Vol. 20, No. 2, June, 2012 □ 증 례 □
1)
Introduction
Guillain Barre Syndrome (GBS) is an acute ascending inflammatory demyelinating polyneu- ropathy thought to be caused by antibodies to
접수 :2012년 6월2 ,일 수정:2012년7월 25일
승인 :2012년 7월28일
책임저자 : 고태성 울산대학교 의과대학 아산병원 소아청소년과,
Tel: 02)3010-3381, Fax: 02)3010-3725
E-mail: [email protected]
gangliosides on the axolemma, which leads macrophages to invade the axon at the node of Ranvier
1). Typical clinical findings are progres- sive weakness starting from the limbs, with or without sensory deficit. The weakness may last for several weeks before good recovery, or it may remain as a chronic disability. Trans- verse myelitis is an inflammatory disorder, characterized by acute or subacute motor, sen- sory, and autonomic spinal cord dysfunction,
Concurrent Gullain-Barre Syndrome and Acute Transverse Myelitis as an Initial Presentation
of Systemic Lupus Erythematosus
Sung-Han Kang, K.D., Mi-Sun Yum, M.D.
*, Eun-Hye Lee, M.D.
*, † and Tae-Sung Ko, M.D.
*
Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine
*
Department of Pediatrics, College of Medicine, Kyung Hee University
†Seoul, Korea
= Abstract =
Systemic lupus erythematosus (SLE) is an autoimmune disorder involving multiple organs.
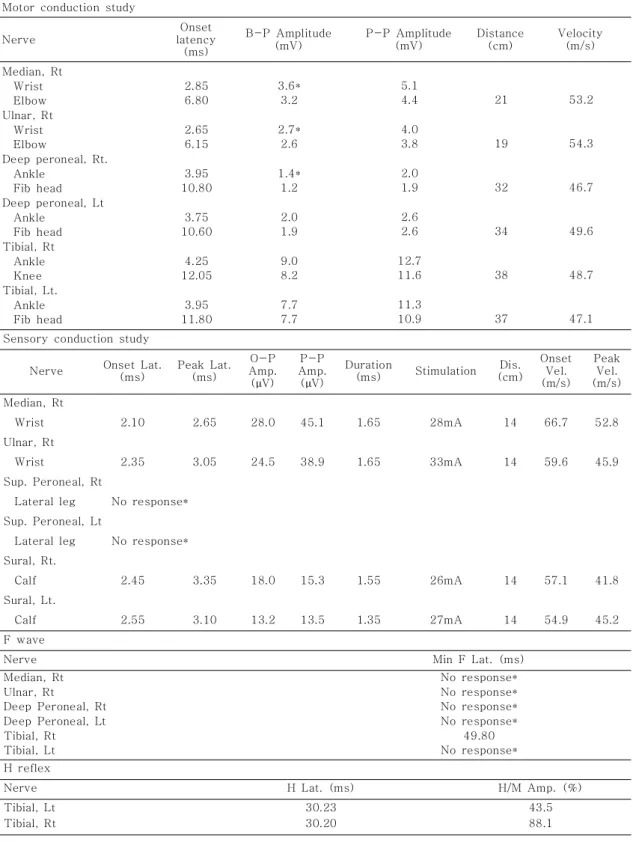
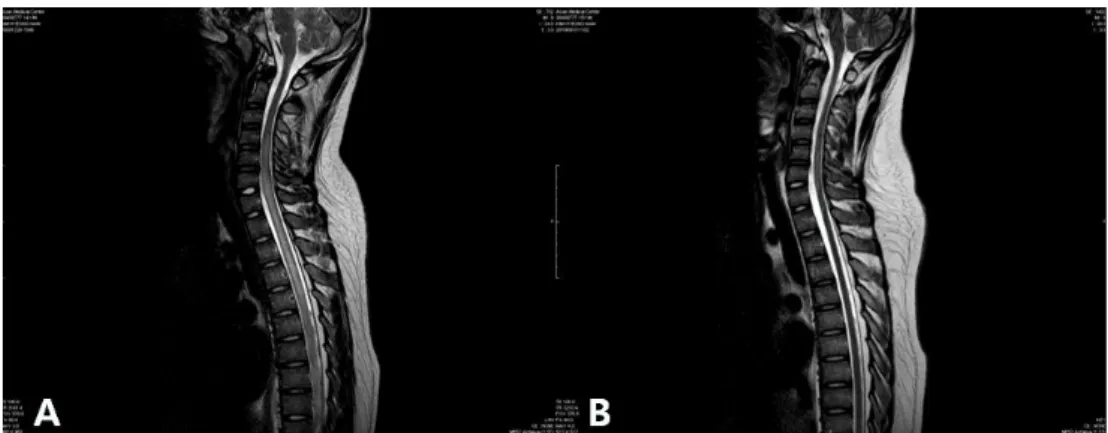
Neuropsychiatric symptoms are frequently associated in SLE, which is referred to as neurop- sychiatric SLE (NPSLE). NPSLE contains both central and peripheral nervous systems, which includes transverse myelitis, and Guillain-Barre syndrome (GBS). We report our experience of concurrent manifestation of transverse myelitis and GBS as an initial presentation of SLE, which suggests the common immune-mediated mechanisms of diseases. We here report the case of a 14-year-old boy with SLE who first presented with features of GBS. The patient developed ascending weakness starting from low extremities, experienced difficulty voiding, and had a facial rash. An initial diagnosis of GBS was made on the basis of clinical findings and nerve conduction studies. But he did not respond to intravenous immunoglobulin therapy and following spine MRI displayed T2 weighted high signal intensities from the cervical to thoracic region of the spinal cord, and serological analysis revealed the presence of anti- dsDNA, anti-smAb, anti nuclear antibody with decreased level of complements. The diagno- sis was revised to GBS and acute transverse myelitis resulting from SLE. Additional methyl- prednisolone pulse therapy led to rapid clinical improvement. This was followed by oral pred- nisolone and cyclophosphamide pulse therapy. This is the first case of concurrent manifesta- tion of GBS and transverse myelitis as initial presentation of SLE. The cross-reactivity of autoantibodies and increased susceptibility to infection owing to immunologic changes asso- ciated with lupus may form the basis of the association. Clinicians should consider a diagno- sis of SLE as an etiology of GBS or transverse myelitis.
Key Words : Guillain-Barre syndrome, Transverse myelitis, Systemic lupus erythematosus