Index terms
Lymphoepithelioma-Like Carcinoma Computed Tomography
INTRODUCTION
Epstein-Barr virus (EBV) affects the pathogenesis of various tu- mors. EBV may play an oncogenic role in nasopharyngeal carci- noma, Burkitt’s lymphoma, sinonasal T-cell lymphoma, B-cell lymphoma, and Hodgkin’s lymphoma (1, 2). Primary gastric lym- phoepithelioma-like carcinoma (LELC) resembles the histologic pattern of nasopharyngeal cancer. It is reported that over 80% to 90% of gastric LELC demonstrate EBV infections (3). LELC of the stomach is a rare type of undifferentiated carcinoma with an in- tense lymphoplasmacytoid stroma, which was first described in 1976 (4). Histologically, primary gastric LELC demonstrates moderate-poorly differentiation with prominent intratumoral lymphocytic infiltration (5, 6). Patients with EBV-associated LELC have a better prognosis than those with conventional gas- tric adenocarcinoma (7). The incidence of this tumor is less com- mon than the conventional gastric adenocarcinoma. However,
this lesion reportedly constitutes 7% to 16% of all gastric adeno- carcinomas (8, 9).
Sporadic reports have described several characteristics of LELC. Most of these studies evaluated the clinicopathologic fea- tures of LELC (7, 10). However, to date, there have been few studies about the computed tomography (CT) features of EBV- associated LELC (11). The purpose of this study was to analyze the clinical and radiological features of EBV-associated LELC and to determine which CT features are seen more often in EBV- associated LELC.
MATERIALS AND METHODS
Population
This retrospective study was approved by our Institutional Re- view Board, which waived the requirement to obtain informed consent. Between January 2004 and September 2014, EBV in
J Korean Soc Radiol 2015;72(1):20-28 http://dx.doi.org/10.3348/jksr.2015.72.1.20
Received July 29, 2014; Accepted October 11, 2014 Corresponding author: Young Chul Kim, MD Department of Radiology, Ajou University School of Medicine, 164 World cup-ro, Yeongtong-gu, Suwon 443-380, Korea.
Tel. 82-31-219-5852 Fax. 82-31-219-5862 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Purpose: To analyze the computed tomography (CT) features of Epstein-Barr virus (EBV)-associated lymphoepithelioma-like carcinoma (LELC).
Materials and Methods: Between January 2004 and September 2014, radiologic fea- tures of 44 EBV-associated LELCs were analyzed. Lesion detectability, multiplicity, loca- tion, gross appearance, lesion thickness and margin, presence of a round edge, contrast enhancement pattern, and the degree of contrast enhancement were analyzed.
Results: The most common location of LELC was the upper third of the stomach (n = 28; 63.64%). A high percentage of cases showed uniform peripheral thickness (n = 32;
88.89%). LELCs demonstrated well-defined margins in a high percentage of cases (n
= 31; 86.11%). Additionally, a high percentage of cases showed the presence of a round edge (n = 28; 77.78%).
Conclusion: CT features, including tumor location in the upper third of the stom- ach and presence of uniform peripheral thickness with a round edge, may suggest the possibility of EBV-associated LELC.
Imaging Findings of Epstein-Barr Virus-Associated Gastric Lymphoepithelioma-Like Carcinoma
1엡스타인-바 바이러스 연관 림프상피종 유사 암종의 영상 소견1
Tae Sun Han, MD
1, Young Chul Kim, MD
1, Yong En Chung, MD
2, Dakeun Lee, MD
3, Mee Jin Park, MD
1, Jei Hee Lee, MD
1, Jai Keun Kim, MD
1Departments of 1Radiology, 3Pathology, Ajou University School of Medicine, Suwon, Korea
2Department of Radiology, Yonsei University College of Medicine, Seoul, Korea
and arterial phase enhanced CTs, the scanning range was from the xyphoid process to the level including the whole stomach.
