Clinical study of keratocystic odontogenic tumors
Nobuyoshi Tomomatsu
1, Narikazu Uzawa
1, Yasuyuki Michi
1, Kazuto Kurohara
1, Norihiko Okada
2, Teruo Amagasa
11
Maxillofacial Surgery, Maxillofacial Reconstruction and Function, Division of Maxillofacial and Neck Reconstruction,
2
Diagnostic Oral Pathology, Oral Restitution, Oral Health Sciences, Graduate School, Tokyo Medical and Dental University
Abstract(J Korean Assoc Oral Maxillofac Surg 2012;38:55-63)
The odontogenic keratocyst (OKC) was originally classified as a developmental cyst, and OKCs were histologically divided into orthokeratotic (O-OKCs) and parakeratotic (P-OKCs) types. Clinical features differ between O-OKCs and P-OKCs with P-OKCs having a tendency to recur after surgical treatment. According to the revised histopathological classification of odontogenic tumors by the World Health Organization (2005) , the term keratocystic odontogenic tumor (KCOT) has been adopted to describe P-OKCs. In this retrospective study, we examined 186 KCOTs treated at the Maxillofacial Surgery Department of the Tokyo Medical and Dental University Hospital from 1981 through 2005. The patients ranged in age from 7 to 85 years (mean, 32.7) and consisted of 93 males and 93 females. The most frequently treated areas were the mandibular molar region and ramus. The majority of KCOTs in the maxillary region were treated by enucleation and primary closure. The majority of KCOTs in the mandibular region were enucleated, and the wound was left open. Marginal resection was performed in the 4 patients with large lesions arising in the mandible. In patients who were followed for more than a year, recurrences were observed in 19 of 120 lesions (15.8%) . The recurrences were found at the margins of the primary lesion in contact with the roots of the teeth or at the upper margins of the mandibular ramus. Clinicians should consider aggressive treatment for KCOTs because the recurrence rate of P-OKCs is higher than that of other cyst types such as O-OKCs, dentigerous cysts, primordial cysts that were non-keratinized, and slightly keratinized stratified squamous epithelium. Although more aggressive treatment is needed for KCOTs as compared to other cystic lesions, it is difficult to make a precise diagnosis preoperatively on the basis of clinical features and X-ray imaging. Therefore, preoperative biopsy is necessary for selecting the appropriate treatment for patients with cystic lesions.
Key words: Keratocystic odontogenic tumor, Odontogenic benign tumor, Odontogenic keratocyst, Odontogenic orthokeratocyst
유전자의관여가인정되는점
,
진행성및재발성의성격을 보유하고있는점,
기저세포모반증후군을동반하여다발 성으로 발생하는경우가있는점7,
치질골을파괴하여주 위 연조직에파급되는점,
기저세포층직상의세포증식활 성이 높은점,
그리고상피이형성을볼수 있다는점등을 들 수 있다1.
지금까지다수의치성각화낭종의재발에 관 한임상적검토가진행되어그원인에대해서도여러견해 가보고되었다.
재발률은12.0%
부터62.5%
로폭넓게보고되고있으며4,817
,
그원인으로낭낭포(daughter cyst),
상피섬(epithelial island)
의존재,
낭종벽표피세포의활발한증식 능등이거론되고있지만,
얇은낭종벽때문에적출시발생 하는상피조직의잔존이원인이라는지적도다수보고되고 있다12,1719.
이에본연구는과거
25
년간본과에서진단하고치료한 단발성의악골낭종을새로운WHO
분류에준하여재분류 한 후,
각화낭성치성종양으로분류된것을대상으로임상 적검토를실시하였다.
I. 제 언
2005
년에치성종양World Health Organization (WHO)
조직분류1가개정되어,
종래의치성각화낭종(odontogenic
keratocyst)
은 낭종상피가착각화를보이는것을 각화낭성치성종양
(keratocystic odontogenic tumor)
으로분류하여양 성종양의 하나로다루게되었다.
치성각화낭종은1956
년Philipsen
2에의해보고된이래,
높은재발률과침윤성등종양으로서의성격이다수보고되었다36
.
종양으로분류된이유로는본병변의발현에암억제유전자의하나인
patched
Nobuyoshi Tomomatsu
Maxillofacial Surgery, Maxillofacial Reconstruction and Function, Division of Maxillofacial and Neck Reconstruction, Graduate School, Tokyo Medical and Dental University, 1-5-45 Yushima Bunkyo-ku, Tokyo 113-8549, Japan TEL: +81-3-5803-5500 FAX: +81-3-5803-0198
E-mail: [email protected]
*Some points of this article was reported at the 51th Japanese Meeting of Oral and Maxillofacial Surgery in Oct, 2006.
*This article was published in Japanese Journal of Oral and Maxillofacial Surgery and secondary publication was permitted each other between Korea and Japan.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
CC
필요가 있었다
.
