- 53 -
체위의존성 및 체위비의존성 수면무호흡 환자의 상기도 형태 비교
경북대학교 의학전문대학원 이비인후과교실
최재혁 · 장현욱 · 김태훈 · 정다정 · 석준호 · 김정수
Comparison of Upper Airway Morphology between Position-Dependent Sleep Apnea Patients and Position-Independent Sleep Apnea Patients
Jae Hyuk Choi, MD, Hyun-Uk Jang, MD, Tae Hoon Kim, MD, Da-Jung Jung, MD, Jun Ho Seok, MD and Jung Soo Kim, MD
Department of Otorhinolaryngology-Head & Neck Surgery, School of Medicine, Kyungpook National University, Daegu, Korea
ABSTRACT
Background and Objectives: The aim of this study is to compare polysomnography (PSG) data and upper airway morphol- ogy between a position-dependent sleep apnea (PDSA) group and a position-independent sleep apnea (PISA) group. Materi- als and Methods:This is a retrospective analysis into which 58 patients who were evaluated with overnight polysomnography, lateral cephalometry, and multidetector computed tomography (MD-CT, spiral CT scan) to diagnosis obstructive sleep apnea were enrolled. The patients were divided in two groups : the PDSA group who had a supine apnea-hypopnea index (AHI) that was at least two times higher than the non-supine AHI and the PISA group in whom the AHI in the supine position was less than twice that in the lateral position. Twelve cephalometric variables were measured. MD-CT measurements were evaluated in four neck levels from the hard palate to the top of the epiglottis. Minimal cross-sectional area (mCSA) and collapsibility in- dex (CI) were calculated at each level. Results:AHI was significantly higher in the PISA compared with PDSA. None of the cephalomeric measurements were significantly different between the two groups. In the MD-CT measurements, the mCSA of the low retropalate area (LRP) in the awake state was significantly lower in the PISA group compared to that in the PDSA group. In the sleep state, the CI was significantly higher in the high and low retroglossal areas (HRG and LRG) in the PISA compared to those in the PDSA group. Conclusion:In the supine position, PISA had increased collapsibility at the levels of the HRG and LRG during sleep compared to those in PDSA. In the future, a further evaluation with MD-CT in a non-supine po- sition is needed.
KEY WORDS:Sleep apneaㆍPolysomnographyㆍSpiral CT scan.
서 론
구조 이상이나 인두근의 이완작용에 의한 상기도 변화가 수면무호흡 환자에서 기도의 폐쇄를 일으킬 수 있다고 알 려져 있으며, 수면 중 반복되는 완전 혹은 불완전한 상기도 폐쇄는 수면의 단절을 야기하고 이로 인하여 과도한 주간
졸림, 피곤, 인지 장애 등을 유발할 뿐만 아니라 자동차 사 고의 한 원인으로도 알려져 있다.
1)수면무호흡 환자에서 앙와위 시에 측와위 시 보다 수면 중 무호흡이 더 빈발하게 발생한다는 여러 보고들이 있다.
2-4)따라서 수면무호흡 환자에서 수면 시에 무호흡 감소의 한 방법으로 측와위가 권유되나 보다 심한 수면 무호흡 환자에 서는 종종 체위변화에 따른 무호흡-저호흡 지수의 뚜렷한 개선이 없는 경우도 많아 체위의존성 수면무호흡 환자군과 체위비의존성 수면무호흡 환자군으로 나누어 분류되기도 하나
5)이들 두 군간의 상기도 형태의 차이에 대한 비교연구 는 미미한 실정이다.
이 논문은 2008년 경북대학교 학술연구비에 의하여 연구되었음.
논문접수일:2011년 1월 10일 / 심사완료일:2011년 4월 19일 교신저자:김정수, 700-721 대구광역시 중구 삼덕 2가 50 경북대학교 의학전문대학원 이비인후과교실
전 화:(053) 420-5777·전 송:(053) 420-4524 E-mail:[email protected]
저자들은 수면다원검사, 측면두개골계측, Multi Detector 컴퓨터 단층촬영(MD-CT)를 실시한 환자를 대상으로 수면 중 자세에 따른 무호흡의 변화의 정도에 따라 체위의존성 수면무호흡 환자군과 체위비의존성 수면무호흡 환자로 각 각 나누고 두 군간에 수면다원검사 결과와 각성 시 및 수면 시의 상기도의 형태를 비교 분석해 보고자 하였다.