CT scanning parameters were as follows: for 16 detector rows, a beam collimation of 1.5 × 16 mm, a pitch of 0.938, kVp/mA 120/300, and a gantry rotation time of 0.75 seconds; for 64 detec- tor rows, a beam collimation of 0.625 × 64 mm, a pitch of 0.891, kVp/mA 120/300, and a gantry rotation time of 0.75 seconds;
and for 128 detector rows, a beam collimation of 0.6 × 128 mm, a pitch of 0.6, kVp/mA 120/300, and a gantry rotation time of 0.5 seconds. Isotropic raw data was acquired with a slice thickness of 1 mm and an interval of 1 mm using MDCT. Using these raw data, transverse images were obtained with a slice thickness of 5 mm and an interval of 5 mm; the coronal maximum intensity projection (MIP) images were reconstructed on a workstation with arterial phase contrast CT scans, and coronal and sagittal multiplanar reformation (MPR) images were reconstructed on the workstation with portal venous phase contrast CT scans.
Each MIP image was obtained at a 30 mm interval with a slice thickness of 3 mm, and each MPR image was obtained at a 3 mm interval with a slice thickness of 3 mm.
Imaging Analysis
All CT images were analyzed retrospectively by two radiologists in consensus (with 7 and 12 years of experience, respectively). The qualities of all CT images were adequate for image analysis with- out artifacts that could hinder correct image evaluation. The re- viewers evaluated tumor detectability on CT images with the aid of two-dimensional reformatted images (coronal and sagittal).
Second, the number of tumors was recorded to evaluate multi- plicity (single or multiple). Third, the following items were ana- lyzed: tumor location, long diameter of tumor, gross appearance, tumor thickness, tumor margin, presence of round edge, con- trast enhancement pattern, and degree of contrast enhancement (12). The location of lesions was classified as upper, middle, or lower third of the stomach. The long diameter was measured in mm with an electronic caliper on CT images. The gross appear- ance of each mass lesion was categorized as 1) polypoid, defined as an intraluminal growing mass; 2) fungating, defined as a lesion with a focal wall thickening of more than 1 cm, with or without a depressed area; 3) ulcerated, defined as a depressed lesion with a wall thickening of less than 1 cm; or 4) diffusely infiltrative, de- fined as a lesion involving more than 50% of the entire stomach situ hybridization (ISH) tests were performed on surgical speci-
mens of 123 gastric carcinoma patients, many of which showed variable lymphocytic infiltration, which may suggest the possi- bility of LELC. Eighty-four patient specimens that demonstrated EBV positivity on the EBV-ISH test were initially included as EBV-associated LELC. Of these specimens, 40 were excluded from analysis because they showed pathologic features of conven- tional gastric adenocarcinoma, neuroendocrine tumor, or signet- ring cell carcinoma. The surgical specimens of the remaining 44 patients fulfilled the pathologic criterion for LELC with EBV positivity. The tumors in 39 patients that demonstrated EBV neg- ativity on EBV-ISH test were also excluded. A total of 44 pa- tients received esophagogastroduodenoscopy (EGD) before sur- gery or endoscopic submucosal dissection (ESD). The interval between EGD and CT was less than 2 weeks. All patients under- went surgery or ESD. Patients underwent total gastrectomy (n = 21; 47.73%), subtotal gastrectomy (n = 15; 34.09%), proximal gastrectomy (n = 4; 9.09%), or ESD (n = 4; 9.09%).
CT Examination
All patients underwent CT examinations with one of four com- mercially available 16-, 64-, or 128-channel multidetector CT (MDCT) scanners: Somatom Definition flash, Somatom Sensa- tion 16 (Siemens Medical Solutions, Erlangen, Germany), Bril- iance 16, and Briliance 64 (Philips Healthcare, Cleveland, OH, USA), respectively.
All patients fasted for over 6 hours and gave written consent before undergoing the CT scan. They did not receive intrave- nous anticholinergic drugs or glucagon injections beforehand.
Patients underwent CT scanning immediately after drinking 700–1000 mL of pure water for adequate stomach distension, in a routine supine position to avoid artifacts caused by air in the stomach. An unenhanced CT was taken first, and for contrast- enhanced CT, 150 cc of nonionic contrast agent (Ioversol, Opti- ray; Mallinckrodt Pharmaceuticals, Dublin, Ireland) was adminis- trated intravenously at rate of 3 mL/sec using a power injector.