즉,
각화낭성치성종양은2005
년의분류개 정에의해양성종양으로서다뤄지게되었지만,
이는단지 명칭이바뀐것만이아니라진단기준에도다소변경된부 분이있다.
각화양식이정각화인편평상피로부터이뤄지 는것은이범주에포함하지않으며,
정각화를띠는악골내 낭종을치성정각화낭종(odontogenic orthokeratocyst)
으로 분류하고,
각화낭성치성종양은각화양식이착각화를띠는 것에한정시켰다.
이러한두가지각화양식의차이에따라 임상증상은 달라져,
착각화를띠는것은정각화보다재발II. 연구 대상 및 방법
1981
년부터2005
년까지25
년간동경의과치과대학치학부부속병원악안면외과외래
(
구제1
구강외과)
의임상,
병 리조직학적진료를통해각화낭성치성종양으로진단된단 발186
증례를대상으로하였다.
다발성증례에관해서는이 번해석에서제외하였다.
그러나각화낭성치성종양의진단기준에관해서는신
·
구 분류법에 애매한부분이있어일정한진단기준을적용할Fig. 1. The classification of odontogenic tumors/cyst by World Health Organi- zation (WHO).
Nobuyoshi Tomomatsu et al: Clinical study of kera- tocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Fig. 2. The histopathological classications of odontogenic tumors. A. Parakeratotic type. B. Orthokeratotic type. C. Non-keratotic type (×200, scale bar:100 μm).
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
아이상의병변을대병변으로
,
그보다작은병변을소병변 로분류하여각병변의대소비(
대병변/
소병변)
를비교하였 다.
통계학적분석은2
검정(Yates
의보정)
및Fisher
의직접확률검정을이용하여
P<0.05
를유의한것으로보았다.
III. 결 과 1. 발생빈도 (연령·성비·발생부위)
186
증례의초진시연령은7
세부터85
세까지 분포하고있었고 평균연령은
32.7
세였다.
연령별로는20
대64
증례(34.4%), 10
대35
증례(18.8%), 30
대31
증례(16.7%)
의순으 로나타났다.
성별은남성이93
증례,
여성이93
증례로차이 가 없었다.(Table 1)
발생 부위는상악41
증례,
하악145
증 례로하악구치부로부터하악지에걸쳐발생한것이111
증 례(59.7%)
로가장많았다.(Table 2)
상악의발생부위는 대 구치부가많았다.
2. 임상소견 (증상·X선 소견)
증상으로는종창이
70
증례(37.6%)
로가장 많았고,
동통36
증례(19.4%),
배농18
증례(9.7%),
위화감8
증례(4.3%),
개구장애7
증례(3.8%),
치아의동요1
증례(0.5%)
의순서 였다.
한편 무증상으로X
선 사진에서 발견된것은46
증 례(24.7%)
였다.(Table 3) X
선 소견은 단방성이107
증례 을초래하는경우가많았다20.
그런데이번새로운분류에는치성상피성낭종의조직분류에관한언급은없기때문
에새로운견해가도출될때까지이전
1992
년의조직분류를적용키로한다21
.
애매한종래의치성각화낭종과원시성 낭종,
함치성낭종의진단기준분류에이번새로운분류까 지더할경우,
낭종상피가착각화를띠는것은각화낭성치 성종양으로분류되지만그외정각화를띠는낭종과단발 성으로각화경향이매우경미한낭종의분류는불분명해 진다.
이에본연구에서는아래의기준에준하여분류하였 다1,21.(Figs. 1, 2)
치성각화낭종,
원시성낭종,
함치성낭종중 착각화를띨경우각화낭성치성종양으로,
정각화인경우는 치성정각화낭종으로,
단발성으로각화경향이매우경미하 며매복치를포함하지않는경우는원시성낭종,
매복치를 포함하는것은함치성낭종으로분류하였다.
또한착각화를 띠더라도각화경향이경미한경우는원시성낭종,
함치성 낭종으로분류하였다.
각화양식이혼재하는경우에는보 다명확하게나타나는양식에준하여분류하였다.
치료성적및재발에대해서는
1
년이상 경과관찰이가 능했던120
증례에대해검토하였다.
또한같은기간내에 본과에서진단,
치료를실시한치성정각화낭종17
증례,
원 시성낭종230
증례,
함치성낭종523
증례,
에나멜상피종151
증례의대소비에대해서도일부비교,
검토를실시하였다.
