우리나라에서는 전통적으로 혼합 성분의 한약을 복용하는 경우가 많은데 드물게 그 부작용으로 기침, 호흡곤란 등을 호 소하는 환자들이 있다. 기존의 여러 문헌에서 한약 복용 이후 에 생긴 부작용으로 간 독성에 대해서는 언급이 많았으며, 최 근에는 폐 독성에 관심이 쏠리고 있다. 하지만, 국내에서는 아 직 한약 유발 폐질환에 대한 영상학적인 연구는 없는 것으로 알고 있다. 이에 저자들은 혼합 성분의 한약 복용으로 인한 미 만성침윤성폐질환의 고해상 CT 소견과 함께 조직병리학적 소 견을 알아보고자 하였다.
대상과 방법
2005년 10월부터 2007년 6월까지, 혼합 성분의 한약 복용 이후 조직검사에서 미만성 침윤성 폐질환으로 진단된 7명의
환자와 조직검사는 시행하지 않았지만, 임상적으로 진단한 1 명을 포함해 총 8명을 대상으로 하였다. 여자가 6명, 남자가 2 명이었으며 연령은 31~81세(평균 51.4세)였다. 주로 호소하 는 증상은 기침과 호흡곤란으로, 한약 복용 이후에 기침, 호흡 곤란이 새로 발생한 환자가 4명이었고 기존의 기침을 완화하 기 위해 한약을 복용하였다가 이후 기침이 더 심해지면서 호흡 곤란이 발생한 환자가 4명이었다. 환자들은 증상이 발생하거 나 악화한 시점으로부터 1~1.5개월 전에, 3~20일 동안 복합 성분의 한약을 복용한 과거력이 있었다. 한약을 복용한 이유로 는 기침 조절을 위해서가 3명이었고, 건강 증진을 위한 경우가 3명, 체중 감량을 위한 경우가 2명이었다.
모든 환자는 흉부 X선촬영, 흉부 고해상 CT, 폐기능 검사를 시행하였다. 사용된 CT 기종은 Siemens Somatom Volume Zoom (Siemens medical system, Forchheim, Germany) 이었으며 2 mm의 절편 두께로 흉곽입구에서 상복부까지 영상 을 얻었다. 6명의 환자에서 과거 흉부 X선사진은 정상이었으 며 2명은 과거 사진이 없었다. 흉부 X선촬영 사진과 고해상 CT의 판독은 2명의 영상의학과 전문의가 후향적으로 분석하
혼합성분의 한약복용 후 발생된 미만성침윤성폐질환:
고해상CT 및 조직병리학적 소견
1김 태 규∙김 정 숙2∙신 은 아3
목적: 혼합성분의 한약 복용 후 발생한 미만성침윤성폐질환의 고해상 CT소견 및 병리학적 소견 을 알아보고자 하였다.
대상과 방법:혼합 성분의 한약을 복용한 이후 기침, 호흡곤란이 발생하였거나 기존의 기침, 호 흡곤란이 더 심해진 8명(여자 6명, 남자 2명, 31~81세)을 대상으로 하였다. 모든 환자에게 흉 부 X선촬영 및 흉부 고해상 CT를 시행하였고, 7명에서는 방사선투시 하 대침절제생검 및 경기 관지폐생검으로 폐병변 부위의 병리 조직을 얻었다.
결과:가장 흔한 고해상CT 소견으로는 양측성 미만성 간유리 음영(n=7)이었고, 다음으로 기 관지주위 경화(n=5), 소엽간 중격 비후(n=2)였다. 병변은 폐 상부보다는 폐 하부, 폐 주변부 보다는 폐 중심부에 주로 분포하였다. 조직검사를 시행한 7예의 병리학적 소견으로는 비특이적 간질성폐렴이 3명, 폐쇄성세기관지기질화폐렴이 2명, 그리고 과민성폐렴, 호산구성폐렴이 각각 1명이었다. 조직병리학적 소견과 관계없이 모든 환자는 스테로이드 치료 이후 임상적, 영상학 적으로 호전되었다.
결론: 혼합 성분의 한약 복용 후 발생한 미만성침윤성폐질환의 고해상CT 소견은 주로 양측성 미만성 간유리 음영, 기관지주위 경화로 나타났으며 폐 하부를 주로 침범하는 경향이 있었다.
병리학적 소견으로는 비특이적간질성폐렴, 폐쇄성세기관지기질화폐렴, 과민성폐렴, 호산구성 폐렴 등 다양하였다.
1인제대학교 상계백병원 영상의학과
2이화여자대학교 목동병원 건진의학과
3인제대학교 상계백병원 진단병리과
이 논문은 2010년 8월 30일 접수하여 2010년 10월 9일에 채택되었음.