The second CT scan was performed 30 seconds after the admin- istration of the contrast agent to obtain the arterial phase. The third CT scan was performed 90 seconds after the contrast agent was administered to obtain the portal venous phase. The scan- ning ranged from the xyphoid process to the lower end of the symphysis pubis in the portal venous phase; for the unenhanced
edge was confirmed by reviewing hematoxylin and eosin (H&E)- stained slides of surgical specimens. Finally, according to the 7th American Joint Committee on Cancer (AJCC) TNM staging system, the pathological TNM stage was assessed.
Statistical Analyses
Statistic analyses were performed using MedCalc software (MedCalc, Mariakerke, Belgium). Mean values and percentages were calculated for each clinical and imaging finding.
RESULTS
Clinical Characteristics
The mean age of patients with EBV-associated LELC was 58.18 years old (range: 34–82 years old). Male predominance (male to female ratio = 35:9) was seen in patients with EBV-associated LELC. Multiple lesions were detected in only three patients with EBV-associated LELCs. The most common location of EBV-asso- ciated LELC was the upper third of the stomach (n = 28; 63.64%).
According to the 7th AJCC classification, TNM stages of EBV- associated LELCs were T1aN0M0 (n = 1), T1bN0M0 (n = 21), T1bN1M0 (n = 3), T2N0M0 (n = 5), T2N1M0 (n = 2), T2N2M0 (n = 1), T3N0M0 (n = 6), T3N1M0 (n = 1), T3N2M0 (n = 1), T3N3M0 (n = 1), T4aN0M0 (n = 1), and T4aN3M0 (n = 1).
Lymph node metastasis was seen in 10 cases (22.73%) of EBV- associated LELCs. The clinical characteristics of EBV-positive LELC are summarized in Table 1.
Radiologic Findings
Detectability of the tumors was 81.82% (n = 36) in EBV-asso- ciated LELCs. Eight cases of EBV-associated LELCs were not detected on CT scans. The long diameters of EBV-associated LELCs ranged from 6 mm to 90 mm (mean, 25.83 mm).
Fungating lesions were the most common type of gross ap- pearance; 24 patients (66.67%) presented with them (Fig. 2).
The second most common type was ulcerative lesion, which was seen in 9 patients (25%) (Fig. 3). The polypoid appearance was demonstrated in two cases of 44 EBV-associated LELCs (Fig. 4).
The infiltrative lesion was the least common type of gross ap- pearance, as only one patient showed that type (2.78%).
A high percentage of cases showed the presence of uniform pe- ripheral thickness in EBV-associated LELCs; 32 patients (88.89%).
wall (13). As another morphologic criterion, the peripheral thick- ness of the mass was recorded as uniform or variable (14). When the periphery of a mass had a uniform thickness of within 10%
along the horizontal cross-section in CT scans, the peripheral thickness of tumor was considered as uniform (Fig. 1). When a tumor had a well-defined margin, the reviewers recorded pres- ence or absence of a round edge on the CT scans. The tumor loca- tion, multiplicity, long diameter of tumor, gross appearance, the presence of uniform peripheral thickness, and well-defined mar- gin were correlated with histologic specimens that were con- firmed by a pathologist. The contrast enhancements of the tumors were classified as of a homogenous or heterogeneous pattern. The degree of enhancement was classified as high enhancement (tu- mor attenuation was higher than that of adjacent normal gastric mucosa), moderate enhancement (tumor attenuation was com- parable with that of gastric mucosa), and low enhancement (tu- mor attenuation was lower than that of gastric mucosa) (15).
Reference Standard
All surgical specimens were evaluated by one experienced pa- thologist (12 years of experience). The criteria of EBV-associat- ed LELC were defined as follows: 1) well-defined tumor margin, 2) dense lymphocytic infiltration of a degree whereby tumor in- filtrating lymphocytes outnumbered the tumor cells, 3) syncytial growth pattern and/or poorly formed glandular structures, and 4) presence of EBV in gastric tumor cells as determined by EBV- encoded RNA (EBER) in situ hybridization. On the other hand, cases showing scattered lymphocytes with prominent desmo- plasia and only one or two lymphoid aggregates per tissue sec- tion were classified as conventional adenocarcinoma. All these cases were determined to be EBER-negative. Cases that showed both LELC areas and conventional adenocarcinomatous area were excluded in this analysis. The presence or absence of round
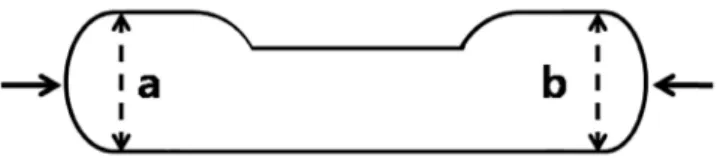
Fig. 1. Technique for peripheral thickness measurement of a mass.
