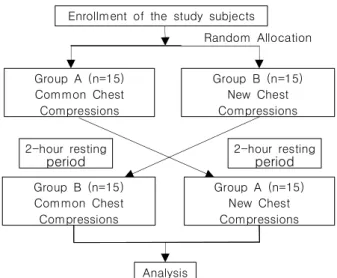
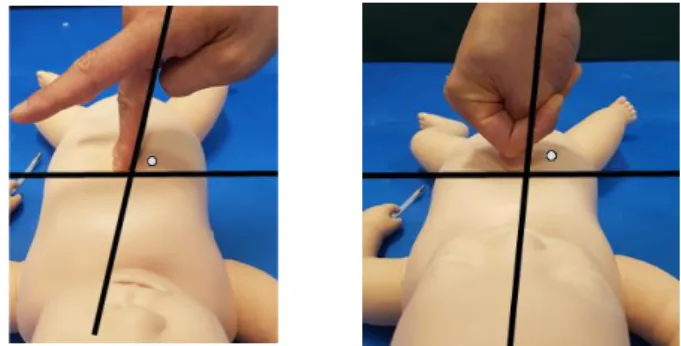
Comparison of New Infant Chest Compression Methods: Simulation Study on Randomization Using Manikin
1)
전체 글
1)
수치
관련 문서
첫째, UTAUT모형을 이용하여 스마트폰 어플리케이션의 구매에 대해 검정한 결과 독립변수들 (성과기대, 예상노력, 사회적 영향, 유희적 가치,
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
This study confirmed that the characteristics of cyberspace, hypermedia and multi-sensory experience of new media in the fourth industrial revolution era can
Third, based on the above results, this study concluded that the competitiveness of the agricultural product distribution industry in uncertain business
Therefore, this study speculated on block building toys that can enhance spatial sense in infants based on the development of creativity and sociability
This dissertation is composed of 6 chapters. ChapterⅠ deals with the purpose and the methods of this study. ChapterⅡ refers the methods and the problems of
That is, the dry powder of the sludge wastes, generated during the decommissioning of nuclear power plants, were compacted, and a study, focused on
From the results of this study, we concluded that two different sized graft materials have positive effects on new bone formation.. Additionally, smaller
