서 론
만성신장병(Chronic Kidney Disease, CKD)은 세계적인 공중보건문제로 대두되고 있다. 미국의 경우 2003 USRDS 자료에 의하면 약 2,000만 명의 만성신장병 환자가 있는 것으로 보고되었다.1) 만성신장병은 말기신 장병(End-stage Renal Disease, ESRD)으로 진행될 뿐 아니라, 만성신장병 자체가 전신죽상경화증과 관상동맥병 발생의 독립적 위험인자임이 점차로 밝혀지고 있다.2-5) 또한 만성신장병은 심한 관상동맥병과 연관성이 있 으며 심장혈관병의 예후에도 악영향을 미치는 것으로 알려졌다.5-9) 따라서 만성신장병 환자는 심장혈관병에 의한 이환과 사망의 위험성이 높다. 현재까지의 연구에 의하면 만성신장병의 조기 진단과 치료는 신부전으 로의 진행과 그 합병증을 방지 또는 둔화시킬 수 있다고 알려졌다.10,11)
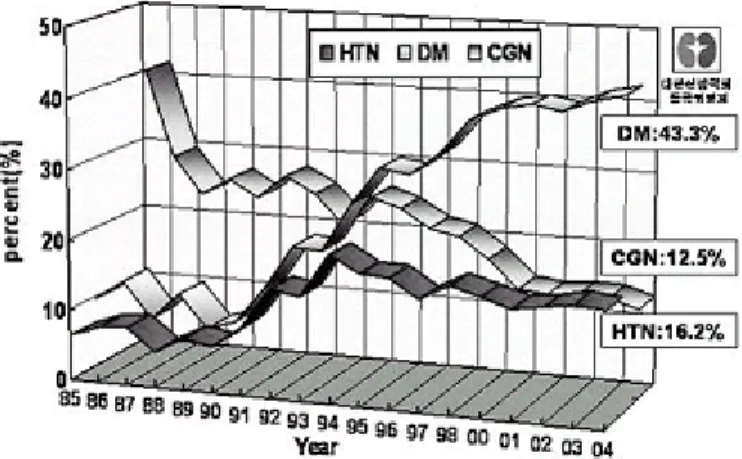
당뇨병성 신증은 만성신장병의 주요 원인 중의 하나이다. 대한신장학회의 2004년도 우리나라 신대체요법 현황에 의하면 말기 신부전 환자 수의 증가는 인구의 증가보다 훨씬 높은 비율로 계속되고 있으며 인구 백만 명당 말기 신장병 환자수가 1,000명에 근접하고 있어 전 세계적으로도 10위 정도의 높은 유병률 및 발병률을 보이고 있고, 특히 당뇨병에 의한 말기 신부전 환자 비율은 거의 절반 정도로 전 세계적으로도 가장 높은 수준으로 보고되었다(Figure 1). 최근의 연구에 의하면 제1형과 제2형 당뇨병에서 당뇨병성 신증 위험도는 비슷한 것으로 알려졌다. 당뇨병성 신증의 누적 발생률은 제1형의 경우 당뇨병 발병 후 40년쯤에
외래에서 노인의 당뇨병성 신증 관리
최 규 복
이대목동병원 신장내과
Figure 1. Three major causes of ESRD in Korea.
약 20∼40%이나 제2형의 경우는 대략 20 % 미만으로 알려졌다. 그러나 노인 인구가 증가하고, 특히 고혈압 과 관상동맥병의 효과적인 치료로 장기 생존하여 말기신장병 환자 수는 제 2형 당뇨병 환자가 더 많다.12) 대한신장학회의 2004년도 우리나라 신대체요법 현황에 의하면 투석환자의 연령별 분포가 1986년 본 조사 초기의 연령별 환자 분포와 비교하여 보면 20대 환자와 30대 환자수가 감소하고 50대 이후의 투석환자 비율이 계속적으로 증가하였으며 2002년부터는 50대 환자 비율보다 60대 환자 비율이 더 커져 가장 많은 투석 환자 연령대는 60대로 보고되었다(Figure 2).