Thickness of a mass was measured at the peripheral portion. When (a) and (b) show less than 10% difference in length, it is defined as posi- tive presence of uniform thickness profile. In addition to uniform thickness profile, round edges (arrows) were seen in the masses re- sembling pizza crust.
EBV-associated LELCs demonstrated well-defined margin (n = 31; 86.11%) in more cases. A high percentage of cases showed the presence of round edge; 28 patients (77.78%).
The most common pattern of contrast enhancement was the homogeneous type as shown in Table 2 (n = 32; 88.89%). Four cases of EBV-associated LELC showed a heterogeneous pattern of contrast enhancement. The most common degree of contrast enhancement was moderate; 25 patients (69.44%). The second most common degree was high; nine patients (25%) with EBV- associated LELCs (Fig. 5). The low degree of contrast enhance- ment were seen in just two patients (5.56%).
DISCUSSION
EBV-associated LELCs developed in male patients (n = 35) more often than in female patients (n = 9). The results support a previous meta-analysis (3): the incidence of EBV-associated LELC was four times higher in males than females but that of conven- tional gastric adenocarcinoma was twice as high in males than in females. The mean age of patients with EBV-associated LELC was 58.18 years old (range: 34–82 years old). To date, the preva- lent age of EBV-associated LELCs are controversial (16, 17). The peak prevalence of conventional adenocarcinoma is known to be between 50 and 70 years old (18). Thus, this may suggest little age difference between the two groups when compared with our study results.
Multiple lesions were detected only in three patients with EBV- associated LELCs. Previous researchers reported that EBV-asso- ciated LELCs tended to be highly associated with multiplicity (9, 16). But, in our study, multiplicity of LELC was seen in only few cases. Lymph node metastasis was also seen in a small percent- age of cases (n = 10; 22.73%). According to previous reports, EBV-associated LELC showed association with significantly lower T stage and lower N stage as compared with conventional adenocarcinoma (19, 20). One study showed 37% (n = 46/123) of N0 cancers in EBV-associated LELC group compared with 6.4% (n = 26/405) of N0 cancers in the conventional gastric car- cinoma group (19).
Detectability of the tumors was 81.82% (n = 36) in our study.
In previous reports, the detection rate of gastric cancer using MDCT ranged from 86.5% to 100% in advanced cases and 32%
to 96.7% in early cases (21-23).
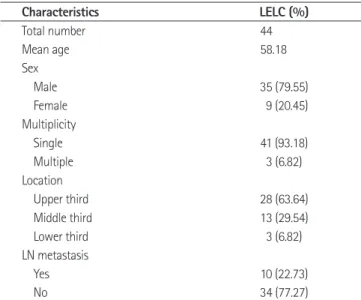
Table 1. Clinical and Pathological Characteristics of Patients with EBV-Associated LELCs
Characteristics LELC (%)
Total number 44
Mean age 58.18
Sex
Male 35 (79.55)
Female 9 (20.45)
Multiplicity
Single 41 (93.18)
Multiple 3 (6.82)
Location
Upper third 28 (63.64)
Middle third 13 (29.54)
Lower third 3 (6.82)
LN metastasis
Yes 10 (22.73)
No 34 (77.27)
Note.-EBV = Epstein-Barr virus, LELC = lymphoepithelioma-like carci- noma, LN = lymph node
Fig. 2. A 58-year-old female with Epstein-Barr virus-associated lym- phoepithelioma-like carcinoma in the stomach. Precontrast (A) and venous phase contrast-enhanced (B) axial CT scans show fungating mass with round edge and moderate enhancement (arrows) in the an- trum of stomach.