대상 및 방법
대 상
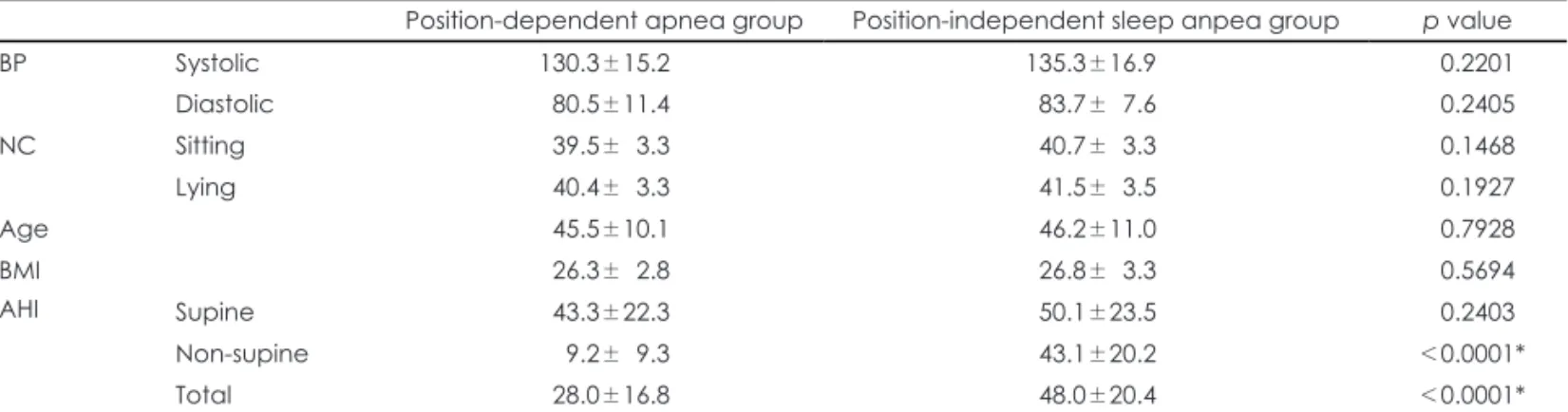
후향적 검사로 수면무호흡을 주소로 내원한 환자 중 수 면다원검사, 측면두개골계측 및 MD-CT 촬영 모두를 실시 하였던 환자 58명을 대상으로 하였으며 이들의 나이, 혈압, 목둘레, 체질량지수를 조사하였다(Table 1).
전산화 자동 수면다원검사(Beehive Millenium, Grass- Telefactor Inc., West Warwick, RI) 결과에서, 무호흡-저 호흡 지수가 5 이상인 환자 중 측와위 시 무호흡-저호흡 지 수가 50% 이상 개선되는 군을 체위의존성 수면무호흡 환 자군으로, 무호흡-저호흡 지수가 50% 이상 개선되지 않는 군을 체위비의존성 수면무호흡 환자군으로 정의하였으며 각각 38명과 20명이 해당되었다. 기본골격구조 및 상기도 의 형태의 비교를 위해 측면두개골 계측(Cephalometry, ASAHI CX-90SP Ashahi Tokyo, Japan)를 이용하여 하악 골에서 설골까지 길이(mandibular plane to hyoid, MPH) 를 포함해 전비극과 후비극을 연결한 선에 평행한 혀 뒤 기 도의 최소직경(posterior airway space, PAS), 후비극에 서 연구개천장까지 길이(the posterior nasal spine to the tip of soft palate ; soft palate length, SPL), 하악돌기에 서 턱끝융기점-전체 하악골길이(condyle to gnathion ; total mandibular length), 하악각점에서 턱끝융기점-하악골체 길이(gonion to gnathion; mandibular body length), 하 악돌기에서 하악각점-하악골가지높이(condyle to gonion ;
mandibular ramus height), 연구개의 가장 두꺼운 부위(the widest point of soft palate ; soft palate thickness, SPT), 인두길이(pharyngeal length, PhL), 후구개의 가장 좁은 공간(the smallest anteroposterior dimension of the retropalate space, RP), 후설부 공간(the retroglossal space, RG), 안장-비근점-치상점이 이루는 각(sella-na - sion-supradentale, SNA), 안장-비근점-치하점이 이루는 각(sella-nasion-infradentale, SNB) 등 총 12가지 변수 에 대해 조사하였다.