전치부에서는최대 지름이4
치아이상,
구치부에서는3
치Table 1. The distribution of sex and age
Age Sex
Male Female Total (%)
09 1019 2029 3039 4049 5059 6069 7079 80
Total
2 16 26 18 13 7 6 4 1 93
2 19 38 13 7 9 2 2 1 93
4 (2.2) 35 (18.8) 64 (34.4) 31 (16.7) 20 (10.8) 16 (8.6)
8 (4.3) 6 (3.2) 2 (1.1) 186 (100) Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 2. The distribution of location
Molar~sinus Premolar Incisor and canine Others
(the range of lesion is more than two area) Total
Maxilla 20
(10.8%)
6 (3.2%)
7 (3.8%)
8 (4.3%)
41 (22.0%)
Molar~ramus Premolar Incisor and canine Others Total
Mandible 111
(59.7%)
8 (4.3%)
4 (2.2%)
22 (11.8%) Extending over both sides
8 (4.3%)
145 (78.0%)
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 3. Presenting symptoms
Symptom Number (%)
Swelling Pain Drainage
Feeling of wrongness Trismus
Tooth mobility
Asymptomatic (found incidentally by xray examination)
Total
70 (37.6) 36 (19.4) 18 (9.7) 8 (4.3) 7 (3.8) 1 (0.5) 46 (24.7) 186 (100) Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
그중
19
증례는상악동근치수술을병행하였다.
하악은90
증례중83
증례에대해적출후개방창의술식을사용하였 다.
이러한83
증례중병변이컸던35
증례에대해서는개창 요법을실행한후에적출하였다.(Fig. 3)
나머지7
증례중3
증례는적출후폐쇄창, 4
증례는악골변연절제술을실행하 였다.
매복치의경우,
맹출가능한것으로판단되는영구치 는보존을원칙으로하였고,
지치는모두발치하였다.
개창요법의
35
증례중22
증례(62.9%)
에서축소가확인되었고,
13
증례에서는크기변화를볼수없었다.(Table 6)
상악증례에서는
30
증례중4
증례에서재발이인정되었 고,
하악증례에서는적출후 개방창술식의경우83
증례 중14
증례(16.9%)
에서,
적출후폐쇄창술식의경우3
증례 중1
증례에서재발이인정되었다.
변연절제를실시한4
증 례에서는재발이인정되지않았다.
전체증례의재발률은120
증례중19
증례(15.8%)
였다.
또한개창요법과재발과의 관계를살펴본결과,
개창요법을실행한35
증례중5
증례(14.3%)
에서,
개창요법을실행하지않고적출방법을실행한
48
증례중9
증례(18.8%)
에서재발이인정되었다.
개창 요법의실행이적은재발경향을보였지만,
통계학적으로유의차는인정되지않았다
( P=0. 811).
(57.5%),
다방성이62
증례(33.3%)
였다.
병변과관련된매복치의존재유무는매복치가있는경우가
102
증례(54.8%),
매복치가없는경우가
82
증례(44.1%)
였다.(Table 4) 3. 치료법과 치료성적
본과에서수술을실시한후
, 1
년이상경과관찰을실시한
120
증례의치료법,
치료성적의결과를Table 5
에나타내었다
.
상악의경우30
증례모두적출후일차폐쇄하였고,
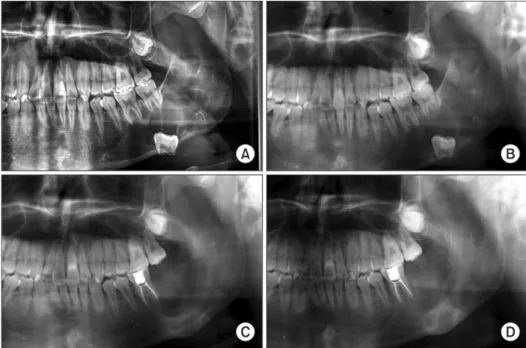
Fig. 3. A case that treated by enuclea- tion after the marsupialization. A. First examination. B. 3 months after the marsupialization (before the encleation).
C. 6 months after the enucleation. D. 1 year after the enucleation.
Nobuyoshi Tomomatsu et al: Clinical study of kera- tocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 4. Radiografic findings
Tumor variant Unilocular Multilocular Unknown Total Number 107 (57.5%) 62 (33.3%) 17 (9.1%) 186 (100%) Impacted tooth Containing Non Unknown Total
Number 102 (54.8%) 82 (44.1%) 2 (1.1%) 186 (100%) Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 5. Treatment results (recurrence/number)
Maxilla Mandible Total
Enucleation with marsupialization Enucleation (close) Marginal ostectomy Total
0/0 (0%) 4/30 [2/19]
(13.3%)
4/30 (13.3%)
14/83 (5/35) (16.9%)
1/3 (33.3%)
0/4 (0%) 15/90 (16.7%)
14/83 (16.9%)
5/33 (15.2%)
0/4 (0%) 19/120 (15.8%) Upper section [ ]: with radical operation of maxillary sinus, ( ):
enucleation after marsupilization. Under section recurrence rate.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 6. The effect of marsupialization
Number Recurrence Recurrence rate (%) Enucleation after
marsupialization Effective*
Noneffective Only enucleation Total
35 22 13 48 83
5 3 2 9 14
14.3 13.6 15.4 18.8 16.9
*Effective case: after the marsupialization, lesion reduced.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
종창
4
증례,
동통2
증례,
위화감2
증례,
기타11
증례에대해 서는증상없이경과관찰중에X
선사진에서발견된것이 대부분이었다.(Table 8)
재발부위는19
증례중18
증례가 악골에서재발하였으며,
그중7
증례가낭종에인접한잔존 치의치근부에서(Fig. 4), 4
증례가하악지상부에서재발하 였다.(Fig. 5)
연조직의재발도1
증례인정되었다.
