Received: 26 March 2011, Accepted: 12 July 2011 Corresponding author: Ji Hye Suk
Department of Internal Medicine, Maryknoll Medical Center, 12 Daecheong-dong 4-ga, Jung-gu, Busan 600-730, Korea
Tel: +82-51-461-2693, Fax: +82-51-465-7470, E-mail: Jihyesuk@gmail.com
Ophthalmopathy Induced by Bilateral Carotid Cavernous Fistula in a Patient with Graves’ Disease
Jong Kun Ha, Ji Hye Suk, A Ra Jo, Chan Woo Jung, Bong Jae Kim, Seong Oh Park, Sang Su Kim1, Mi Kyung Kim Departments of Internal Medicine and Ophthalmology1, Maryknoll Medical Center, Busan, Korea
Graves’ disease (GD) can lead to specific eye afflictions including proptosis, periorbital swelling, conjunctival injection, chemosis, and opthalmoplegia, which then become a condition called Graves’ ophthalmopathy or thyroid-associated ophthalmopathy (TAO). A carotid cavernous fistula (CCF) is an abnormal vascular communication between the carotid artery and the cavernous sinus. The clinical signs of CCF are very similar to TAO and should be considered as a differential diagnosis of TAO. We would like to present an interesting case of a bilateral ophthalmopathy induced by CCF in a GD patient. A 54-year-old man with a 6-year his- tory of GD presented with bilateral exophthalmos and conjunctival injection for two months. The orbital CT scan findings were consistent with CCF, and an angiography revealed bilateral CCF. He received a bilateral coil embolization for the CCF and his oph- thalmic signs were immediately improved. We recommend orbital imaging to exclude other coexisting diseases in patients who are suspected of TAO, especially when the diagnosis is uncertain or when determining whether medical or surgical intervention is appropriate. (Endocrinol Metab 26:335-339, 2011)
Key Words: Carotid cavernous fistula, Graves’ disease, Ophthalmopathy
서 론
그레이브스안구병증또는 갑상선안구병증(thyroid-associated opthalmopathy, TAO)은그레이브스병(Graves’ disease, GD)의대표 적인갑상선외이상으로안구돌출, 결막충혈, 안검및눈주위부
종, 눈근육마비등을일으킬수있다[1,2]. TAO는주로자가면역기
전에의한섬유아세포의활동성증가로의해외안근과안와의결합 조직에글리코사미노글리칸과수분이축적되어발생한주위결합 조직의부종과비후가원인이다[2].
경동맥-해면정맥동루(carotid cavernous fistula, CCF)는경동맥과 해면정맥동사이에비정상적인연결이존재하는것으로안구돌출, 결막충혈, 안검및눈주위부종, 안압상승, 복시등의 TAO와비슷
한증상및소견이발생할수있다[3]. CCF는직접형과간접형으로
나뉜다. 직접형은흔히외상에의해유발되며뚜렷한안구증상및 소견을보이며, 간접형은비외상성이며비교적드물고고혈압, 동맥 경화등의기타신체적이상과도연관이있는것으로알려져있으며
다양한양상을보인다[4].
저자들은 GD 환자에서양측성 CCF로인한양측성안구병증을 보인증례를경험하였다. 특히, 방사선학적검사가안구병증의감별 진단에유용하다는것을확인하였기에문헌고찰과함께보고하고 자한다.