MD-CT
각성 및 수면시의 상기도 형태학적 변화를 관찰하기 위한 Muti-detector 컴퓨터 단층 촬영기(MD-CT, Light Speed Ultra 16, GE medical systems, Milwaukee, WI)를 이용한 검사는 이전의 저자들이 사용한 방법과 동일하게 시행되었 다.
6)이를 간단하게 살펴 보면, 환자들은 검사대 위에 먼저 각성 상태에서 앙와위 자세로 누운 후 경구개 시작부위부 터 후두개가 보이기 시작하는 위치까지를 8 부위로 나눈 후 호흡에 따른 기도변화를 알기 위하여 0.3초 간격으로 각 부 위 당 25회씩 반복 촬영하였고, 절편의 두께는 10 mm로 하였으며 영상 당 촬영시간은 0.4초로 총 검사시간은 60~
80초가 걸렸다. 이 후 5~10 mg의 Dormicum(Midazolam 0.1 mg/kg, 한국 로슈)을 정맥 주사하여 환자가 잠들어 코 를 골기 시작할 때 수면상태에서의 촬영을 각성상태에서 실시한 동일한 방법으로 시행하였다.
상기도의 부위별 특성을 알아보기 위해 경구개에서 후두 개가 보이기 시작하는 부위까지를 구개수끝을 기준으로 두 부위로 나누고 이를 다시 각각 이등분하여 상후구개부 (high-retropalate area, HRP), 하후구개구부(low-ret - ropalate area, LRP), 상후설부(high-retroglossal area, HRG), 하후설부(low-retroglossal area, LRG)의 네 부위 로 구분하였다(Fig. 1). 상기도 전체와 각 부위의 단면적 및
Table 1. Comparison of position-dependent sleep apnea patients and position-independent sleep apnea patients at the bloody pres- sure, neck circumference, body mass index, age and apnea-hypopnea index
Position-dependent apnea group Position-independent sleep anpea group p value
BP Systolic 130.3±15.2 135.3±16.9 0.2201*
Diastolic 080.5±11.4 83.7±07.6 0.2405*
NC Sitting 039.5±03.3 40.7±03.3 0.1468*
Lying 040.4±03.3 41.5±03.5 0.1927*
Age 045.5±10.1 46.2±11.0 0.7928*
BMI 026.3±02.8 26.8±03.3 0.5694*
AHI Supine 043.3±22.3 50.1±23.5 0.2403*
Non-supine 009.2±09.3 43.1±20.2 <0.0001*
Total 028.0±16.8 48.0±20.4 <0.0001*
* : p<0.05, Values are mean±SD. BP : blood pressure, NC : neck circumference, AHI : apnea-hypopnea index, BMI : body mass index
체적은 MD-CT에서 자동적으로 측정 및 제공되는 자료로 얻을 수 있었으며 이를 이용하여 각 부위별 평균 최소단면 적과 상기도가 호흡에 따라 단면적 및 체적의 변화를 나타 내는 허탈지수(Collapsibility index, CI)을 측정하였다. CI
는 호흡 주기 중 기도 단면적이 가장 클 때를 최대단면적 (maximal cross sectional area, MCSA)으로 정의하고 가 장 작을 때를 최소단면적(minimal cross sectional area, mCSA)으로 정의한 후 각 부위별로 측정한 후 다음과 같은 방법으로 산출하였다 ;
Callapsibility index=(MCSA-mCSA) 100/MCSA
통계분석
두 군간의 목둘레, 나이, 체질량지수, 무호흡-저호흡 지수 의 비교는 unpaired t-test로, 수면시의 상기도의 단면적 및 CI는 paired t-test를 사용하여 각성 시 상기도 상태와 비교하였다. 통계학적 유의 수준은 0.05 미만으로 하였다.