X
선소견과재발과의관련에대해Table 9
에제시하였다.
X
선 소견에서다방성을띠는증례에서는43
증례중11
증 례(25.6%)
에서,
단방성의경우59
증례중8
증례(13.6%)
에 재발이인정되어다방성증례는단방성증례에비해재발 의 예가약간많았지만통계학적으로차이는인정되지못했다
( P=0.200).
매복치와재발과의관계는불분명한2
증례를제외한나머지를검토하였다
.
병변과관계가 있는매복 치를동반한52
증례에서는7
증례(13.5%)
에서,
그외동반 하지않는66
증례에서는12
증례(18.2%)
에서재발이인정4. 재발 시의 증상 및 X선 소견·매복치·크기와 치료
성적
수술후의경과관찰기간과재발과의관계를
Table 7
에 나타내었다.
경과관찰기간은1
년부터17
년까지로,
평균3
년2
개월이었다.
또한재발까지의기간은1
년4
개월부터12
년11
개월까지로,
평균6
년5
개월이었다.
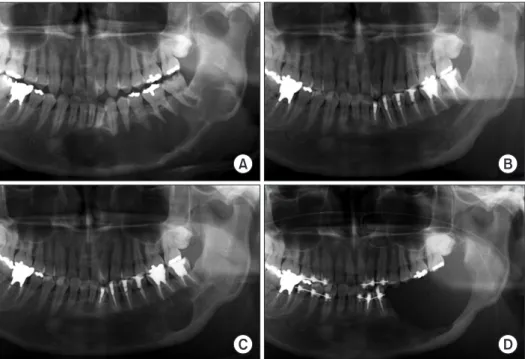
재발시증상은Fig. 4. The recurrence case 1 (the re- cu rrence location is root tip of the tooth). A. First examination. B. After the enucleation. C. Recurrence (3 years and 8 months after the enucleation). D.
Marginal ostectomy.
Nobuyoshi Tomomatsu et al: Clinical study of kera- tocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 7. The correlation between the follow-up period of 120 cases and recurrence
Followup period Recurrence Nonrecurrence
~2 year
~3 year
~5 year
~8 year
~10 year
~15 year 15 year~
Total
4 3 3 5 1 3 19
38 24 14 18 2 4 1 101 120 cases: followup periods is more than 1 year.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 8. Symptoms at the recurrence
Symptom Number Location of recurrence Number Swelling
Pain
Feeling of wrongness Asymptomatic (found incidentally by xray examination) Total
4 2 2 11
19
In the jaw bone Around the root tip The upper of ramus Other (in the bone) Soft tissue Total
18 7 4 7 1 19 Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 9. The correlation between radiografic finding and re- currence
Number Recurrence Recurrence rate (%) Tumor variant
(P=0.200) Impacted tooth (P=0.660) Size (P=0.137)
Unilocular Multilocular Unknown Containing No Known Large Small
59 43 18 52 66 2 69 51
8 11 0 7 12 0 14 5
13.6 25.6 13.5 18.2 20.3 9.8 Size: large size is more than 4 tooth in anterior area, or more than 3 tooth in posterior area.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
교한결과
,
큰증례69
증례중14
증례(20.3%)
에서,
작은증례
51
증례 중5
증례(9.8%)
에서재발이인정되어통계학적차이가없기는했지만큰증례에재발이많은경향을보였 다
( P=0. 137).
5. 각화낭성치성종양과 유사병변과의 비교
과거
25
년간본과에서진단,
치료를실시한각화낭성치 성종양은186
증례,
치성정각화낭종은17
증례,
원시성낭종 은230
증례,
함치성낭종은523
증례,
에나멜상피종은151
증례로그대소비(
대병변/
소병변)
를비교하였다.(Table 10)
각화낭성치성종양의 대소비는1.70,
치성정각화낭종은0.55,
원시성낭종은0.50,
함치성낭종은0.26,
에나멜상피종은
2.15
였다.
각화낭성치성종양과에나멜상피종의대소비는 치성정각화낭종
,
원시성낭종,
함치성낭종의대소비와 되었지만,
매복치와재발과의관련은통계학적으로명확하지않았다
( P=0.660).
또한 병변이큰증례(
전치부에서는4
치이상
,
구치부에서는3
치이상)
와그보다작은증례를비Fig. 5. The recurrence case 2 (the re- currence location is the upper of the ramous). A. First examination. B. 8 months after marsupialization, before the enucleation. C. Reccurence (3 years and 8 months after the enucleation).