였으며, 고해상 CT에서 주된 병변의 소견과 그 병변의 분포 영역에 대해 알아보았다.
8명의 환자 중 5명은 16게이지의 대침으로 방사선투시유도 하 경피적폐생검술을, 2명은 경기관지폐생검술을 시행하여 병 리 조직을 얻어 진단하였고, 나머지 한 명은 임상적, 영상학적 소견을 바탕으로 진단하였다.
모든 환자는 한약 복용을 중단하였고, 10일~4개월(평균 43 일) 동안의 스테로이드 치료를 받았다. 치료 후 면담을 시행하 고, 흉부 X선촬영 혹은 흉부 고해상CT를 시행하여 추적관찰 을 하였다.
결 과
가장 흔한 흉부 고해상CT 소견으로는 양측성 미만성 간유리 음영(ground glass opacity)으로 8명 모두에서 보였다. 다음 으로, 기관지주위 경화(peribronchial consolidation)가 나타 난 경우가 5명이었고, 2명에서 소엽간 중격 비후(interlobu- lar septal thickening)를 나타내었다. 8명 중 폐 중심부에 주 로 분포를 한 경우가 6명, 폐 주변부에 주로 분포를 한 경우가 1명이었고 중심부와 주변부에 골고루 분포한 경우가 1명이었 다. 그리고 폐 상부(n=2)보다는 폐 하부(n=6)에 병변이 주
A B
C D
Fig. 1. A 51-year-old man who had taken mixed herbal medicine for general health promotion. After one and half month, dyspnea and cough were developed.
A. Chest PA shows diffuse increased haziness in both lower lung zone.
B. HRCT demonstrates diffuse ground glass opacities in both lower lobes.
C. Fluoroguided cutting needle biopsy specimen demonstates nonspecific interstitial pneumonia pneumonia (H & E staining × 400).
D. On chest PA radiograph after steroid therapy, most of the opacity was cleared and patient’s symptom was improved.
로 존재하였다.
모든 환자는 폐기능 검사에서 제한성 폐질환과 함께 폐쇄성 폐질환의 소견을 나타내었다.
폐 생검을 시행한 7명의 조직병리 소견으로는 비특이적간질 성폐렴(nonspecific interstitial pneumonia)이 3명(Fig.
1), 폐쇄성세기관지기질화폐렴(bronchiolitis obliterans organizing pneumonia)이 2명(Fig. 2), 과민성폐렴 (hypersensitivity pneumonitis)과 호 산 구 성 폐 렴 (eosinophilic pneumonia)이 각각 1명이었다(Fig. 3). 조직 검사를 시행하지 않은 나머지 한 명은 한약 복용 이후에 기침 과 호흡곤란이 발생하였으며, 고해상CT소견에서 양측성 미만
성 기관지주위 경화를 보여 한약으로 인한 폐쇄성세기관지기 질화폐렴 의심 하에 한약 복용을 중단하고 스테로이드 치료를 하여 호전된 증례였다. 조직병리 소견과 관계없이 8명 모두에 서 한약 복용 중단과 스테로이드 치료 이후 임상적, 영상학적 으로 호전되었다(Table 1).
고 찰
한약은 한국, 중국, 일본 등에서 전통적으로 많이 복용해 왔 으며 최근에는 미국, 유럽 등 여러 나라에서 관심이 있는 약제 로 한약 복용으로 인한 폐질환은 1989년 Tsukiyama 등에 의
A B
C D
Fig. 2. A 58-year-old woman who had taken mixed herbal medicine for cough control. After one month, dyspnea and cough were progressed.
A. Chest PA shows bilateral hilar and perihilar consolidation.
B. HRCT shows peribronchial consolidation and ground glass opacities in both upper lobes.
C. Fluoroguided cutting needle biopsy specimen demonstrates bronchiolitis obliterans organizing pneumonia (H & E staining, × 100).