따라서 노인 당뇨병성 신증의 예방과 조기진단 및 치료는 특히 중요하다. 이 글에서는 만성신장병 및 당뇨병성 신증의 주요 위험인자인 혈당조절과 고혈압을 중점으로 다루었다.
정 의
1. 당뇨병성 신증의 정의
당뇨병성 신증의 임상적 정의는 지속적인 단백뇨와 함께 사구체 여과율의 감소 및 혈압의 증가를 동반하 는 임상증후군을 의미한다.13)
2. 만성신장병의 정의
만성신장병의 정의는 3개월 이상 신장 손상이나 신장 기능 감소의 증거를 보이는 경우이다. 신장기능 감소는 사구체 여과율이 90 ml/min/1.73 m2 미만을 의미하며, 60 미만인 경우는 신기능 감소가 현저한 것으 로 간주된다. 신장 손상은 병리학적 이상, 혈액이나 소변의 이상, 또는 영상 검사상의 이상을 포함한다.
만성신장병의 병기는 원인 질환과 무관하게 신장 손상 유무나 사구체 여과율에 의해 결정된다(Table 1).
그러나 임상양상은 원인 질환에 따라 틀릴 수 있다.
Figure 2. Age distribution of dialysis patients according to years in Korea.
진 단
1. 알부민뇨(Albuminuria)
알부민은 대부분의 당뇨병성 만성신장병 환자의 총 요단백 중 약 40%를 차지한다. 알부민뇨와 단백뇨는, 특히 당뇨병성 신증에서, 신장 손상의 조기 표식자일 뿐 아니라, 심장혈관병의 예민한 지표이고 C-반응 단백과 연관성이 높다.
요중 알부민 배설양의 측정은 만성신장병 진단에 중요하다. 하루 요중 알부민 배설량이 30∼299 mg인 경우를 “미세알부민뇨(microalbuminuria)”라 하며 일반적인 dipstick에 의한 소변 검사로는 검출되지 않는다.
그러나 발열, 운동, 심부전, 요로감염, 고혈당 등에 의하여 일시적 미세알부민뇨를 보일 수 있고,14) 나날의 변동(day-to-day variability)이 있을 수 있다. 따라서 미세알부민뇨의 진단은 3∼6개월 내에 한 달 이상의 간격 을 두고 요검사를 3 회 실시하여 2회 이상 하루 요중 알부민 배설량이 30,299 mg인 경우에 내릴 수 있다.
미세알부민뇨의 선별검사는 3가지 방법을 이용한다(Table 3).
1) 무작위 단회뇨의 알부민/크레아티닌 비; 가장 쉬운 방법으로 외래에서 시행하기에 좋은 방법이다.
알부민/크레아티닌 비가 30 mg/g, 30μ/mg, 또는 0.03 mg/mg 이상이면 미세알부민뇨가 있다고 볼 수 있다.
2) 24 시간 요 측정
Table 1. Stages of CKD
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Stage Description GFR (ml/min/1.73m
2)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 1. Kidney damage with normal or increased GFR ≥ 90 2. Kidney damage with mild decrease in GFR 60∼89*
3. Moderate decrease in GFR 30∼59
4. Severe decrease in GFR 15∼29
5. Kidney failure (ESRD) <15 or dialysis
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*: Maybe normal age.