증 례
환자: 54세, 남자
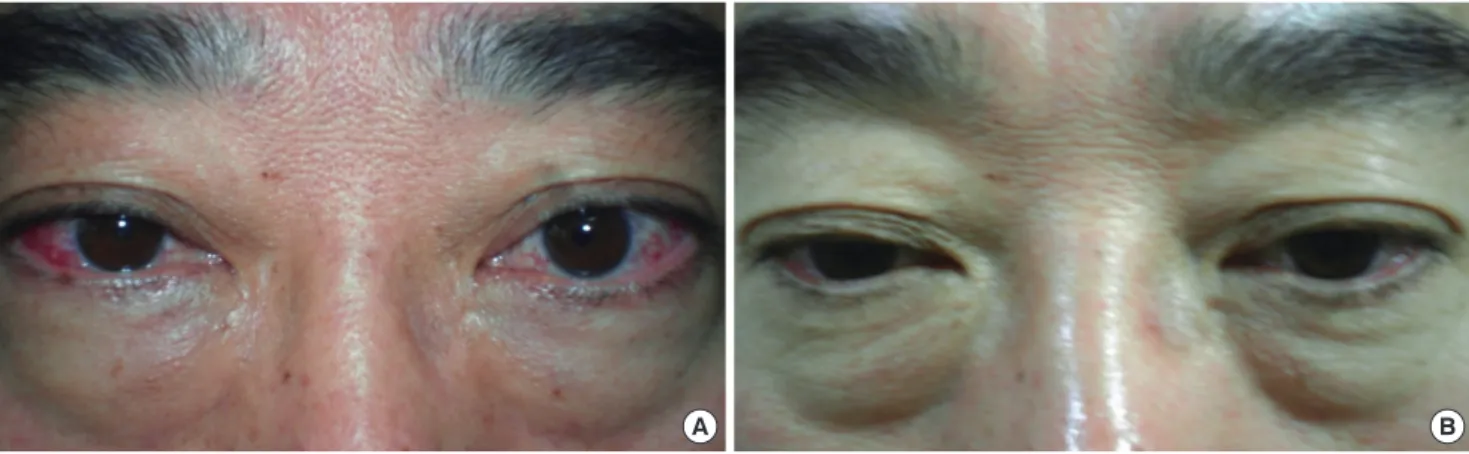
주소:양측안구돌출, 안검부종, 결막충혈(Fig. 1A)
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2011 Korean Endocrine Society
현병력:내원 6년전 GD를진단받았으나불규칙하게항갑상선제 를복용하던중 3개월전갑상선항진증이재발하여항갑상선제를 복용하기 시작하였고내원 2개월전부터양측안구돌출, 안검부 종, 결막충혈등의증상이발생하였다. 개인병원에서 TAO가의심된 다는이야기를듣고치료를받았으며, 내원당시프로필티오우라실 75 mg 하루 2회와덱사메타손 0.75 mg 하루 1회를복용하고있었 다. 환자는임상적호전이없어본원내분비내과외래를방문하였고 정밀검사를위해입원하였다.
과거력 및 가족력: 9년전좌안의백내장으로수술한병력이있었 으며안구의외상병력은없었다.
사회력:약 20갑년의흡연력이있었으나 10년전금연하였으며, 주 1회소주 1병정도의음주력이있었다.
신체 진찰 소견:입원당시혈압 120/80 mmHg, 맥박수 68회/분, 호흡수 12회/분, 체온 36.4°C이었으며신장 165 cm, 체중 74 kg으로 체질량지수 27.18 kg/m2이었다. 전신상태는양호하였고양측의안구 돌출, 안검부종, 결막충혈을보이고있었으며, 시력저하의소견은 관찰되지않았다.
검사실 소견:입원후시행한혈액검사에서백혈구 8,900/mm3, 혈 색소 16.3 mg/dL, 헤마토크리트 46.2%, 혈소판 192,000/mm3이었다. 전해질검사에서나트륨 139 mEq/L, 칼륨 3.8 mEq/L의소견보였으 며, 생화학검사에서 AST 26 IU/L, ALT 47 IU/L, 총단백질 7.2 mg/dL,
알부민 4.5 mg/dL의결과관찰되었다. 내원당시한달간항갑상선제
를복용하고있는상태였으며, 본원에서시행한갑상선기능검사에서 총 T3 92 ng/dL (정상범위, 58-157), 유리 T4 0.92 ng/dL (정상범위, 0.71-1.85), TSH 5.69 mIU/L (정상범위, 0.38-4.70), 갑상선자극호르 몬수용체항체는 0.28 U/L (정상범위, 0-10), 항갑상선과산화효소 항체는 24.5 U/mL (정상범위, 60 미만), 항갑상선글로불린항체는 210.4 IU/mL (정상범위, 60 미만)의결과를보였다. 본원내원 3개월 전방문한 개인병원에서검사한갑상선기능검사는 T3 239 ng/dL, 유리 T4 3.44 ng/dL, TSH < 0.01 μIU/mL이었다.