Nobuyoshi Tomomatsu et al: Clinical study of kera- tocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
Table 10. The correlation between cystic tumor/cyst and size of lesion (25 years: 1981-2005)
Number Large Small Ratio a: keratocystic odonotogenic tumor
b: odontogenic orthokeratocyst c: primordial cyst
d: dentigerous cyst e: ameloblastoma
186 17 230 523 151
117 6 77 107 103
69 11 153 416 48
1.70 0.55 0.50 0.26 2.15 Ratio: large/small.
Pvalue: ab: 0.049, ac: 0.000, ad: 0.000, be: 0.015, ce: 0.000, de:
0.000.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
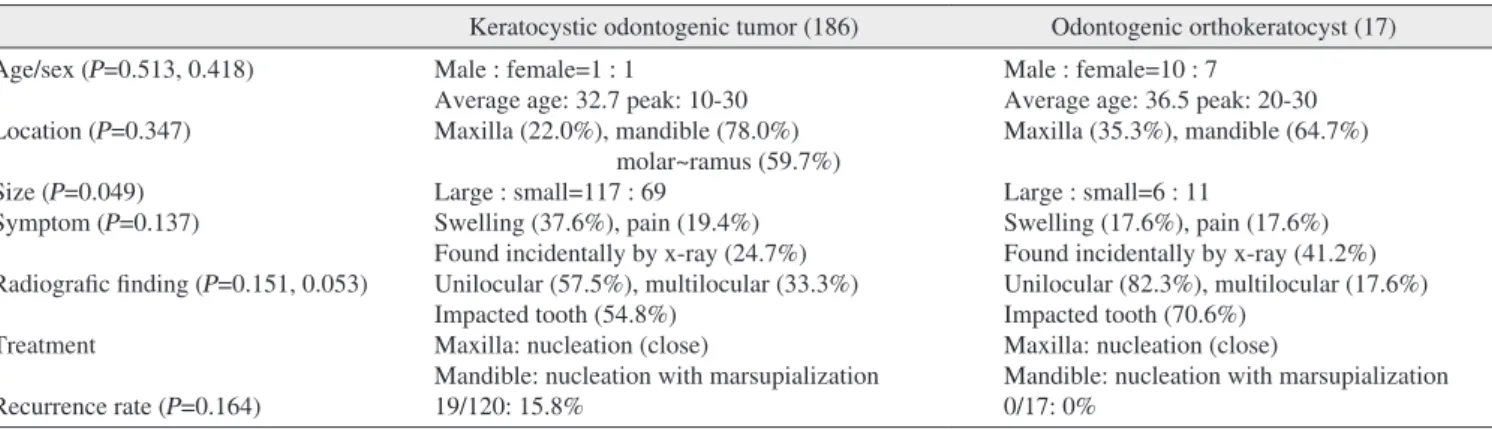
Table 11. The correlation between keratocystic odontogenic tumor and odontogenic orthokeratocyst
Keratocystic odontogenic tumor (186) Odontogenic orthokeratocyst (17) Age/sex (P=0.513, 0.418)
Location (P=0.347) Size (P=0.049) Symptom (P=0.137)
Radiografic finding (P=0.151, 0.053) Treatment
Recurrence rate (P=0.164)
Male : female=1 : 1
Average age: 32.7 peak: 1030 Maxilla (22.0%), mandible (78.0%)
molar~ramus (59.7%) Large : small=117 : 69
Swelling (37.6%), pain (19.4%) Found incidentally by xray (24.7%) Unilocular (57.5%), multilocular (33.3%) Impacted tooth (54.8%)
Maxilla: nucleation (close)
Mandible: nucleation with marsupialization 19/120: 15.8%
Male : female=10 : 7 Average age: 36.5 peak: 2030 Maxilla (35.3%), mandible (64.7%) Large : small=6 : 11
Swelling (17.6%), pain (17.6%) Found incidentally by xray (41.2%) Unilocular (82.3%), multilocular (17.6%) Impacted tooth (70.6%)
Maxilla: nucleation (close)
Mandible: nucleation with marsupialization 0/17: 0%
Pvalue: between keratocystic odontogenic tumor and odontogenic orthokeratocyst.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
지로
1030
대가많았으며,
평균32.7
세였다. 2. 부위
지금까지치성각화낭종은 하악
,
특히지치부에 호발하 는것으로보고되었다3,11,18,19,22.
각화낭성치성종양에한정시 킨자체 실험증례에서도186
증례중145
증례(78.0%)
가하 악에서발생하였고,
그중에서도하악대구치부로부터하악 지부에많았다.
상악증례에서는대구치부로부터상악동에 걸친부위가많았다.
3. 임상증상
지금까지치성각화낭종의임상증상에는감염등으로 인 한 이차적증상도포함되어종창
,
동통,
배농,
개구장애의 순으로다수인정된다고보고된반면,
무증상으로증대하 여X
선검사에서우연히발견되는증례도적지않다는보고도있다3,14,22
.