D. Two month after steroid theraphy, chest PA was cleared with improving clinical symptom.
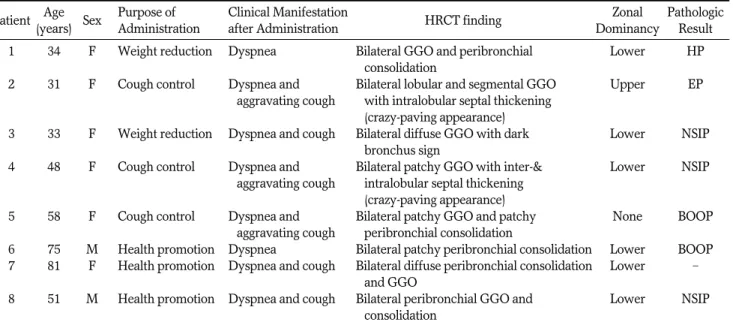
Table 1. Summary of Clinical history, HRCT Finding, and Pathologic Result of Mixed Herbal Medicine Induced DILD in 8 Patients Patient Age
Sex Purpose of Clinical Manifestation
HRCT finding Zonal Pathologic
(years) Administration after Administration Dominancy Result
1 34 F Weight reduction Dyspnea Bilateral GGO and peribronchial Lower HP
consolidation
2 31 F Cough control Dyspnea and Bilateral lobular and segmental GGO Upper EP aggravating cough with intralobular septal thickening
(crazy-paving appearance)
3 33 F Weight reduction Dyspnea and cough Bilateral diffuse GGO with dark Lower NSIP bronchus sign
4 48 F Cough control Dyspnea and Bilateral patchy GGO with inter-& Lower NSIP aggravating cough intralobular septal thickening
(crazy-paving appearance)
5 58 F Cough control Dyspnea and Bilateral patchy GGO and patchy None BOOP
aggravating cough peribronchial consolidation
6 75 M Health promotion Dyspnea Bilateral patchy peribronchial consolidation Lower BOOP 7 81 F Health promotion Dyspnea and cough Bilateral diffuse peribronchial consolidation Lower -
and GGO
8 51 M Health promotion Dyspnea and cough Bilateral peribronchial GGO and Lower NSIP consolidation
Note.─DILD = diffuse infiltrative lung disease, HRCT = High-resolution computed tomography, GGO = ground glass opacity, HP = hypersen sitivity pneumonitis, EP = eosinophilic pneumonia, NSIP = nonspecific interstitial pneumonia, BOOP = bronchiolitis obliterans organizing pneumonia
A
B
Fig. 3. A 31-year-old women who had taken herb medicine for control of coughing. After one month, dyspnea and aggravating cough was developed.
A. HRCT shows subpleural lobular ground glass opacities in both upper lobes.
B. Histologic spacimen demonstrates eosinophilic pneumonia (H & E staining ×400).
해 처음 보고되었다(1).
일반적으로 복용하는 한약은 한 가지 약제 성분으로 구성된 것이 아니라 보통 여러 성분이 혼합되어 있다. Takeshita 등 (2)은 이 복합 한약 성분 중에 어떤 성분이 폐질환을 일으켰는 지 알기 위해 각각의 약제 성분으로 유발 검사를 시행하였다.
한 가지 특정 성분을 투여하였을 때만 체온, 백혈구, C 반응 단백질이 상승하고, 동맥혈 산소분압이 감소하며, 흉부 X선촬 영과 CT에서 미만성 간질성 음영이 증가하는 것을 확인함으로 써 그 특정 성분에 의해 폐질환이 발생하였다는 것을 증명하였 다.
폐질환이 한약에 의해 유발되었다는 것을 증명하는 또 다른 방법으로 림프구 유발 검사가 있다. Shiota 등(3)에 의하면 림 프구 유발 검사에서 양성으로 나오면 그 약제를 원인으로 생각 할 수가 있다. 반면에 Sakamoto 등(4)에 의한 연구에서는 5 명 중 4명에서 림프구 자극 검사를 시행하였으나 모두 음성으 로 나왔으며, 림프구 자극 검사와 관계없이 5명 모두에서 한약 복용의 병력과 복용 후에 발생한 임상증상, 영상학적 검사에서 의 폐침윤, 여러 혈액검사 소견을 종합하여 한약 유발 폐질환 의 진단에 이르렀다. 본 연구에서는 약제 유발 검사, 림프구 자 극 검사는 시행하지 않았지만, 이전의 정상 흉부 X선촬영, 약 제 복용 과거력, 복용 이후 임상 증상의 발생 혹은 악화, 영상 학적인 폐침윤, 폐 조직 병리, 한약 복용 중지와 스테로이드 치 료 후 호전 등의 소견을 종합하여 진단하였다.
기관지 폐포 세척 검사도 시행할 수 있는데, 한약 유발 폐질 환에서도 일반적인 약제에서와 마찬가지로 림프구가 증가하고 CD4/CD8 비가 감소를 하면 진단에 도움을 줄 수 있다(2, 5, 6).
본 연구에서 주된 고해상 CT 소견은 양측성 미만성 간유리 음영과 기관지주위 경화였다. 기존의 문헌에서는 미만성 간유 리 음영과 기관지주위 경화 외에도 소결절, 흉막 삼출, 그리고 성인호흡곤란증후군이 발생한 경우는 견인성 기관지 확장증이 나 폐구조 왜곡 등의 소견을 보고하기도 하였다(3, 4, 7).