안과검사 소견:안구돌출계(Hertel exophthalmometer)로측정한
안구의돌출정도는양측 모두 20 mm이었으며, 안압은좌안 31.1
mmHg, 우안 23.4 mmHg (정상범위, 10-21 mmHg)로양측의안압 이상승된소견이관찰되었고, 양안약간의외전장애가관찰되었다. 안저검사, 시야검사에서는특이사항이관찰되지않았다.
방사선검사 소견:입원 2일째시행한안와컴퓨터단층촬영에서외
안근의비후소견은관찰되지않았고, 좌측상안정맥(left superior
ophthalmic vein)의확장과좌측해면정맥동에조영이증강된부분
이관찰되어 CCF가의심되었다(Fig. 2).
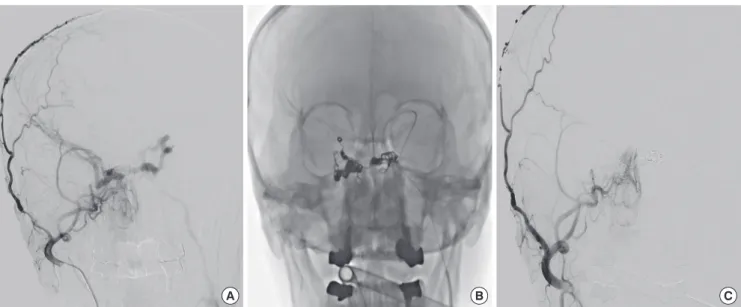
임상 경과: CCF의확진및치료를위해환자를전원하였으며전원 후뇌혈관조영술에서양측 CCF를진단하였고, 코일을이용한색전 술을통해동정맥루를성공적으로차단하였다(Fig. 3). 뇌혈관조영 술에서양측모두내, 외경동맥의경막분지와교통하고있었다. 환 자는색전술시행 2주후본원외래를방문하였으며당시결막충혈 은소실되고안검부종도호전되었다(Fig. 1B). 색전술 3개월후에시 행한안과검사에서양안의안구돌출정도는양안모두 18 mm 정 도로약간의호전을보였으며, 양안의운동기능은정상으로호전되 었다. 안압은좌안 30.2 mmHg, 우안 21.5 mmHg로미약한호전을 보이고있다. 현재 GD에대해서메티마졸 2.5 mg을하루 1회투여 하면서추적관찰중이다.
고 찰
GD 환자에서임상적 TAO는 30-50% 정도에서나타나지만시력이
위험할정도로심한안구병증은 3-5%에서발생한다[1,2]. 임상적으로 나타나지않는경우도많아안와영상검사를시행하면거의 70%에
서외안근침범이나타나는것으로보고되어있다[5]. 그러나, 동양
인에서는서양인에비해드물고정도도경한것으로알려져있다[6].
TAO의흔한임상양상으로는상안검퇴축, 안구돌출, 결막충혈, 안 검및눈주위부종, 복시등이있고, 증상은대개양측성으로나타
A B
Fig. 1. Ocular manifestations of the patient. A. Before embolization treatment, the patient presented bilateral proptosis, periorbital edema, conjunctival injection and chemosis. B. After embolization treatment, conjunctival injection and chemosis disappeared, bilateral proptosis was improved.