각화낭성치성종양에한정시킨자체실험증례에서도종창
,
동통을증상으로하는증례가많았지만(
합계
57.0%),
무증상으로X
선검사를통해우연히발견된증례도
24.7%
를차지하였다. 4. X선 소견
지금까지 치성각화낭종의
X
선 화상은 단방성이 비교 적 많은 것으로 알려졌다(6380%)
11,18,19,22,23.
각화낭성치 성종양의 자체실험증례에서도 단방성(57.5%)
은 다방성(33.3%)
에비해약간많아종래의보고와같은경향을보였다
.
병변에 인접한매복치는종래의 치성각화낭종에서49.556.3%
가인정되었다는보고3,11,19,22,24가있었으며,
자체 실험증례에서도54.8%
로종래의치성각화낭종의 보고와 거의일치하였다.
5. 재발
재발에관해서는이전부터 많은보고가있었다
.
그러나 상피의 착각화 혹은정각화의 구분없이치성각화낭종으 로보고된다수의자료중각화낭성치성종양의진단기준에 비교시 통계학적으로의미가있어 본종양과에나멜상피종은발견시 치성정각화낭종
,
원시성낭종,
함치성낭종에 비해큰병변이많은것을알수있었다( P<0.05).
또한이번분류를통해종래의치성각화낭종은각화낭성 치성종양과치성정각화낭종으로재분류되었다
.
임상적차이에대해검토한결과를
Table 11
에제시하였다.
통계학적검토결과
, P
값은 각각성별0.513,
연령0.418,
발생부위
0.347, X
선소견의단방성의비율0.151,
매복치의유무0.053
으로통계학적의미는없었지만,
초진시의병변크기에대해서는
0.049
로 유의하여본종양이치성정각화낭종에비해발견시큰증례가많은것을알수있었다
.
또한재발률에관해서는
P
값이0.164
로의미가없었다.
이는각화낭성치성종양
(120
증례)
과비교시치성정각화낭종의증례 수가17
증례로대단히적기때문에통계학적차이를인정 받지못한것으로생각한다.
IV. 고 찰
2005
년에치성종양에관한WHO
조직 분류가개정되어 종래의치성각화낭종은낭종외장상피가착각화를띠는것 은각화낭성치성종양으로분류되어양성종양의하나로다 뤄지게되었다1.
지금까지치성각화낭종의재발에관한통 계학적검토는다수보고된바있고,
그원인에대해서도다 수의견해가 피력되었다11,13,19,22.
그러나상피가 착각화를 띠는각화낭성치성종양만을다룬연구보고는그다지많지 않다.
이러한까닭에과거25
년간 본과에서진단,
치료를 실시한단발증례의낭종성병변을재검토하여새로운분 류기준에준한각화낭성치성종양에대해검토하였다.
1. 성차·연령
각화낭성치성종양을포함한종래의치성각화낭종에대
한보고를살펴보면
,
성차를인정하지않는것2224,
남성에약간많다는것3,4,13,18,22,23등이 있지만각화낭성치성종양의
자체실험증례에서는전혀성차가인정되지않았다
.
연령 의경우,
종래의치성각화낭종에서는일반적으로1030
대 에많은것으로알려져있다.
자체실험증례에서연령분포 는7
세부터85
세까지폭넓게분포하여다른보고와마찬가Table 12. The comparison of the treatment result of keratocystic odontogenic tumor
Report year Reporter Number Recurrence Recurrence rate (%) Followup period
1988 1988 2000 2001 2007
Harada, et al.
Hatake, et al.
Matuki, et al.
Hoon, et al.
This report
11 9 21 132 120
5 3 3 77 19
45.5 33.3 14.3 58.3 15.8
More than 6 months More than 6 months More than 1 year More than 1 year The other reports were the treatment result of odontogenic keratocyst, but the author calculated as keratocystic odontogenic tumor.
Nobuyoshi Tomomatsu et al: Clinical study of keratocystic odontogenic tumors. J Korean Assoc Oral Maxillofac Surg 2012
6. 각화낭성치성종양과 유사병변과의 비교
X
선소견,
임상소견만으로본질환을진단하는것은곤 란하다.
이에본질환과 기타낭종성질환,
에나멜상피종의X
선사진상에서의대소비를조사한결과,
각화낭성치성종 양과에나멜상피종은병변의최대지름이큰증례가치성정 각화낭종,
원시성낭종,
함치성낭종과비교시유의차를갖 는다수인점을확인하였다.
이조건은진단의스크리닝으 로서유용할것으로생각한다.
본검토에서치성정각화낭종은
17
증례로소수이지만재 발증례는인정되지않았으며,
원시성낭종와함치성낭종을합친재발률은
0.3%
로대단히낮았다.
이와비교시각화낭성치성종양의재발률은
15.8%
로확연히높았다.
치료전생 검을통해확정진단을받을것을권하는보고도있어15,18,28,
본연구에서도수술전생검을거쳐확정진단을받은각화 낭성치성종양의경우는재발률이높았기때문에근치성의 높은치료를실시할필요가있다.