기존의 여러 연구에서 조직 검사를 시행하여 병리 소견을 알 아보고자 한 경우가 있었는데 주로 림프구 폐포염, 간질성 폐 렴, 호산구성 폐렴 혹은 기질화 폐렴 등의 결과였다(2, 5, 8- 10). 저자들이 아는 바로는 조직검사에서 폐쇄성세기관지-기 질화폐렴으로 나온 경우는 거의 없는 것으로 알고 있다. Hata 등(11)에 의한 연구에서는 CT에서 폐쇄성세기관지-기질화폐 렴을 시사하는 소견이 보였으나 조직검사는 시행하지 않았다 (11). 본 연구에서는 2명의 병리조직에서 폐포 내 섬유모세포 전(intraalveolar fibroblast plug)을 보이는 폐쇄성세기관 지-기질화폐렴의 소견을 나타내었다.
한약 유발 폐질환이 발생하였을 때는 한약 복용을 중지하는 것이 우선이다. 스테로이드를 사용하지 않아도 증상이 호전된 다는 보고도 있으며(2, 5) 스테로이드 치료가 효과 있다는 보 고도 있다(3, 4, 8, 12). 한편, 폐부종에 의해 폐 기능 부전이 발생하였을 경우는 스테로이드 치료만으로는 불충분하고 기계 호흡(호기말 양압 호흡)을 시행하면 매우 효과적이라는 주장 도 있다(13). Sato 등(14)은 한약 유발 폐질환에 의해 폐 기
능 부전이 발생하여 사망한 예도 보고를 하였다(14). 본 연구 에서는 8명 모두에서 한약 복용을 중단시키고 스테로이드를 사용한 후 임상적, 영상학적 호전을 보였다. 따라서 한약 복용 이후 기침 혹은 호흡곤란이 새로 발생하였거나 더 심해졌을 때 는 한약 유발성 폐질환을 의심하여 약 복용을 즉시 중단시켜야 한다. 이어서 흉부 X선촬영, CT를 시행하여 미만성 침윤성 폐 질환의 소견이 있을 경우 스테로이드 사용을 고려해야 할 것이 다. 반대로 기침 혹은 호흡곤란을 호소하는 환자가 영상학적 혹은 병리학적으로 미만성 침윤성 폐질환의 소견이 있을 때는 한약 복용의 과거력을 조사해 보는 것이 필요하다.
본 연구의 제한점으로 우선 환자의 수가 적었다는 점이다.
두 번째로는 약제 유발 검사나 림프구 자극 검사를 시행하지 않았다는 점이며 세 번째로는 한약은 대부분 복합 성분으로 이 루어져 있는데 그 중 어떤 특정 성분이 폐질환을 유발하였는지 는 알 수 없었다는 점이다.
결론적으로 혼합 성분의 한약 복용으로 유발된 미만성 침윤 성 폐질환의 주된 CT 소견으로는 양측성 미만성 간유리 음영, 기관지주위 폐경화이며 폐 상부보다는 폐 하부에, 폐 주변부보 다는 폐 중심부에 병변이 분포하는 경향이 있다. 또한, 조직병 리학적으로는 비특이적간질성 폐렴, 폐쇄성세기관지-기질화폐 렴, 과민성폐렴, 호산구성폐렴 등을 보일 수 있다.
참 고 문 헌
1. Tsukiyama K, Tasaka Y, Nakajima M, Hino J, Nakahama C, Okimoto N, et al. A case of pneumonitis due to sho-saiko-to. Nihon Kyobu Shikkan Gakkai Zasshi 1989;27:1556-1561
2. Takeshita K, Saisho Y, Kitamura K, Kaburagi N, Funabiki T, Inamura T, et al. Pneumonitis induced by ou-gon (scullcap). Intern Med 2001;40:764-768
3. Shiota Y, Wilson JG, Matsumoto H, Munemasa M, Okamura M, Hiyama J, et al. Adult respiratory distress syndrome induced by a Chinese medicine, Kamisyoyo-san. Intern Med 1996;35:494-496 4. Sakamoto O, Ichikado K, Kohrogi H, Suga M. Clinical and CT
characteristics of Chinese medicine-induced acute respiratory dis- tress syndrome. Respirology 2003;8:344-350
5. Heki U, Fujimura M, Ogawa H, Matsuda T, Kitagawa M.
Pneumonitis caused by saikokeisikankyou-tou, an herbal drug.