Table 2. Clinical features of Diabetic and Vascular CKD
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Stage Description Diabetic CKD Vascular CKD
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ At increased risk DM, hypertension, family history Hypertension, family history
DM duration 5∼10 yrs, Microalbuminemia
retinopathy, rising BP
1∼2 Kidney damage Microalbuminuria
DM duration 10∼15 yrs,
Macroalbuminuria
retinoapthy, hypertension Hypertension, retinopathy, CVD,
3∼4 Decreased GFR Hypertension complications
diabetic complications Retinopathy, CVD,
5 ESRD Uremia, CVD
diabetic complications, uremia
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ BP: blood pressure, CKD: chronic kidney disease, CVD: cardiovascular disaease, EDRD: end-stage renal disease, GFR:
glomerular filtration rate. From Bakris GL: AJH 18: 112S-119S, 2005.
3) 일정 시간 요 측정; 4 시간 또는 그 이상의 일정 시간 동안의 요 측정.
상기의 방법을 시행하기 어려운 경우는 Clinitek Microalbumin Dipsticks 또는 Micral-Test IItest strips 같은 semiquantitative dipsticks를 사용할 수도 있다.
제1형 당뇨병 환자의 경우는 미세알부민뇨 선별 검사를 당뇨병 진단(발병) 5년 후로 미룰 수 있으나, 제2 형 당뇨병 환자에서는 당뇨 발병 시기가 명확하지 않으므로 당뇨병 진단 즉시 선별 검사를 시행한다. 최초 선별 검사에서 미세알부민뇨가 없는 경우에는 1년마다 선별 검사를 시행한다.
2. 신장 기능: 사구체여과율
혈청 크레아티닌 농도만으로 신장 기능을 평가해서는 안 된다. 미국 National Kidney Foundation에서는 혈 청 크레아티닌 농도를 이용한 예측 방정식을 이용하여 사구체여과율을 추정할 것을 권유하였다.
1) The Cockroft-Gault formula:
(140-age in years)×(body weight in kilograms)
GFR=
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ ×(0.85 if female) Serum creatinine (mg/dl)×72
Table 3.
Definitions of abnormalities in albumin excretionꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Spot collection 24-h collection Timed collection Category
(μg/mg creatinine) (mg/24 h) (μg/min) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Normal <30 <30 <20
Microalbuminuria 30∼299 30∼299 20∼299
Clinical albuminuria ≥300 ≥300 ≥200
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Because of variability in urinary albumin excretion, two of three specimens collected within a 3- to 6-month perios should be abnormal before considering a patient to have crossed one of these diagnostic threshols. Exercise within 24 h, infection, fever, congestive heart failure, marked hyperglycemia, marked hypertension, pyuria and hematuria may elevate urinary albumin excretion over baseline values.
Table 4.
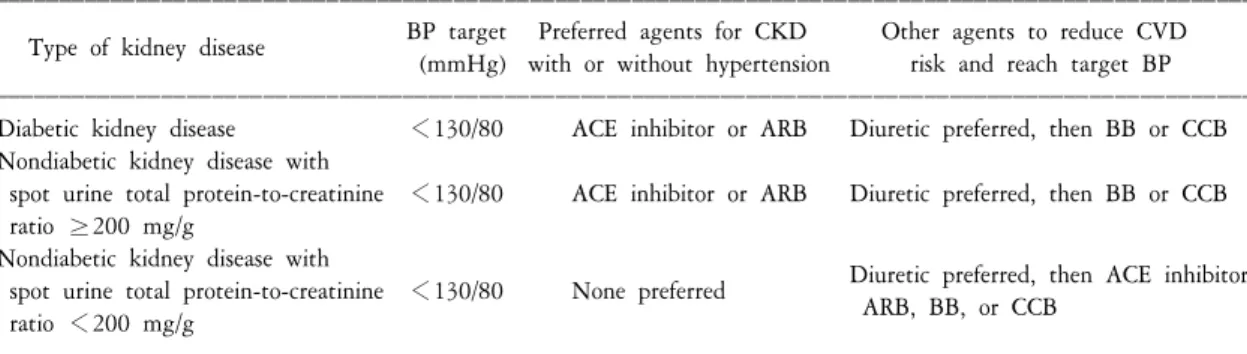
Hypertension and antihypertensive agents in chronic kidney diseaseꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
BP target Preferred agents for CKD Other agents to reduce CVD Type of kidney disease
(mmHg) with or without hypertension risk and reach target BP ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Diabetic kidney disease <130/80 ACE inhibitor or ARB Diuretic preferred, then BB or CCB Nondiabetic kidney disease with
spot urine total protein-to-creatinine <130/80 ACE inhibitor or ARB Diuretic preferred, then BB or CCB ratio ≥200 mg/g
Nondiabetic kidney disease with
Diuretic preferred, then ACE inhibitor spot urine total protein-to-creatinine <130/80 None preferred
ARB, BB, or CCB ratio <200 mg/g
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
ACE: angiotensin-converting enzyme, ARB: angiotensin receptor blocker, BB:β-blocker; BP=blood pressure, CCB: calcium channel
blocker, CKD: hronic kidney disease, CVD=cardiovascular disease. Adapted with permission from the National Kidney Foundation; K/DOQI clinical
practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis 2004;43(Suppl 1):S1-S290.