A
B
The most common type of gross appearance was the fungat- ing type (n = 24; 66.67%). The second most common type of gross appearance was the ulcerative type (n = 9; 25%). The pol- ypoid appearance was demonstrated only in two of the 44 EBV- associated LELCs. The infiltrative lesion was the least common type of gross appearance. The results of our study support the previous research (11) which found that EBV-associated LELCs In our CT imaging analysis, the most common location of EBV-
associated LELC was the upper third of the stomach (63.64%). The results of our research agree with previous reports that EBV-as- sociated LELCs occur more frequently in the upper third of the stomach (1, 17, 24, 25). As for conventional adenocarcinomas, they were reported to be located more often in either middle or lower third of stomach (19).
Fig. 3. A 63-year-old male with Epstein-Barr virus-associated lymphoepithelioma-like carcinoma in the stomach. Precontrast- (A), arterial phase contrast- (B) and venous phase contrast- (C) enhanced axial CT scans show ulcerative mass with uniform peripheral thickness, round edge and homogeneous enhancement (arrows) in the upper third of stomach. D. Low-power photomicrograph (hematoxylin & eosin stain, × 4) shows well- demarcated mass of lymphoid stroma with uniform thickness and round edge at both sides of tumor. E. High-power photomicrograph (hematoxy- lin & eosin stain, × 40) shows uniformly distributed multifocal nests of poorly differentiated adenocarcinomas in the lymphoid stroma.
Fig. 4. A 54-year-old female with Epstein-Barr virus-associated lymphoepithelioma-like carcinoma in the stomach. A. Esophageal gastroduode- noscopy revealed submucosal mass with mucosal ulcerations in the upper third of stomach. Contrast-enhanced coronal multiplanar reconstruc- tion (B) and contrast-enhanced axial CT scan (C) show small polypoid mass with round edge and low enhancement (arrows).
A
C
A
B
D
B
E
C
lymph node metastasis and better prognosis, differentiation of LELCs from conventional adenocarcinomas may allow tailored therapeutic management in such patients in the future, such as medical treatment with a demethylation agent that may induce lysis of EBV infected cancer cells (7, 18, 20, 29). Understanding show as bulging masses from gastric wall. In one large series, the
percentage of each subtype of conventional advanced gastric carcinoma was polypoid in 4.7%; fungating in 17.7%; ulcerative in 66.6%; and infiltrative in 11% (26). Compared with this pre- vious result, a higher percentage of the fungating type was seen in our LELC study.
A high percentage of cases showed the presence of uniform pe- ripheral thickness of the tumors in EBV-associated LELCs (n = 32; 88.89%). EBV-associated LELCs demonstrated well-defined margins in 31 cases (86.11%). A high percentage of cases showed the presence of round edges in EBV-associated LELCs (n = 28;
77.78%). EBV-associated LELC reportedly demonstrated expan- sive growth of nodules with submucosal invasion in the stom- ach wall (17, 27). Watanabe et al. (4) reported that, at the pe- riphery of the tumor, the lymphoid cells infiltrated the tissue of gastric wall immediately beyond the advancing margin of carci- noma cells. But, as a rule, the margins of the stromal infiltrate as well as that of the tumor cells were sharply delineated against the surrounding stomach wall. In addition, several researchers reported that the tumor cells, which are arranged in sheets or nests, are surrounded by a dense lymphocytic infiltration (4, 17, 28). These pathological features may contribute to the round uniform edges of LELCs.
The uniform peripheral thickness with round edge that was more commonly found in EBV-associated LELCs can be de- scribed as having uniform thickness profile that may resemble a pizza crust edge. Presently, CT features of the LELC are not fa- miliar to clinicians. As EBV-associated LELCs have a low risk of
Fig. 5. A 69-year-old male with Epstein-Barr virus-associated lymphoepithelioma-like carcinoma in the stomach. Arterial phase (A) and venous phase (B) contrast-enhanced axial CT scans show fungating mass with round edge, uniform peripheral thickness, and high enhancement (ar- rows) in the lower third of stomach. C. Low-power photomicrograph (hematoxylin & eosin stain, × 4) shows well-demarcated mass of lymphoid stroma. The mass shows uniform peripheral thickness with round well-demarcated edge. Reactive lymphoid follicles (open arrows) are scattered between tumor nests with dense lymphocytic infiltration.
