- 65 -
Introduction
Schwannoma is a benign tumor originated from Schwann cell of the neural sheath. The lesion is characterized by well encapsulated, relatively hard solitary tumor.
1)The pre- operative diagnosis is often difficult because of their non-specific clinical presentation. Generally it is asympto- matic, although the pain and paresthesia may occur. The clinical presentation varies depends on its origin and size.
They are usually diagnosed in the third and fourth decades, with no gender predilection.
2)The lesion can arise from
any cranial, autonomic, peripheral nerve that contains Schwann cells. Approximately 25%-45% of schwannomas occur in the head and neck region, and up to 35% of these involve the oral cavity. They occur most commonly in tongue, followed by the floor of mouth, the palate, the buc- cal mucosa, the gingiva, the lips and the vestibular mucosa.
3)4)We review the literature and report a rare case of a 35-year-old female patient with a schwannoma of the hard palate, which was excised intraorally.
Case report
A 35-year-old woman was referred to our department from local clinic with tumor on the hard palate. The patient visited local clinic 2 weeks ago, when she found a mass on right palate incidentally.
There was no medical history or family history of interest.
Received Re v i se d Accepted
: October 6, 2016 : November 5, 2016 : November 7, 2016
+
Corresponding author: Jae Wook Kim, MD, Department of Otorhinolaryngology-Head & Neck Surgery, Soonchunhyang University College of Medicine, 59, Daesagwan-ro, Yongsan-gu, Seoul 04401, Korea
Tel: +82-2-709-9364 Fax: +82-2-709-9362 E-mail: [email protected]
대한두경부종양학회지, 제32권 제2호, 2016. pp.65-68 Korean Journal of Head & Neck Oncology, Vol.32, No.2
http://dx.doi.org/10.21593/kjhno/2016.32.2.65 ISSN 1229-5183(Print)
A Case of Schwannoma Arising in Hard Palate
Jeong Tae Kim, MD, Jae Wook Kim, MD
+Department of Otolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, Seoul, South Korea
경구개에 발생한 신경초종 1예 및 문헌고찰
김정태·김재욱
+
순천향대학교 의과대학 이비인후과학교실
= Abstract =
신경초종은 천천히 자라는 양성종양으로 뇌신경, 말초신경, 또는 자율신경 등 신경초세포(Schwann cells) 를 포함한 신경 어디에나 발생할 수 있다. 대부분의 신경초종은 무증상이며, 악성화되는 경우는 드물다.
전체 신경초종 중 약 25%에서 45%가 두경부 영역에서 발생하지만 구강 내 발생하는 경우는 거의 없는 것으로 알려져 있다. 구강 내 신경초종의 대부분은 설부에서 발생하며 그 외 발생하는 부위로 협부점막, 구개, 구강저, 잇몸, 입술 등이 있다.
본 저자들은 최근에 경구개에 발생한 신경초종 1예를 경험하였으며, 이를 관련문헌 고찰과 더불어 보고 하는 바이다.
중심 단어:신경초종ㆍ경구개
- 66 - On physical examination, a non-tender, firm mass was pal- pated on right palate area, but no cervical lymph nodes were noted. Other physical examinations were not remarkable, and laboratory test, chest X-ray, electrocardiography, urine analysis were within normal range as well.
On contrast computed tomography, a heterogeneously en- hanced round mass, without any signs of bone destruction on right hard palate was demonstrated (Fig 1). The provi- sional diagnosis was established as a benign soft-tissue neo- plasm, and intraoral excisional biopsy was recommended for confirmation of diagnosis. So we considered additional study such as MRI or surgical biopsy, and planned the con- firmation through surgical resection. After acquiring the op- eration field by mouth gag under general anesthesia, we exposed the mass after making the incision about 2 cm on the middle of the mass (Fig. 2A and B).The neoplasm was circumscribed, well encapsulated, but not infiltrating sur- rounding tissue. We dissected a mass along the margin and enucleated completely (Fig. 2C). Grossly, 2.2 x 1.5 cm sized soft, yellowish tumor with encapsulated surface was ob- served (Fig. 3).
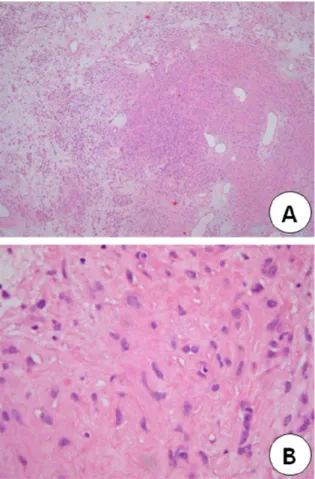
The pathologic features included Antoni A area, com- posed of hypercellular spindle cells in hyalinization matrix, and Antoni B area composed of hypocellular area with ir- regular arrangement of the cells. The final diagnosis of schwannoma was established by immunohistochemical staining revealed positivity for S-100 protein (Fig. 4).