결 과
두 군간의 나이, 혈압, 목둘레, 체질량지수는 통계학적 차 이가 관찰되지 않았으나 무호홉-저호흡 지수는 체위비의 존성 수면무호흡 환자군에서 48.0±20.4, 체위의존성 환자 군에서는 28.0±16.8로 체위비의존성 수면무호흡 환자군 에서 의미 있게 높았다(p˂0.0001). 특히 앙와위에서는 두 군간에 통계적 차이는 없었으나 측와위 시에 체위비의존성 수면무호흡 환자군에서 무호흡-저호흡 지수가 유의하게 높은 결과를 보였다(Table 1).
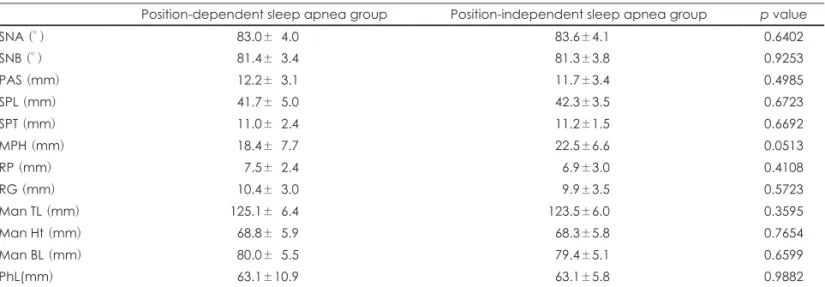
측면두개골계측에서 두 군간에 12개의 변수 중 수면무호 흡 환자의 골격형태에서 중요하게 여겨지는 하악골에서 설 골까지의 길이(MPH)는 체위변화성 수면무호흡 환자군에서 는 18.4±7.7, 비체위변화성 수면무호흡 환자군에서는 22.5
Fig. 1. The upper airway was classified as 4 levels. The area from the inferior border of the hard palate to the inferior border of the uvula is classified as the retropalate level : the area from the in- ferior border of the uvular to the superior border of the epiglottis tip as the retroglossal level. HRP : high retropalate area, LRP : low retropalate area, HRG : high retroglossal area, LRG : low retroglos- sal area.
HRP LRP HRG LGR
Table 2. Comparison of position-dependent sleep apnea patients and position-independent sleep apnea patients at the cephalomet- ric data
Position-dependent sleep apnea group Position-independent sleep apnea group p value
SNA (° ) 083.0±04.0 083.6±4.1 0.6402
SNB (° ) 081.4±03.4 081.3±3.8 0.9253
PAS (mm) 012.2±03.1 011.7±3.4 0.4985
SPL (mm) 041.7±05.0 042.3±3.5 0.6723
SPT (mm) 011.0±02.4 011.2±1.5 0.6692
MPH (mm) 018.4±07.7 022.5±6.6 0.0513
RP (mm) 007.5±02.4 006.9±3.0 0.4108
RG (mm) 010.4±03.0 009.9±3.5 0.5723
Man TL (mm) 125.1±06.4 123.5±6.0 0.3595
Man Ht (mm) 068.8±05.9 068.3±5.8 0.7654
Man BL (mm) 080.0±05.5 079.4±5.1 0.6599
PhL(mm) 063.1±10.9 063.1±5.8 0.9882
* : p<0.05, Values are mean±SD. SNA : sella-nasion-supradentale, SNB : sella-nasion-infradentale, PAS : posterior airway space, SPL : soft palate length, SPT : soft palate thickness, MPH : mandibular plane to hyoid, Man TL : condyle to gnathion-total mandibular length, Man Ht : condyle to gonion-mandibular ramus height, Man BL : gonion to gnathion-mandibular body length, RP : retropalatal, RG : ret- roglossal, PhL : pharyngeal length
±6.6으로 비체위변화성 환자군에서 더 길었으나 통계학적 유의성은 없었다(p=0.051). 그 외의 변수에서도 통계학적 차이는 관찰되지 않았다(Table 2).
MD-CT 결과에서 각성 시에서 측정한 4부위에서 최소 단 면적과 상기도 용적을 비교하였을 때 LRP에서 체위비의존 성 환자군에서 통계학적으로 유의하게 좁은 결과를 보였으 나, 수면 시에는 두 군간에 유의한 차이는 관찰되지 않았다 (Table 3).