A B C
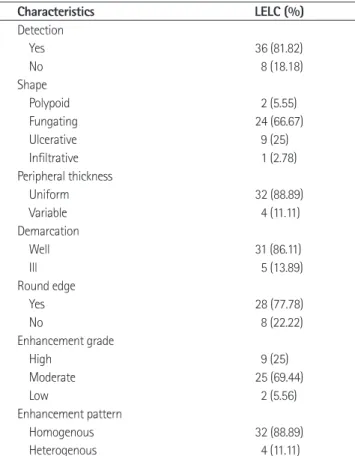
Table 2. CT Features of EBV-Associated LELCs
Characteristics LELC (%)
Detection
Yes 36 (81.82)
No 8 (18.18)
Shape
Polypoid 2 (5.55)
Fungating 24 (66.67)
Ulcerative 9 (25)
Infiltrative 1 (2.78)
Peripheral thickness
Uniform 32 (88.89)
Variable 4 (11.11)
Demarcation
Well 31 (86.11)
Ill 5 (13.89)
Round edge
Yes 28 (77.78)
No 8 (22.22)
Enhancement grade
High 9 (25)
Moderate 25 (69.44)
Low 2 (5.56)
Enhancement pattern
Homogenous 32 (88.89)
Heterogenous 4 (11.11)
Note.-EBV = Epstein-Barr virus, LELC = lymphoepithelioma-like carci- noma
to lymphoepithelial type of gastric carcinoma among vari- ous epithelial neoplasms. J Med Virol 2001;64:513-518 2. Selves J, Bibeau F, Brousset P, Meggetto F, Mazerolles C,
Voigt JJ, et al. Epstein-Barr virus latent and replicative gene expression in gastric carcinoma. Histopathology 1996;28:
121-127
3. Murphy G, Pfeiffer R, Camargo MC, Rabkin CS. Meta- analysis shows that prevalence of Epstein-Barr virus-posi- tive gastric cancer differs based on sex and anatomic lo- cation. Gastroenterology 2009;137:824-833
4. Watanabe H, Enjoji M, Imai T. Gastric carcinoma with lym- phoid stroma. Its morphologic characteristics and prognos- tic correlations. Cancer 1976;38:232-243
5. Ushiku T, Shinozaki A, Uozaki H, Iwasaki Y, Tateishi Y, Funata N, et al. Gastric carcinoma with osteoclast-like giant cells.
Lymphoepithelioma-like carcinoma with Epstein-Barr virus infection is the predominant type. Pathol Int 2010;60:551- 558
6. Torlakovic G, Snover DC, Torlakovic E. Simultaneous EBV- positive lymphoepithelioma-like carcinoma and EBV-neg- ative intestinal-type adenocarcinoma in a patient with Helicobacter pylori-associated chronic gastritis. Am J Clin Pathol 2004;121:237-243
7. Herath CH, Chetty R. Epstein-Barr virus-associated lym- phoepithelioma-like gastric carcinoma. Arch Pathol Lab Med 2008;132:706-709
8. Shibata D, Weiss LM. Epstein-Barr virus-associated gastric adenocarcinoma. Am J Pathol 1992;140:769-774
9. Fukayama M, Chong JM, Uozaki H. Pathology and molecu- lar pathology of Epstein-Barr virus-associated gastric car- cinoma. Curr Top Microbiol Immunol 2001;258:91-102 10. Wang HH, Wu MS, Shun CT, Wang HP, Lin CC, Lin JT. Lym-
phoepithelioma-like carcinoma of the stomach: a subset of gastric carcinoma with distinct clinicopathological fea- tures and high prevalence of Epstein-Barr virus infection.
