우 좁
상장간막동맥증후군
한양대학교 의과대학 내과학교실
이 항 락
Superior Mesenteric Artery Syndrome
Hang Lak Lee, M.D.Department of Internal Medicine, Hanyang University Hospital, Seoul, Korea
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Correspondence to: Hang Lak Lee, M.D.
Department of Internal Medicine, Hanyang University Hospital 17 Haengdang-dong, Seongdong-gu, Seoul 133-070, Korea Tel: +82-2-2290-8354, Fax: +82-2-2298-9183
E-mail: [email protected]
Fig. 1. Gastroscopic finding. Duodenal 2nd portion is markedly dilated without definite obstructive lesion.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
연락처: 이항락, 133-070, 서울시 성동구 행당동 산 17번지 한양대학교병원 소화기내과
Tel: (02) 2290-8354, Fax: (02) 2298-9183 E-mail: [email protected]
Fig. 2. (A) Abdominal CT find- ing. It shows a compression of the duodenum between the aorta (white arrow) and superior mesen- teric artery (black arrow). In ad- dition, small amount of abdominal fat is noted. (B) Abdominal CT finding of sagittal view. It shows a narrowed aortomesenteric angle more clearly (arrow).
2 대한소화기학회지: 제46권 제1호, 2005
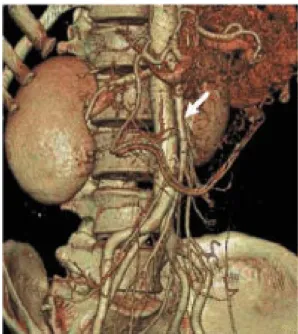
았으며 십이지장 3부의 압박이 보였다(Fig. 2A). 또한 상장 간막동맥과 대동맥의 각도가 좁았다(Fig. 2B). 3차원 CT 혈 관촬영에서 상장간막동맥이 복부대동맥에서 다소 수직으로 주행되어 보였다(Fig. 3). 소장조영술에서 십이지장 3부가 수직으로 압박되었고 또한 십이지장 2부 및 3부가 확장되어 있었으며 3부의 부분 폐색을 의심하였다(Fig. 4). 진단은?
진단: 상장간막동맥증후군
상장간막동맥증후군은 1861년 Rokitansky에 의해 처음으 로 소개되었으며 arteriomesenteric duodenal compression, vas- cular compression of the duodenum, Wilkie 증후군으로도 불 린다.1,2 해부학에서 상장간막동맥은 1번 요추위치의 복부대 동맥에서 기시해 십이지장을 가로지르며 이 상장간막동맥 에 의해 십이지장 3부가 눌려서 발생하는 질환이다.3 이 증 후군은 대동맥과 상장간막동맥 각도가 6-16도까지 감소하면 발생할 수 있으며 대부분 심한 체중 감소와 연관이 있다. 또 한 신체 cast, 선천적인 해부 이상, 복부 수술 합병증, 복부 대동맥류, 갑상선 항진증 및 임신도 가능한 원인이다.4-6 정 상인에서 상장간동맥 기시부의 지방조직과 림프조직 등이 십이지장을 압박하는 것을 보호하지만 급속하게 체중이 감 소하는 경우 상장간막동맥 주변에 지방조직이 감소하여 십 이지장 압박의 원인이 된다.2 임상증상은 급성 또는 만성으 로 발생할 수 있으며 급성인 경우 오심, 구토, 복통, 복부팽 만 등의 소장 폐색 증상이 나타나며 만성인 경우 반복 구토 를 동반한 복통, 포만감, 식욕부진 등의 증상이 나타난다.
방사선소견은 단순복부촬영에서 위 확장이 보이며 소장조
영술에서 십이지장의 확장 및 십이지장 3부에서 수직 방향 의 선상 외부압박이 보인다. 십이지장조영술과 동시에 상장 간막동맥조영술을 시행하는 경우 좀 더 좋은 영상을 얻을 수 있으며 3차원 복부 CT 혈관촬영도 십이지장 확장과 상 장간막동맥과 복부대동맥의 접근을 쉽게 알 수 있어 진단에 좋은 정보를 준다.7
치료는 보전 치료가 우선이며 드물게 수술을 고려할 수 있다. 보전 치료는 전비경구 영양이나 비공장관을 통한 영 양 공급에 따른 체중 증량이 중요하며 자세 변화 등도 도움 이 된다. 보전 치료가 실패한 경우 수술 치료도 고려할 수 있다.
참고문헌
1. Sostek M, Fine SN, Harris TL. Duodenal obstruction by ab- dominal aortic aneurysm. Am J Med 1993;94:220-221.
2. Hines JR, Gore RM, Ballantyne GH. Superior mesenteric ar- tery syndrome. Diagnostic criteria and therapeutic approaches.
Am J Surg 1984;148:630-632.
3. Komai H, Naito Y, Fujiwara K. Superior mesenteric artery syndrome as a result of enlarged abdominal aortic aneurysm.
J Vasc Surg 1999;29:1162-1163.
4. Edwards KC, Katzen BT. Superior mesenteric artery syn- drome due to large dissecting abdominal aortic aneurysm.
Am J Gastroenterol 1984;79:72-74.
5. McClenathan JH, Wood BP. Radiological case of the month.
Hyperthyroidism as a cause of superior mesenteric artery syndrome. Am J Dis Child 1988;142:685-686.
Fig. 3. Three dimensional abdominal CT angiographic finding. It shows a relative vertical axis of superior mesenteric artery (white arrow) from abdominal aorta.
Fig. 4. Duodenographic finding. It shows a distended 2nd and 3rd portion of the duodenum and vertical extrinsic compression of the duodenal 3rd portion.
이항락. 상장간막동맥증후군 3
6. Iko BO, Monu JU, Orhue A, Sarkar SK. The superior me- senteric artery syndrome in pregnancy: a case resulting in recurrent pregnancy loss. Eur J Obstet Gynecol Reprod Biol 1986;21:233-236.
7. Shetty AK, Schmidt-Sommerfeld E, Haymon ML, Udall JN Jr. Radiological case of the month. Superior mesenteric artery syndrome. Arch Pediatr Adolesc Med 1999;153:303-304.