즉,
병변에근접한치아의 발치,
보다큰개창의실시,
병변적출후의주위골삭제등 을 적극적으로시행하는쪽이바람직한것으로생각한다.
또한에나멜상피종의개창반복요법처럼첫번째수술은가 급적적출후개방창으로하여뼈의회복을기다린다음두 번째 수술에서주위골과함께 병변을절제하는술식도검 토할필요가있다고여겨진다.
또한술후의경과관찰기간 에관해서도재발률의정도,
재발시기의관점에서10
년이 상의경과관찰은필요하다고하겠다.
한편수술전 생검을통해비각화성의함치성낭종과원 시성낭종
,
정각화성의치성정각화낭종의경우인접치의처 리에서도보다보존가능한방향으로진행시켜악골·
치아 를 가능한한온존시키는치료로충분히치유될가능성이 높으며,
이와동시에수술후의경과관찰기간도단축가능 할것으로생각하지만,
향후증례수를늘려검토해나갈필 요가있다.
V. 결 어
과거
25
년간 각화낭성치성종양으로진단된 단발 증례186
증례에대해임상적검토와함께유사악골병변과비교한결과이하의결론을얻게되었다
. 1. 각화낭성치성종양에 대하여
1)
발생빈도에성차는없었으며,
초진시연령은1030
대가많았다
.
2)
부위는상악41
증례,
하악145
증례였으며,
상악에서는 대구치부로부터상악동에걸쳐서,
하악에서는대구치 부로부터하악지부가많았다.
합치되는것만을발췌하여
Table 12
에제시하였다4,817.
자 체실험증례에서의재발률은15.8%
로,
종래의보고(14.3
58.3%)
3,14,15,19와비교할때 관찰기간이상이하다는전제하에자체 실험증례의재발률은반드시높은수치는아니었 다
.
또한,
치성정각화낭종17
증례에서재발은인정되지않 았다.
정각화를띠는치성각화낭종의재발은02.2%
라는보고9,12,20가있으며
,
자체실험증례에서도동일하였다.
재발원인에대해이전의보고에서는 병변의일괴적출 곤란에따른상피조직의잔존이주된재발의요인으로여
겨져왔다11,18,19
.
재발부위는鵜澤
등13이보고한것(
치성각화낭종
)
처럼낭종에인접한잔존치의치근부가많았으며,
이번검토에서도19
증례중7
증례가이에해당되었다.
이 로인해병변에인접한치아의처리가문제로대두된다.
재 발을방지하는관점에서인접치를발치해야한다는보고도 있지만,
새로운논의를필요로한다25.
또한 하악구치부로 부터하악지상부,
근돌기에이르는큰병변의경우하악지 상부에재발한경우가4
증례있었으며,
이는적출하기어려 운부위에기인하는것으로생각한다.
X
선소견과재발과의관련에대해横林
등11의보고에의하면크기그자체에차이는없다고한다
.
그러나자체실험 증례에서는작은병변의증례(
병변의최대지름이구치부 에서는3
치미만,
전치부에서는4
치미만)
의재발이9.8%
인 것에비해,
큰병변의증례에서는20.3%
의재발률을보였 다. Forssell
등26은재발증례의70%
가X
선검사에서최대지름
4 cm
이상으로,
큰병변이재발률이높다고보고하였으며자체실험증례도같은결과였다
.
또한,
매복치의존재에차이가없다는보고22,27나포함하지않는쪽이재발률이
높은경향이라는보고24도있다
.
자체실험증례에서는매복 치를포함하지않는쪽에약간많은재발이인정되었지만,
통계학적으로유의차는볼수없었다.
재발까지의기간은수술후
5
년이내라는보고3,11,24가많 지만,
자체실험증례에서는재발19
증례중10
증례는5
년 이내, 9
증례는5
년을넘겨재발하였다. Brannon
9의보고와 마찬가지로자체 실험증례에서도8
년을넘겨재발한증례 가4
증례있어,
수술후의경과관찰기간은10
년이상이바 람직한것으로여겨진다.
본과에서는상악의 경우적출후 폐쇄창
,
하악은 적출 후개방창으로처치하는경우가대부분으로,
적출후처치 법에따른재발률의차이는인정되지않았다.
큰병변에대 한개창요법의35
증례중축소효과가인정된것은22
증례(62.9%)
로,
하악하연이나하악관보존이가능한점에서개창요법의 유용성에대해서는 이후상세한검토가필요할 것으로생각한다
.
또한,
하악골구역절제술및하악골변연 절제술은침습이크지만자체실험증례에서도대단히낮은 재발빈도를보임으로써큰재발병변의경우에적극적으 로적용할만하다하겠다.
a benign cystic neoplasm? Part 1. Clinical and early experimental evidence of aggressive behaviour. Oral Oncol 2002;38:21926.
6. Shear M. The aggressive nature of the odontogenic keratocyst: is it a benign cystic neoplasm? Part 2. Proliferation and genetic studies.
