Korean Circulation Journal
Introduction
Heart failure (HF) continues to have a poor prognosis despite the advances in medical treatment.
1)Previous studies suggested sever- al predictors for mortality in HF population. QRS duration is a pre- dictor of poor prognosis in HF.
2)3)Wide QRS duration was found in
Print ISSN 1738-5520 • On-line ISSN 1738-5555
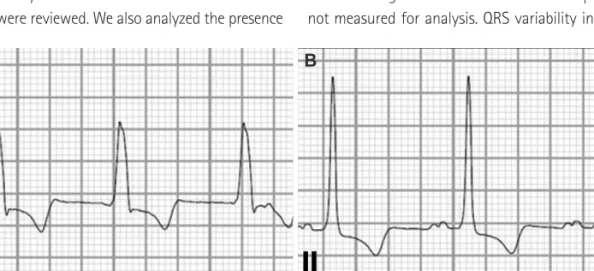
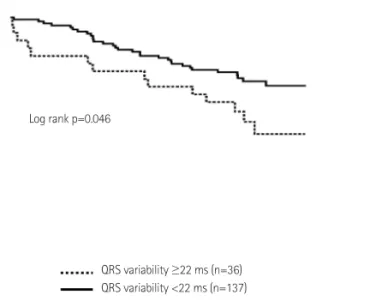
Prognostic Implication of QRS Variability during Hospitalization in Patients with Acute Decompensated Heart Failure
So-Ryoung Lee, MD 1 , Eue-Keun Choi, MD 1 , Do-Yoon Kang, MD 1 , Myung-Jin Cha, MD 1 , Youngjin Cho, MD 1 , Il-Young Oh, MD 2 , and Seil Oh, MD 1
1
Department of Internal Medicine, Seoul National University Hospital, Seoul,
2