CI의 비교 결과는 각성 시에는 LRP에서만 체위비의존성 수면무호흡 환자군(37.3±21.0)과 체위의존성 수면무호흡 환자군(51.5±26.4) 간에 통계학적으로 유의한 차이가 있었 다(
p=0.0299) 하지만 수면시에는 HRG와 LRG에서 체위비의존성 수면무호흡 환자군의 CI가 체위의존성 수면무호흡 환 자군에 비해 유의하게 높게 나타났으며(p=0.0211, 0.003), 상기도 전체용적의 CI도 체위비의존성 수면무호흡 환자군 에서 높은 것으로 나타났다(Table 4).
고 찰
Cartwright
2)는 수면무호흡 환자의 수면다원화검사에서 앙와위 시에 측와위 시 보다 무호흡 발생이 2배 가량 증가 되는 것을 확인하여 수면 중 측와위가 미치는 영향에 대해 처음으로 보고하였다. 이후 체위 변화에 따른 수면무호흡 상 태가 변하는 원인에 대한 연구는 다양하게 이루어져 왔다.
Table 3. Mean value of mCSA (mm2) at four level of upper air way and upper airway volume during awake and asleep at supine posi- tion by using MD-CT
Position-dependent sleep apnea group Position-independent sleep apnea group p value Awake
HRP 241.1±0108.5 303.9±0202.4 0.1281
LRP 102.9±0049.5 68.6±0050.6 *0.0158*
HRG 214.7±0095.7 206.7±0116.5 0.7801
LRG 262.1±0139.0 283.4±0150.6 0.5899
Volume 15801.7±5604.9 16197.8±5599.7 0.7990
Asleep
HRP 177.4±0112.5 213.0±0154.8 0.3189
LRP 20.9±0033.8 15.6±0016.7 0.5099
HRG 50.5±0054.0 46.3±0149.0 0.8778
LRG 105.8±0077.8 66.4±0069.4 0.0621
Volume 8275.2±4603.1 6350.1±3728.0 0.1128
* : p<0.05, Values are mean±SD. HRP : high retropalatal area, LRP : low retropalatal area, HRG : high retroglossal area, LRG : low retroglossal area, mCSA : minimal cross sectional area
Table 4. Mean value of collapsibility index (%) at four level of upper airway and upper airway volume during awake and asleep at su- pine position by using MD-CT
Position-dependent sleep apnea group Position-independent sleep apnea group p value Awake
HRP 26.1±18.1 25.1±13.9 0.8328
LRP 51.5±26.4 37.3±21.0 *0.0299*
HRG 23.6±17.6 29.1±22.1 0.3031
LRG 30.8±24.9 24.9±21.4 0.3781
Volume 19.2±14.9 18.9±14.2 0.9321
Overall CI 29.4±13.4 32.7±16.3 0.4255
Asleep
HRP 50.1±23.1 49.6±24.7 0.9317
LRP 83.5±18.9 80.3±16.7 0.5244
HRG 80.0±19.9 91.5±11.5 *0.0211*
LRG 72.6±21.4 88.4±10.4 *0.0030*
Volume 54.8±20.2 69.2±15.3 *0.0072*
Overall CI 71.6±16.2 77.4±11.2 0.1526
* : p<0.05, Values are mean±SD. HRP : high retropalatal area, LRP : low retropalatal area, HRG : high retroglossal area, LRG : low retroglossal area, CI : collapsibility index
Isono 등
7)은 상기도 주위의 연부조직과 하악과 척추 같은 골격구조에 의해 기본적인 상기도 형태가 이루어져 있으며 골격구조와 달리 연부조직은 자세에 따라 상기도 주변으로 분포하는 양이 다르다는 점에서 앙와위와 측와위를 취할 때 중력에 영향을 받는 연부조직의 양 때문에 상기도 단면 적이 달라 질 수 있다고 보고하였다. 즉, 앙와위 시 혀를 포 함한 연부조직이 측와위 시 보다 많아 상기도 단면적이 좁 아진다고 하였다. 또한 자세 변화에 따른 폐용량의 변화가 상기도 단면적에 영향을 미쳐 측와위 시 잔존 폐용량이 앙 와위를 취할 때 보다 증가하여 상기도의 단면적을 증가시 킬 수 있다는 보고도 있다.