Intern Med 1997;36:214-217
6. Akoun GM, Cadranel JL, Milleron BJ, D’Ortho MP, Mayaud CM.
Bronchoalveolar lavage cell data in 19 patients with drug-associat- ed pneumonitis (except amiodarone). Chest 1991;99:98-104 7. Akira M, Ishikawa H, Yamamoto S. Drug-induced pneumonitis:
thin-section CT findings in 60 patients. Radiology 2002;224:852-860 8. Ishizaki T, Sasaki F, Ameshima S, Shiozaki K, Takahashi H, Abe Y, et al. Pneumonitis during interferon and/or herbal drug therapy in patients with chronic active hepatitis. Eur Respir J 1996;9:2691- 2696
9. Kobashi Y, Nakajima M, Niki Y, Matsushima T. A case of acute eosinophilic pneumonia due to Sho-saiko-to. Nihon Kyobu Shikkan Gakkai Zasshi 1997;35:1372-1377
10. Yamawaki I, Katsura H, Taira M, Kadoriku C, Hashimoto I, Chiyotani A, et al. Six patients with pneumonitis related to blended Chinese traditional medicines. Nihon Kyobu Shikkan Gakkai Zasshi 1996;34:1331-1336
11. Hata Y, Uehara H. A case where herbal medicine sho-seiryu-to in- duced interstitial pneumonitis. Nihon Kokyuki Gakkai Zasshi 2005;
43:23-31
12. Yoshida Y. A non-cardiogenic type of pulmonary edema after ad- ministration of Chinese herbal medicine (shosaikoto) - a case re- port. Nihon Kokyuki Gakkai Zasshi 2003;41:300-303
13. Miyazaki E, Ando M, Ih K, Matsumoto T, Kaneda K, Tsuda T.
Pulmonary edema associated with the Chinese medicine shosaiko- to. Nihon Kokyuki Gakkai Zasshi 1998;36:776-780
14. Sato A, Toyoshima M, Kondo A, Ohta K, Sato H, Ohsumi A.
Pneumonitis induced by the herbal medicine Sho-saiko-to in Japan. Nihon Kyobu Shikkan Gakkai Zasshi 1997;35:391-395
J Korean Soc Radiol 2010;63:519-524
Address reprint requests to : Joung Sook Kim, M.D., Department of Health Promotion Medicine, Mokdong Hospital, Ewha Womans University, 911-1 Mok-dong , Yangcheon-gu, Seoul 158-710, Korea.
Tel. 82-2-2650-5922 Fax. 82-2-2650-5037 E-mail: [email protected]
Mixed Herbal Medicine Induced Diffuse Infiltrative Lung Disease:
The HRCT and Histopathologic Findings
1Tae Gyu Kim, M.D., Joung Sook Kim, M.D.2, Eun A Shin, M.D.3
1Department of Radiology, Sanggye Paik Hospital, Inje University
2Department of Health Promotion Medicine, Mokdong Hospital, Ewha Womans University
3Department of Pathology, Sanggye Paik Hospital, Inje University
Purpose: The purpose of this study was to evaluate the high-resolution CT (HRCT) and pathologic findings of mixed herbal medicine-induced diffuse interstitial lung disease.
Materials and Methods: Eight patients (6 women and 2 men, age range: 31 to 81 years, mean age: 51.4 years) who presented with cough or dyspnea after taking mixed herbal medicine were included in this study. All the patients underwent plain chest radiography and HRCT. We obtained pathologic specimens from 7 patients via fluoroscopy guided large bore cutting needle biopsy and transbronchial lung biopsy. All the patients were treated with steroid therapy.
Results: The most common HRCT finding was bilateral diffuse ground glass opacity (n=7), followed by peri- bronchial consolidation (n=5) and inter- or intralobular septal thickening (n=2). For the disease distribution, the lower lung zone was dominantly involved. The pathologic results of 7 patients were nonspecific interstitial pneumonia (n=3), bronchiolitis obliterans organizing pneumonia (n=2), hypersensitivity pneumonitis (n=1) and eosinophilic pneumonia (n=1). Irrespective of the pathologic results, all 8 patients improved clinically and radiologically after steroid treatment.
Conclusion: The HRCT findings of mixed herbal medicine-induced diffuse infiltrative lung disease were main- ly bilateral diffuse ground glass opacity, peribronchial consolidation and dominant involvement of the lower lung zone. Those pathologic findings were nonspecific and the differential diagnosis could include interstitial pneumonia, bronchiolitis obliterans organizing pneumonia, hypersensitivity pneumonitis and eosinophilic pneumonia.
Index words :Herbal Medicine Lung, Diseases
Tomography, X-Ray Computed