나며, 일측성인경우는 5-15%이다[1,2]. TAO를보이는환자에서안 와컴퓨터단층촬영을시행하였을때 30%에서외안근비후가비대 칭성을보여, 임상적으로일측성인경우에도상당수에서비대칭적 인양측성안구병증이다[7]. TAO는대부분양측성으로나타나지만, 일측성으로나타나거나양측성비대칭성으로나타날수있으며이 런경우에는 TAO가의심되더라도안와종양, CCF, 해면정맥혈전증 등유사한임상양상을유발할수있는다른질환이동반되어있는
지감별진단이필요하다[1].
CCF는경동맥과해면정맥동사이의비정상적인교통이존재하는 것으로, 해부학적인구조에따라직접형과간접형으로구분할수있
다[4]. 직접형 CCF는경동맥과해면정맥루사이에직접적인누공이
존재하는것으로대개외상이나두부수술의부작용등에의해발
생하며 CCF의대부분을차지한다[4]. 간접형 CCF는동정맥루가경
동맥의경막동맥분지와해면정맥동사이에발생하는것으로혈류의
A B C
Fig. 3. Cerebral angiography. A. Before embolization treatment, anteroposterial projection, demonstrating the supply to the bilateral carotid cavernous fistula from both branches of external carotid artery and meningeal branches of internal carotid artery. B. Embolization was performed with venous approach at both cavernous sinuses and intercavernous sinus. C. After embolization treatment, anteroposterial projection, showing complete occlusion of bilateral carotid cavernous fistula.
Fig. 2. Before embolization treatment. Orbital computed tomography revealed dilated left superior ophthalmic vein (white arrow, A) and dilated left cavernous sinus (Black arrow, B).
A B
있다[4]. 간접형 CCF는비교적드문질환으로발병기전은정확히알 려져있지않으나대개중년의여성에서발생하며고혈압, 동맥경화, 결체조직질환, 혈관질환, 기타다른신체적이상과연관이있는것으 로알려져있다[4].
CCF에서안구증상은해면정맥동으로부터상안정맥으로의역류 성혈류에의한안정맥의고혈압으로인해발생하며안구돌출, 안검 부종, 결막충혈, 눈부심, 안구운동장애, 복시, 시력저하등의증상
을유발할수있다[3]. 그외안압이상승할수있으며, 안와에서잡
음이들릴수있다[3]. CCF는종종결막염, 녹내장, TAO로오진되며, 진단이지연되는경우폐쇄각녹내장, 망막중심정맥폐쇄, 증식성망
막증 등의 심각한합병증이 발생하여시력을 상실할 수있다[8].
CCF는대개편측으로나타나나드물게양측으로나타나거나공급
혈관의반대측에나타나는경우도있다[9].
TAO에동반된일측안구병증을유발한 CCF가각각국외[9]와국 내[10]에서한사례씩보고되었다. 국외보고에서는 GD로진단받고 10년간항갑상선제치료를받던 67세의여자환자가양측의안검부 종, 안구돌출, 결막충혈, 복시가있어수개월동안고용량스테로이 드치료를받았으며, 치료이후좌안의안구증상은호전되었는데 반해, 우안의안구증상이호전되지않았다. 안와컴퓨터단층촬영을 시행하여우안의 CCF를발견하고색전술을시행받고안구병증이 호전되었다[9]. 국내보고는 GD로진단받고 8개월간치료받던 26세 여자환자가우안의돌출, 복시, 안검퇴축, 안검지체가발생하여안 와자기공명촬영에서 CCF가의심되었다. 뇌혈관조영술을시행하여 우측 CCF를확진하고색전술을시행한후안구병증이호전되었다[10].
국외의보고는 TAO와일측성 CCF가동시에발생한경우로생각되 며국내의보고는일측성 CCF가단독으로발생한것으로보인다.