8)9)Pevernagie 등은 수면무호흡 환자에서 환자의 자세를 앙와위에서 측와위로 변화시킨 후 상기도의 평균단면적을 전산화단층촬영으로 측정하여 수면무호흡 환자에서 측와위 자세에서 상기도 단면적이 증가됨을 보고하였다.
10)하지만 이는 각성 시 환자의 상기도 형태를 평가한 것으로 측와위 시 상기도 단면적의 증가가 각성 상태인 환자의 인두근의 작용으로 인한 영향을 배제할 수 없었다. 저자들의 이전 연 구에서 수면 중 측와위 및 복와위에서 앙와위에 비해 상기 도의 CI가 감소되고 기도 내경이 증가되며 특히 측와위가 기도 유지에 가장 유리하다는 것을 수면 중 촬영한 MD- CT 검사에서 통해 보고한 바 있다.
11)보다 심한 수면무호흡 환자에서는 종종 체위변화에 따른 무호흡-저호흡 지수의 뚜렷한 개선이 없어 체위의존성 수 면무호흡 환자군과 체위비의존성 수면무호흡 환자군으로 나누어 분류되기도 하며
5)본 연구에서도 체위비의존성 환자 군에서 수면무호흡이 더 심하게 나타나는 것을 관찰할 수 있 었다. 체위의존성 수면무호흡 환자군과 체위비의존성 수면 무호흡 환자군간에 신체적 특징을 비교했을 때 체위비의존 성 환자군에서 나이와 체질량지수가 유의하게 높다는 보고 가 있으나
5)본 연구에서는 두 군간에 나이, 목둘레, 체질량 지수의 차이는 발견할 수 없었으며 이는 인종간 혹은 환자 구성에서의 차이에 따른 것으로 판단된다.
이상과 같이 체위의존성 수면무호흡 환자군과 체위비의존 성 수면무호흡 환자군간에 수면다원검사나 인구학적 차이에 대한 연구는 다수 있었으나 상기도 형태의 차이에 대한 연 구는 미미하다. 체위비의존성 수면무호흡 환자군의 경우에 는 체위변화에 따른 수면무호흡을 감소시키는 요인을 방해 하는 상기도 형태의 변화가 있을 것이라 추측할 수 있으나 상기도의 역동적인 변화에 대한 연구, 특히 수면시의 비교 연구는 저자들이 조사한 바로는 현재까지 없다.
수면무호흡은 상기도의 반복적인 폐쇄로 발생하며 상기 도 폐쇄 부위의 확인은 환자의 치료 선택에 매우 중요하나,
현재까지 명확하게 폐쇄 부위를 확인할 수 있는 방법이 없 는 상태로 측면두개골계측, 컴퓨터단층촬영, 자기공명영상 등이 시도되어 왔다. 측면두개골계측은 안면부와 상부기도 연부조직의 구조적 이상을 관찰할 수 있는 검사로, 수면 무 호흡증 환자에서 하악의 후방전위, 좁은 후기도공간, 설골 하방전위 등을 관찰할 수 있어 수면무호흡 환자의 골격 및 연부조직을 측정하는 데 가장 많이 사용되고 있지만 2차원 영상으로 기도 용적을 평가 하는데는 제한이 있다. 단순 컴 퓨터단층촬영과 자기공명영상은 상기도 용적의 3차원적 재 구성이 가능하여 보다 정확한 상기도 평가가 가능하나 수면 상태에서 상기도의 역동적인 변화를 반영하는 데 어려움이 있다. 상기도의 역동적인 변화를 측정하기 위해 연성 비인두 내시경(fiberopitic nasopharyngoscope), 형광투시검사 (fluoroscopy), 전자선 단층촬영(electron beam tomogra- phy), multi-detector 컴퓨터 단층촬영(MD-CT) 등이 시도 되어 왔다. 그 중 MD-CT는 나선형의 컴퓨터 단층촬영을 기반으로 여러 개의 열로 구성된 검출기에 의해 1회 회전으 로 다수의 영상을 획득할 수 있어 스캔 시간이 단축되고 얇 은 두께의 스캔으로 해상력이 향상되며 다양한 면의 상과 3 차원 영상을 얻을 수 있는 장점이 있다. 또한 자동으로 측 정된 상기도 각 부위의 단면적 수치에서 최대 협착 부위 및 호흡에 따른 기도 면적의 변화 등의 측정이 가능하며 환자 의 실제 상기도 형태를 비교적 정확하게 반영할 수 있어 전 체적인 상기도의 변화를 쉽게 파악할 수 있다.