2) The Modification of Diet in Renal Disease (MDRD) equation:
GFR=186×(plasma creatinine)-1.154×(age)-0.203×(0.742 if female)×(1.210 if black)
두 방법 중에서 체중의 영향이 없는 MDRD equation이 당뇨병성 신증 환자에서 Cockroft-Gault formula보다 좀더 정확하다고 알려졌다.15,16)
당뇨병성 신증의 예방 및 치료
1. 일차 예방(Primary Prevention)
1) 혈당조절: 1형 및 2형 당뇨병 환자에서 철저한 혈당 조절을 하면 미세단백뇨의 발생 위험도를 낮출 수 있다.17,18) HbA1c 수치를 8.1% (역치) 아래로 혈당 조절을 하여야 한다는 보고가 있으나,19) 특정 HbA1c 역치는 없고 HbA1c 수치를 낮게 유지할수록 미세단백뇨의 발생 위험도를 더욱 낮출 수 있다는 보고도 있다.20,21)
2) 전신 혈압조절: 제2형 당뇨병 환자에서 철저한 혈압 조절은 당뇨병성 신증의 발생 위험도를 낮출 수 있다고 보고되었다.22) 혈압 조절에 있어서도 역치는 없는 것으로 보고되었으나,23) 일반적으로 혈압의 허용 상한치는 130/80 mmHg 정도이고, 항고혈압제의 종류보다는 혈압 조절 정도가 더 중요한 것으로 알려졌다.
그러나 제1형 당뇨병 환자에서 혈압 조절이 일차 예방 효과가 있는지는 아직 밝혀지지 않았다.
2. 이차 예방(Secondary Prevention)
1) 혈당조절: 당뇨병 환자에서 적극적인 혈당 조절은 미세알부민뇨에서 현성단백뇨(overt proteinuria, macroalbuminuria), 말기신부전으로 진행하는 것을 방지 또는 지연시킬 수 있다.
종래에는 당뇨병성 신증 환자에서 일단 현성 단백뇨를 보이면 혈당 조절을 철저히 하더라도 신장 손상이 진행되는 것을 막을 수 없다고 알려졌다. 그러나 최근의 연구에 의하면 장기간 정상혈당이 유지되는 췌장 이식환자에서는 신장 손상의 진행이 둔화되거나 당뇨병성 사구체 및 세뇨관 병변이 호전될 수도 있다고 보고되었다.24,25)
2) 사구체 내 혈압조절: 사구체 고혈압은 당뇨병성 신증의 특징으로 주된 병인은 안지오텐신 II에 의한 날토리세동맥(efferent glomerular arteriole)의 수축에 기인한다. 따라서 전신 고혈압 유무에 상관없이 제1형 및 제2형 당뇨병환자에서 레닌-안지오텐신계 억제제(ACE 억제제 또는 angiotensin-receptor blocker, ARB)가 가장 우수한 치료제이다.26,27)
3) 전신 혈압조절: 고혈압은 당뇨병선신증을 악화시키는 주요 인자이다. 미세알부민뇨를 동반한 제1형 및 제2형 당뇨병성 신증 환자에서 ACE 억제제나 ARB는 신장병 진행을 억제하는데 효과적이다.28) 현성단백 뇨를 보이는 경우에는 제1형 당뇨병성 신증에서는 ACE 억제제가 더욱 효과적이고,29) 제2형 당뇨병성 신증 에서는 ARB가 좀더 효과적인 것으로 알려졌다.30) 혈압 조절 목표는 130/80 mmHg 아래로 조절하여야 한다.