본증례는 6년전 GD로진단받고불규칙하게항갑상선제를투약 하던환자가양측성의안구돌출과안검부종, 결막충혈을호소하 며내원하여 TAO가우선적으로의심되어소량의스테로이드치료 를받았으나임상적호전이없어시행한안와컴퓨터단층촬영에서 양안의외안근및주위결합조직의비후는두드러지게관찰되지않 았으며, 좌측상안정맥이확장되고좌측해면정맥동의확장및조
영증강된소견이관찰되어 TAO 동반없는 CCF가의심되었다. 뇌혈
관조영술을통하여양측성 CCF로확진되고색전술을시행받은후 안구돌출과결막충혈소견이호전되었다. 즉, GD 환자가 TAO 없이 양측성 CCF에의한양측성안구병증을보였다. 비외상성의양측성
CCF는드물게발생하며[11,12], GD와동반되어나타난경우는아직
까지국내외에서보고된바가없다. GD에서양측성안구병증이있
을때 TAO를가장먼저의심할수있으나, TAO와동반하여또는
동반없이다른질환이병발하여안구병증을유발혹은악화시킬
할가능성이있는경우는정확한감별진단을위해안와영상검사 를시행해야할것으로생각한다.
요 약
그레이브스병에서는안구돌출, 안구주위부종, 결막의부종및
충혈등의증상으로나타나는 TAO를보일수있다. CCF는경동맥과
해면정맥동사이에비정상적인교통이발생한것으로안구돌출, 안 검부종, 결막충혈등 TAO와비슷한증상을보일수있어특히일 측성이나비대칭적인경우, TAO와감별이필요하다. 저자들은그레 이브스병환자에서양측성 CCF로인한양측성안구병증을보인경 우를경험하여보고하고자한다. 6년간의갑상선항진증의 병력을 가진 54세남자환자로 2개월전부터발생한양측성안구돌출, 결 막충혈로내원하였다. 갑상선안구병증을의심하였으나안와컴퓨 터단층촬영에서 CCF로생각되어뇌혈관촬영으로양측성 CCF로진 단하였으며, 색전술시행후안구병증이호전되었다. TAO가의심되 는환자에서, 특히진단이확실하지않거나내과적및외과적중재 술이필요할가능성이있는경우는정확한감별진단을위해안와 영상검사를시행해야할것으로생각한다.
참고문헌
1. Bartalena L, Tanda ML: Clinical practice. Graves’ ophthalmopathy. N Engl J Med 360:994-1001, 2009
2. Burch HB, Wartofsky L: Graves’ ophthalmopathy: current concepts regard- ing pathogenesis and management. Endocr Rev 14:747-793, 1993 3. Phatouros CC, Meyers PM, Dowd CF, Halbach VV, Malek AM, Higashida
RT: Carotid artery cavernous fistulas. Neurosurg Clin N Am 11:67-84, 2000 4. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT:
Classification and treatment of spontaneous carotid-cavernous sinus fistu- las. J Neurosurg 62:248-256, 1985
5. Kahaly GJ: Imaging in thyroid-associated orbitopathy. Eur J Endocrinol 145:107-118, 2001
6. Tellez M, Cooper J, Edmonds C: Graves’ ophthalmopathy in relation to cigarette smoking and ethnic origin. Clin Endocrinol (Oxf) 36:291-294, 1992
7. Enzmann DR, Donaldson SS, Kriss JP: Appearance of Graves’ disease on orbital computed tomography. J Comput Assist Tomogr 3:815-819, 1979 8. Phelps CD, Thompson HS, Ossoinig KC: The diagnosis and prognosis of
atypical carotid-cavernous fistula (red-eyed shunt syndrome). Am J Oph- thalmol 93:423-436, 1982
9. Loré F, Polito E, Cerase A, Bracco S, Loffredo A, Pichierri P, Talidis F: Carot- id cavernous fistula in a patient with Graves’ ophthalmopathy. J Clin En- docrinol Metab 88:3487-3490, 2003