6)이전의 연구 에서 MD-CT를 이용하여 상기도의 부위별 mCSA와 CI를 측정하여 무호흡-저호흡지수와 상관관계가 있으며 특히 각성시 보다 수면시에 이들의 연관성이 보다 뚜렷하여 상 기도 형태연구 조사는 수면시에 이루어 져야 한다는 사실 을 밝힌 바 있다.
12)또한 비만도에 따른 상기도의 형태 차이 에 대한 연구에서 수면시의 상기도의 증가된 CI가 비만군 에서 높은 무호흡-저호흡지수의 원인으로 보고하여 수면 중 MD-CT 검사가 수면무호흡환자의 상기도 형태 연구에 유용하게 사용될 수 있음을 증명하였다.
13)측면두개골계측을 이용한 수면무호흡 환자의 골격 및 연
부조직 측정에서 정상인에 비해 높은 빈도의 하악후퇴증,
좁은 후기도 공간 등의 소견이 발견되었고 MPH의 길이 정
도가 수면무호흡에 영향을 미친다고 보고되었다.
14)이 요인
들이 체위의존성 수면무호흡 환자군과 체위비의존성 환자
군사이에 영향을 미치는 지 알아보기 위해 시행한 측면두
개골계측 결과에서는 체위비의존성 수면무호흡 환자군에서
MPH가 더 긴 양상을 나타냈으나 통계적 유의성은 없었고,
다른 변수에서도 두 군간에 차이를 발견할 수 없었다. 이는
수면무호흡 환자에서 골격 및 연부조직의 형태만이 아닌
기도용적이나 상기도의 역동적인 형태학적 차이가 두 군간 에 있을 것이라 추측할 수 있다.
MD-CT 결과에서 두 군간에 단면적의 차이는 없었으나 체위비의존성 수면무호흡 환자군에서 수면 시 HRG와 LRG에서 CI가 증가되어 있음을 관찰할 수 있었다. 수면무 호흡의 주된 병인의 하나는 수면 중 인두근의 허탈의 증가
이며,
15-18)설후방의 허탈의 증가는 수면무호흡의 정도를 더
욱 증가 시킬 가능성은 있으나 수면무호흡-저호흡지수는 앙 와위에서 두 군간에 통계적 차이는 없었다. 이는 저자들의 이 전의 연구에서 CI가 무호흡-저호흡지수와 상관관계가 있 다는 연구
12)와 일치하지 않으며 두 결과의 차이는 이전의 연 구에서 비록 CI가 무호흡-저호흡지수와 통계학적으로 의미 있게 연관성이 있었으나 상관계수가 낮았던 것이 한 원인 으로 환자 수 등의 차이에 영향을 받았을 것으로 판단된다.
본 연구는 후향적 조사로 앙와위에서만 두 군간의 형태 학적 변화에 대한 연구가 이루어져 측와위에서의 두 군간의 형태학적 차이에 대한 조사가 이루어 지지 않은 제한점을 가지고 있다. 일반적으로 측와위에서는 중력에 따른 주위 조직의 영향을 적게 받게 되나 체위비의존성 수면무호흡 환자군에서는 체위의존성 수면무호흡 환자군에 비해 무호 흡-저호흡지수의 차이가 앙와위 보다는 측와위에서 더 높 게 나타나는 결과를 미루어 보아, 체위비의존성 수면무호 흡 환자군에서는 측와위에서 기도 유지를 어렵게 하는 형 태학적 변화가 발생할 것으로 추측되며 향후 측와위에서의 기도형태 연구가 반드시 이루어져야 할 것으로 판단된다.
결 론
체위비의존성 수면무호흡 환자군이 체위의존성 수면무호 흡 환자군에 비하여 수면무호흡의 정도와 수면 중 앙와위 시에 설후방 부위에서 허탈지수가 높은 것으로 나타났으나 향후 보다 영향을 많이 미치는 측와위에서 두 군간의 기도 형태 변화에 대한 연구가 필요할 것으로 판단된다.