그러나 수축기 혈압이 100 mmHg 아래로 내려가는 것은 피해야 한다.
ACE 억제제 최대용량에 ARB를 병용하면 알부민뇨나 혈압 조절에 더 효과적이라는 보고도 있다.31) 그러 나 두 제제를 당뇨병성 신증 진단 당시부터 병용하거나 또는 순차적으로 사용하는 것 중 어느 것이 좋은지 는 아직 확실하지 않다.
ACE 억제제나 ARB로 혈압 조절이 적절하지 못한 경우는 일차적으로 이뇨제를 추가하는 것이 좋고, 다음 에 칼슘통로차단제(calcium channel blocker, CCB)나 베타차단제를 추가 할 수 있다. CCB로는 nondihydropyridine CCB (diltiazem, verapamil)가 당뇨병성신증 환자에서 ACE 억제제나 ARB와 유사한 효과를 얻을 수 있다. 그러 나 dihydropyridine CCB (nifedipine, nitrendipine, amlodipine 등)는 들토리세동맥을 확장시켜 사구체 고혈압을 유발할 수가 있고, 당뇨병성 신증 환자에서 알부민뇨 감소효과가 적으므로 사용하지 말아야 하며,32) ACE 억제제나 ARB와 병용할 경우에는 추가해볼 수 있다.
노인 당뇨병성 신증 환자
65세 이상의 노인 당뇨병환자를 대상으로 한 철저한 혈당 조절, 혈압 조절, 그리고 고지혈증 치료의 득실 에 대한 장기적인 연구는 없다. 노인 당뇨병 환자는 조기 사망, 기능적 장애, 고혈압, 관상동맥병, 그리고 뇌중풍 등의 빈도가 당뇨병이 없는 노인보다 높다. 따라서 장기간의 철저한 당뇨병 치료의 효과를 기대할 수 있을 정도로 여명이 남아 있고(10년), 활동적이고, 인지 능력이 온전하며, 자가 관리에 충실 할 수 있는
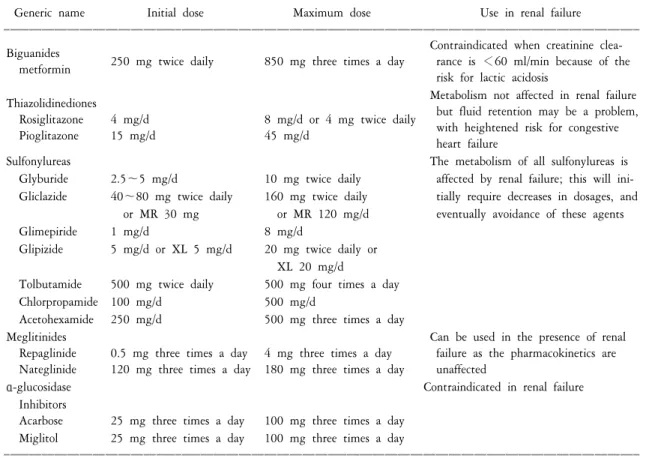
Table 5. Summary of oral antihyperglycemic agents
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Generic name Initial dose Maximum dose Use in renal failure
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Contraindicated when creatinine clea- Biguanides
250 mg twice daily 850 mg three times a day rance is <60 ml/min because of the metformin
risk for lactic acidosis
Metabolism not affected in renal failure Thiazolidinediones
but fluid retention may be a problem,
Rosiglitazone 4 mg/d 8 mg/d or 4 mg twice daily
with heightened risk for congestive
Pioglitazone 15 mg/d 45 mg/d
heart failure
Sulfonylureas The metabolism of all sulfonylureas is
Glyburide 2.5∼5 mg/d 10 mg twice daily affected by renal failure; this will ini- Gliclazide 40∼80 mg twice daily 160 mg twice daily tially require decreases in dosages, and