Hepatogastroenterology 1999;46:1214-1219
11. Maeda E, Akahane M, Uozaki H, Kato N, Hayashi N, Fu- kayama M, et al. CT appearance of Epstein-Barr virus-as- sociated gastric carcinoma. Abdom Imaging 2009;34:618- 625
12. Kim JY, Lee JM, Kim KW, Park HS, Choi JY, Kim SH, et al.
Ectopic pancreas: CT findings with emphasis on differenti- the imaging findings of EBV-associated gastric carcinoma is im-
portant in differentiating it from other tumors, such as submu- cosal tumor and poorly differentiated adenocarcinoma (30). In a case where the pathological features are similar to poorly dif- ferentiated conventional adenocarcinoma, specific imaging fea- tures of EBV-associated LELC can help clinicians to decide whether additional tests such as EBV-ISH are necessary (19). A recent study (19) including 123 EBV-associated gastric carcino- ma cases showed that 18 (14.6%) cases had histologic features that were pathologically indistinguishable from conventional adenocarcinoma in terms of H&E staining.
The most common pattern of contrast enhancement was the homogeneous type (n = 32; 88.89%) and the most common de- gree of contrast enhancement was moderate (n = 25; 69.44%).
Park et al. (13) reported that the most common enhancement pattern and grade of conventional gastric adenocarcinoma were a homogenous pattern and high enhancement grade. However, to date, there is no report about the patterns and grade of EBV- associated LELCs.
There are some limitations in our study. First, our study was a retrospective study, which could have inherent selection bias.
Second, our study involves a small sample size because there were a few patients who had undergone EBV-ISH tests. LELC constitutes a small percentage of all gastric adenocarcinomas and EBV-ISH tests were performed selectively by pathologists when EBV-associated gastric carcinoma was pathologically sus- pected. Widely available and relatively accurate EBV-ISH (8) was used as a standard value and untested cases were not in- cluded as some EBV-associated gastric carcinomas may show similar pathologic features as conventional adenocarcinomas (19). To avoid bias in our study, EBV-ISH negative LELCs and EBV-positive conventional adenocarcinomas were excluded.
In conclusion, when a patient shows radiologic features, in- cluding a tumor location in the upper third of the stomach, and presence of a uniform thickness profile of the mass with a round edge resembling a pizza crust, such features may suggest the possibility of EBV-associated LELC.
REFERENCES
1. Kijima Y, Hokita S, Takao S, Baba M, Natsugoe S, Yoshinaka H, et al. Epstein-Barr virus involvement is mainly restricted
al. Preoperative staging of gastric cancer by endoscopic ultrasonography and multidetector-row computed to- mography. J Gastroenterol Hepatol 2010;25:512-518 23. Bhandari S, Shim CS, Kim JH, Jung IS, Cho JY, Lee JS, et al.
Usefulness of three-dimensional, multidetector row CT (virtual gastroscopy and multiplanar reconstruction) in the evaluation of gastric cancer: a comparison with con- ventional endoscopy, EUS, and histopathology. Gastroin- test Endosc 2004;59:619-626
24. Yanai H, Nishikawa J, Mizugaki Y, Shimizu N, Takada K, Matsusaki K, et al. Endoscopic and pathologic features of Epstein-Barr virus-associated gastric carcinoma. Gastroin- test Endosc 1997;45:236-242
25. Wu MS, Shun CT, Wu CC, Hsu TY, Lin MT, Chang MC, et al.
Epstein-Barr virus-associated gastric carcinomas: relation to H. pylori infection and genetic alterations. Gastroenter- ology 2000;118:1031-1038
26. Kim DY, Kim HR, Kim YJ, Kim S. Clinicopathological fea- tures of patients with Borrmann type IV gastric carcinoma.
ANZ J Surg 2002;72:739-742
27. Nishikawa J, Yanai H, Mizugaki Y, Takada K, Tada M, Okita K. Case report: hypoechoic submucosal nodules: a sign of Epstein-Barr virus-associated early gastric cancer. J Gas- troenterol Hepatol 1998;13:585-590
28. Iezzoni JC, Gaffey MJ, Weiss LM. The role of Epstein-Barr virus in lymphoepithelioma-like carcinomas. Am J Clin Pathol 1995;103:308-315
29. Feng WH, Hong G, Delecluse HJ, Kenney SC. Lytic induc- tion therapy for Epstein-Barr virus-positive B-cell lym- phomas. J Virol 2004;78:1893-1902
30. Kim SW, Shin HC, Kim IY, Kim CJ, Lee JH, Lee CK, et al. Ep- stein-Barr virus-associated lymphoepithelioma-like gastric carcinoma presenting as a submucosal mass: CT findings with pathologic correlation. Korean J Radiol 2010;11:697- 700
ation from small gastrointestinal stromal tumor and leio- myoma. Radiology 2009;252:92-100