중심 단어:수면무호흡·자세변화·단층촬영.
저자역할(Author Contributions)
최재혁, 김태훈, 정다정, 석준호, 장현욱, 김정수는 본 연구에서 모든 자료에 접근할 수 있으며 자료의 완전성과 자료 분석의 정확 성에 책임을 지고 있습니다. 연구 기획:최재혁, 김정수. 자료 해 석 및 분석:김태훈, 석준호. 논문초안:최재혁, 김태훈. 논문수
정:장현욱, 정다정. 연구 총괄:김정수.
REFERENCES
1) Powell NB. Contemporary surgery for obstructive sleep apnea syndrome. Clin Exp Otorhinolaryngol 2009;2:107-14.
2) Cartwright RD. Effect of sleep position on sleep apnea severity.
Sleep 1984;7:110-4.
3) Pevernagie DA, Shepard JW Jr. Relations between sleep stage, posture and effective nasal CPAP level in OSA. Sleep 1992;15:162-7.
4) George CF, Millar TW, Kryger MH. Sleep apnea and body position during sleep. Sleep 1988;11:90-9.
5) Oksenberg A, Silverberg DS, Arons E, Radwan H. Positional vs non- positional obstructive sleep apnea patients: anthropomorphic, noc- turnal polysomnography, and multiple sleep latency test data. Chest 1997;112:629-39.
6) Lee KY, Lee CM, Choi YJ, Lee YJ, Jung SS, Kim JS. Comparision of electron beam tomography and multi detector computed tomog- raphy for dynamic upper airway study in snorers. J Rhinol 2004;
11:57-61.
7) Isono S, Tanaka A, Nishino T. Lateral position decreases collapsibili- ty of the passive pharynx in patients with obstructive sleep apnea.
Anesthesiology 2002;97:780-5.
8) Hoffstein V, Zamel N, Phillipson EA. Lung volume dependence of pharyngeal cross-sectional area in patients with obstructive sleep apnea. Am Rev Respir Dis 1984;130:175-8.
9) Rehder K, Hatch DJ, Sessler AD, Fowler WS. The function of each lung of anesthetized and paralyzed man during mechanical venti- lation. Anesthesiology 1972;37:16-26.
10) Pevernagie DA, Stanton AW, Sheedy PF 2nd, Daniels BK, Shepard JW Jr. Effects of body position on the upper airway of patients with obstructive sleep apnea. Am J Respir Crit Care Med 1995;152:179-85.
11) Sohn JH, Choi YJ, Lee CM, Jang HU, Kim JH, Lee KY, et al. Ef- fect of the body position changes on upper airway caliber in obstruc- tive sleep apnea during sleep. Korean J Otolaryngol 2005;48:1242-7.
12) Heo JY, Kim JS. Correlation between severity of sleep apnea and upper airway morphology: cephalometry and MD-CT study during awake and sleep states. Acta Oto-Larngologica in press.
13) Kim TH, Chun BS, Lee HW, Kim JS. Differences of upper airway morphology according to obesity: Study with cephalometry and dynamic MD-CT. Clinical and Experimental Otorhinolaryngology 2010;3:147-52.
14) Maltais F, Carrier G, Cormier Y, Series F. Cephalometric measure- ments in snorers, non-snorers, and patients with sleep anpoea. Tho- rax 1991;46:419-23.
15) Horner RL. Motor control of the pharyngeal musculature and impli- cations for the pathogenesis of obstructive sleep apnea. Sleep 1996;
19:827-53.
16) Ryan CF, Love LL. Mechanical properties of the velopharynx in obese patients with obstructive sleep apnea. Am J Respir Crit Care Med 1996;154:806-12.
17) Robert JL, Reed WR, Mathew OP, Menon AA, Thach BT. Assess- ment of pharyngeal airway stability in normal and micrognathic infants. J Appl Physiol 1985;58:290-9.
18) Schwartz ARN, Schubert N, Rothman W. Effect of uvulopalato- pharyngoplasty on upper airway collapsibility in obstructive sleep apnea syndrome. Am Rev Respir Dis 1992;145:527-32.