After complete surgical excision, post-operative compli-
Fig. 1. Contrast-enhanced CT shows an about 2.3 x 1.1 cm sized fairly circumscribed heterogeneously enhanced solid mass in the right hard palate.
Fig. 2. The operative findings of the tumor. A: 2.0 x 1.5 cm sized, non-tender, firm tumor in hard palate was identified.
B: The encapsulated tumor was appeared after 2 cm mu- cosal incision. C: The state after tumor enucleation.
Fig. 3. The gross appearance of the tumor. This was a 2.2 x
1.5 cm sized, yellowish soft tissue and the external surface of
the mass was well defined and smooth.
- 67 - cations such as bleeding and wound infection were not not- ed, and recurrence has not been seen.
Discussion
Schwannoma was first described by Verocay in 1910 when he discovered verocay body, a characteristic finding of schwannoma. This tumor is a benign neoplasm originated from neural sheath, which can arise from any cranial nerve, peripheral nerve, and autonomic nerve. Schwannoma is usu- ally found as vestibular schwannoma in central nervous sys- tem, and arises commonly from head, mediastinum, flexion area in extremities in peripheral nervous system.
5)6)When it occurs on head and neck area, usually found in para- pharynx , but rarely in the oral cavity. Generally, there is no gender predilection, and can occur in any age, but most commonly diagnosed in the third and fourth decades of life.
2)The clinical presentation takes months to years, and most- ly found as asymptomatic non-tender lesion. The symptom
varies depending on the location and neural origins of tu- mor, and cough, dyspnea, hoarseness, dysphagia, par- esthesia, pain, anesthesia on affected nerve may occur.
7)In our case, the patient visited clinic with palpable non-tender mass on palate without pain nor paresthesia.
The differential diagnosis of hard palate schwannoma in- cludes hemangioma, hemangiofibroma, epidermal cyst, thy- roglossal duct cyst, lymphangioma, mucocele, benign sali- vary gland tumor, and fibroma.
8)Distinction with neuro- fiboma is most important. Clinically, schwannoma shows efferent nerve distribution within neural sheath.
Transformation to malignant nature is rare, and pain may frequently occur. Neurofibroma can be transform to malig- nant nature in 8-12%, which are mostly asymptomatic.
9)The differential diagnosis can be made by clinical symp- toms, physical examination, radiologic images and fine nee- dle aspiration. The diagnosis is confirmed by pathologic findings.
10)CT scan and MRI can be performed for radio- logic examination. MRI is of greater value than CT on diag- nosing schwannoma with lesser artifacts possibly caused by teeth and well-defined margins of surrounding tissues.
11)Schwannoma in CT can be observed in low density as sur- rounding muscles, and can be enhanced peripherally after enhancing. The schwannoma is demonstrated as low attenu- ation in T1 weighted image and high attenuation in T2 weighted image with partially variant high attenuation.
Histologically, schwannoma is well encapsulated, includ- ing various proportions of Antoni A area and Antoni B area.
Antoni A area consists of nuclei surrounded by cytoplasm, and palisading nucleic bodies called verocay bodies. Antoni B area, on the other hand, has markedly reduced cellularity with degenerative, cystic, inflammatory change.
Furthermore, at immunohistochemical stain, S-100 antigen is expressed in schwannoma.
12)13)The tumor at the hard plate of this report was well-encapsulated, both Antoni A area and Antoni B area could be observed, and intermixed Antoni A and Antoni B area could be seen, thus, can be diagnosed as schwannoma. As for treatment, due to its re- sistance to radiation therapy, surgical resection remains the treatment of choice for removal of schwannoma although observation or gamma-knife is warranted for lesions diffi- cult to approach or eradicate through surgical procedure.
14)Since recurrence is uncommon after complete excision, complete removal of schwannoma with preservation of
Fig. 4. The microscopic findings of the tumor. A:The tumor
shows the pattern of alternating Antoni A (hypercellular)
and B(hypocellular) areas (H-E, x40). B:The tumor cells are
spindle cells that have twisted nuclei and indistinct cyto-
plasmic borders (H-E, x 400).
- 68 - nerve function is recommended.
15)As can be seen, the hard palate schwannoma is charac- terized by less adhesiveness from surrounding tissue, and easy accessibility through intraoral approach, complete re- section within short time without severe complications. The hard palate schwannoma in this case report was completely resected as well, thus, has less potential for recurrence. The case of “Incidentally found hard palate schwannoma” is re- ported with review of literature.
Key Words:SchwannomaㆍHard palate