or MR 30 mg or MR 120 mg/d eventually avoidance of these agents
Glimepiride 1 mg/d 8 mg/d
Glipizide 5 mg/d or XL 5 mg/d 20 mg twice daily or XL 20 mg/d
Tolbutamide 500 mg twice daily 500 mg four times a day
Chlorpropamide 100 mg/d 500 mg/d
Acetohexamide 250 mg/d 500 mg three times a day
Meglitinides Can be used in the presence of renal
Repaglinide 0.5 mg three times a day 4 mg three times a day failure as the pharmacokinetics are Nateglinide 120 mg three times a day 180 mg three times a day unaffected
α-glucosidase Contraindicated in renal failure
Inhibitors
Acarbose 25 mg three times a day 100 mg three times a day Miglitol 25 mg three times a day 100 mg three times a day
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
J Am Soc Nephrol. 2005;16(Suppl 1):S7-S10.
경우에는 젊은 성인의 경우와 같이 치료할 수 있을 것이다(Table 5, 6).33-35)
1. 혈당조절
- 당뇨 합병증이 심하거나, 여명을 단축시킬 수 있는 공존 질환이 있거나, 또는 인지/기능 장애가 있는 경우에는 철저한 혈당 조절을 피하는 것이 좋다.
- 내분비 인슐린은 간에서 파괴되나, 외부 주입 인슐린은 주로 신장을 통해 제거된다. 사구체여과율이 20 ml/min 아래로 감소하면 제1형 및 제2형 당뇨병 모두에서 인슐린 제거율이 감소하여 인슐린 요구량이 줄게 된다. 일반적으로 사구체여과율이 10∼50 ml/min인 경우는 인슐린 용량을 25% 감량하고, 10 ml/min 아래이면 50% 감량하는 것이 좋다.
- Metformin (Glucopharge)은 신장으로 배설되므로 신기능이 저하된 환자에서는 젖산혈증이 올 수 있다.
크레아티닌 청소율이 30∼60 ml/min에서는 적은 용량을 사용해볼 수 있으나, 30 ml/min 아래에서는 투여하 지 말아야 한다.
- Thiazolidinediones [TZDs: rosiglitazone (Avandia), pioglitazone (Actos)]은 부종과 울혈심부전증을 유발할 수 있으므로 NYHA class 3&4 울혈심부전 환자에서는 금기이다.
- Sulfonylurea 계통 중에서는 신기능이 저하되어도 용량 조절이 필요하지 않는 Glipizide를 투여하는 것이 좋다. 그러나 심한 신기능장애가 있으면 금기이다.
2. 혈압조절
- 노인에서는 합병증을 피하기 위하여 혈압을 서서히 낮추는 것이 좋다. 엄격한 혈당조절의 경우와 마찬 가지로 혈압을 130/80 mmHg 이하로 철저하게 조절해야 할 타당한 근거가 없다면 과도한 혈압조절의 위험 성을 피하기 위하여 혈압을 140/90 mmHg 이하로 온건하게 조절하는 것이 현실적일 수도 있다.