13. Park MS, Yu JS, Kim MJ, Yoon SW, Kim SH, Noh TW, et al.
Mucinous versus nonmucinous gastric carcinoma: differ- entiation with helical CT. Radiology 2002;223:540-546 14. Balthazar EJ. CT of the gastrointestinal tract: principles
and interpretation. AJR Am J Roentgenol 1991;156:23-32 15. Hur BY, Kim SH, Choi JY, Rha SE, Lee MW, Kim SY, et al. Gas-
troduodenal glomus tumors: differentiation from other subepithelial lesions based on dynamic contrast-enhanced CT findings. AJR Am J Roentgenol 2011;197:1351-1359 16. Tokunaga M, Land CE, Uemura Y, Tokudome T, Tanaka S,
Sato E. Epstein-Barr virus in gastric carcinoma. Am J Pathol 1993;143:1250-1254
17. Uozaki H, Fukayama M. Epstein-Barr virus and gastric car- cinoma--viral carcinogenesis through epigenetic mecha- nisms. Int J Clin Exp Pathol 2008;1:198-216
18. Kim JH, Eun HW, Goo DE, Shim CS, Auh YH. Imaging of various gastric lesions with 2D MPR and CT gastrography performed with multidetector CT. Radiographics 2006;26:
1101-1116; discussion 1117-1118
19. Song HJ, Srivastava A, Lee J, Kim YS, Kim KM, Ki Kang W, et al. Host inflammatory response predicts survival of pa- tients with Epstein-Barr virus-associated gastric carcino- ma. Gastroenterology 2010;139:84-92
20. van Beek J, zur Hausen A, Klein Kranenbarg E, van de Vel- de CJ, Middeldorp JM, van den Brule AJ, et al. EBV-positive gastric adenocarcinomas: a distinct clinicopathologic en- tity with a low frequency of lymph node involvement. J Clin Oncol 2004;22:664-670
21. Moschetta M, Stabile Ianora AA, Anglani A, Marzullo A, Scardapane A, Angelelli G. Preoperative T staging of gas- tric carcinoma obtained by MDCT vessel probe reconstruc- tions and correlations with histological findings. Eur Radi- ol 2010;20:138-145
22. Hwang SW, Lee DH, Lee SH, Park YS, Hwang JH, Kim JW, et
엡스타인-바 바이러스 연관 림프상피종 유사 암종의 영상 소견1
한태선
1· 김영철
1· 정용은
2· 이다근
3· 박미진
1· 이제희
1· 김재근
1목적: 엡스타인-바 바이러스 연관 림프상피종 유사 암종(lymphoepithelioma-like carcinoma; 이하 LELC)의 전산화단층 촬영(CT) 소견을 분석하고자 하였다.
대상과 방법: 2004년 1월부터 2014년 9월 사이에 44개의 LELC의 영상 소견을 분석하였다. LELC의 병변 검출감도, 다 원성, 위치, 육안적 형태, 병변 두께와 변연, 원형모양 가장자리의 존재, 조영증강 패턴 및 조영증강 정도를 분석하였다.
결과: 가장 흔한 LELC의 위치는 위상부 3분의 1이었다(n = 28; 63.64%). 높은 퍼센트의 균일한 외면 두께의 존재가 보였다(n = 32; 88.89%). LELC에서 경계가 좋은 변연(n = 31; 86.11%)을 높은 퍼센트에서 보였다. 원형모양 가장자리 의 존재는 LECL 환자(n = 28; 77.78%)의 높은 퍼센트에서 보였다.
결론: 종양의 위치가 위상부 3분의 1에 위치하며 균일한 외면 두께의 존재와 함께 원형모양 가장자리가 있는 CT 소견을 보이는 경우 엡스타인-바 바이러스 연관 LELC의 가능성을 제시하는 데 도움을 줄 수 있다.
아주대학교 의과대학 1영상의학과, 3병리과, 2연세대학교 의과대학 영상의학과