- ACE 억제제나 ARB 제제를 투여하고 나서 2개월 내에 혈청 크레아티닌이 30% 이상 증가하면 신동맥협
Table 6. Recommendations for management of diabetes in adults
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
ADA AGS AMDA
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Glycemic control
A1c <7% <8% <7%
Preprandial capillary plasma glucose 80∼120 mg/dl 90∼130 mg/dl Peak postprandial capillary plasma glucose <180 mg/dl <180 mg/dl Blood pressure
All diabetics <130/80 mmHg <140/90 mmHg 130/80 mmHg
Overt proteinuria <125/75 mmHg
Lipids
LDL cholesterol <70∼100 mg/dl
Triglycerides <150 mg/dl
HDL cholesterol >40 mg/dl
Eye examinations Yearly dilated exams Every 2 years if Once or twice yearly for all low risk
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ A1c: glycosylated hemoglobin, ADA: American Diabetes Association, AGS: American Geriatrics Society, AMDA: American Medical Directors Association, HDL: high-density lipoprotein, LDL: low-density lipoprotein. From J Am Med Dir Assoc. 2006;
7:234-34.
착의 가능성을 배제하여야 한다.
- ACE 억제제나 ARB 제제는 신기능 보호와 심혈관 위험도를 낮추는데 효과적이므로 혈청 칼륨 농도가 5.5∼6 mEq/L 이상이 되지 않는 한 투여해볼 수 있다. 만약 고칼륨혈증이 발생하면 ACE 억제제나 ARB 제제 용량을 50% 감량하고 2∼4주 내에 기저치로 회복되지 않으면 ACE 억제제나 ARB 제제 투여를 중단해야 한다.
K/DOQI Recommendations in Diabetic Kidney Disease
36)1. Evaluation - CKD
- CVD and CVD risk factors
2. Diet and other therapeutic lifestyle changes for all patients - Dietary sodium intake <2.4 g/d
- BMI ≤25 kg/m2
- Exercise and physical activity - Moderation of alcohol intake - Smoking cessation
3. Diabetes therapy
- Diabetes therapy for all (ADA guidelines)
4. Therapy for other CVD risk factors
- Dyslipidemia (NCEP guidelines, K/DOQI guidelines )
5. ACE inhibitor or ARB
- ACE inhibitor or ARB for type 1 and type 2 diabetes with spot urine albumin-to-creatinine ratio 30∼300 mg/g (microalbuminuria)
- ACE inhibitor preferred for type 1 diabetes with spot urine albumin-to-creatinine ratio >300 mg/g (macro- albuminuria)
- ARB preferred for type 2 diabetes with spot urine albumin-to-creatinine ratio >300 mg/g (macroalbuminuria) - Either agent can be used as an alternative agent, if the preferred agent cannot be used.
- Use moderate to high doses
6. Systolic blood pressure goal <130 mmHg - Add diuretic first
- Then add CCB or beta-blocker
- Avoid dihydropyridine CCB without an ACE inhibitor or ARB.
7. For patients with spot urine total protein-to-creatine ratio >500∼1,000 mg/g - Consider a lower systolic blood pressure goal
- Consider measures to reduce proteinuria - increase dose of ACE inhibitor or ARB - Use ACE inhibitor or ARB in combination
- Add or increase dosage of other agents that lower proteinuria
8. Monitor serum potassium
- ACE inhibitors or ARBs may cause hyperkalemia.
- Avoid other medications that cause hyperkalemia, if possible (potassium supplements, NSAIDs, Cox 2 inhibitors, potassium sparing diuretics)
- Evaluate causes of hyperkalemia - Treat hyperkalemia with diuretics
- Continue ACE inhibitor or ARB if serum potassium ≤5.5 mEq/L.
- Diuretics may cause hypokalemia.
- Evaluate causes of hypokalemia.
- Treat hypokalemia with caution in CKD
9. Monitor GFR
- If GFR declines >30% from baseline within 4 weeks, eveluate causes.
- Continue ACE inhibitor or ARB if GFR decline is <30% from baseline value over 4 months.