Oral Oncol 2002;38:32331.
7. Gorlin RJ, Goltz RW. Multiple nevoid basalcell epithelioma, jaw cysts and bifid rib. A syndrome. N Engl J Med 1960;262:90812.
8. Pindborg JJ, Hansen J. Studies on odontogenic cyst epithelium.
2. clinical and roentgenologic aspects of odontogenic keratocysts.
Acta Pathol Microbiol Scand 1963;58:28394.
9. Brannon RB. The odontogenic keratocyst. A clinicopathologic study of 312 cases. Part I. Clinical features. Oral Surg Oral Med Oral Pathol 1976;42:5472.
10. Brannon RB. The odontogenic keratocyst. A clinicopathologic study of 312 cases. Part II. Histologic features. Oral Surg Oral Med Oral Pathol 1977;43:23355.
11. 横林敏夫, 横林康夫. 歯原性角化嚢胞の再発に関する検討. 日
口外誌 1984;30:133847.
12. 岩渕博史, 矢郷 香. 歯原性角化嚢胞の角化のタイプによる臨 床病理学的相違. 日口外誌 1996;42:1705.
13. 鵜澤成一, 喜代崎郁子. 歯原性角化嚢胞に関する臨床的研究−
再発に関する因子について−. 日口外誌 2003;49:938.
14. 松木謙直, 市原秀記. 歯原性角化嚢胞 29 症例の臨床病理学的 検討. 日口外誌 2000;46:2324.
15. Myoung H, Hong SP, Hong SD, Lee JI, Lim CY, Choung PH, et al. Odontogenic keratocyst: Review of 256 cases for recurrence and clinicopathologic parameters. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:32833.
16. Morgan TA, Burton CC, Qian F. A retrospective review of treatment of the odontogenic keratocyst. J Oral Maxillofac Surg 2005;63:6359.
17. Chirapathomsakul D, Sastravaha P, Jansisyanont P. A review of odontogenic keratocysts and the behavior of recurrences. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:59.
18. 飯野光喜, 松田耕策. 歯原性角化嚢胞 24 症例の臨床ならびに 病理組織学的検討. 日口外誌 1989;35:96473.
19. 畑毅, 細田 超. 歯原性角化嚢胞の臨床病理組織学的検討. 日口 外誌 1988;34:47084.
20. Crowley TE, Kaugars GE, Gunsolley JC. Odontogenic keratocysts:
a clinical and histologic comparison of the parakeratin and orthokeratin variants. J Oral Maxillofac Surg 1992;50:226.
21. 武田泰典, 高田 隆. WHO による歯原性腫瘍の新たな組織分類と それに関連する上皮性嚢胞について. 日口外誌 2006;52:5461.
22. 重松久夫, 鈴木正二. 歯原性角化嚢胞の治療とその再発に関す る臨床病理学的検討. 日口外誌 1998;44:30310.
23. 永峰浩一郎, 江場光芳. 当講座における過去 11 年間の歯原性 角化嚢胞症例の検討. 日口外誌 1991;37:185361.
24. Browne RM. The odontogenic keratocyst. Clinical aspects. Br Dent J 1970;128:22531.
25. 榎本昭二, 岩佐俊昭. 原始性嚢胞 (Primordialcysts) の臨床的研 究. 日口外誌 1977;23:1218.
26. Forssell K, Sorvari TE, Oksala E. An analysis of the recurrence of odontogenic keratocysts. Proc Finn Dent Soc 1974;70:13540.
27. Bataineh AB, al Qudah M. Treatment of mandibular odontogenic keratocysts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:427.
28. Brøndum N, Jensen VJ. Recurrence of keratocysts and decompression treatment. A longterm followup of fortyfour cases. Oral Surg Oral Med Oral Pathol 1991;72:2659.
3)
증상으로는종창(37.6%),
동통(19.4%)
등이많았고,
무증상
(X
선 검사를통해우연히발견하는경우: 24.7%)
도적지않았다
.
4) X
선소견으로는단방성이다방성에비해약간많았다.
병변과관련이있는매복치는
54.8%
에서인정되었다.
5)
치료법으로는상악에서는적출후폐쇄창,
하악에서는 적출후개방창으로한증례가많았지만치료 성적에 명확한차이는없었다.
6)
재발과X
선소견으로서의단방성·
다방성,
매복치아 의유무,
크기에관해서는통계학적으로는차이를인 정받지못했다.
7)
수술후1
년이상의관찰기간을갖는120
증례에대해검토한결과
,
재발률은15.8%
였다.
재발까지의기간은1
년4
개월로부터12
년11
개월로, 10
년이상의경과관 찰이바람직하다고생각한다.
2. 각화낭성치성종양과 유사병변과의 비교
1) X
선 사진상에서의대소비비교에서각화낭성치성종 양과 에나멜상피종은 치성정각화낭포,
원시성낭종,
함치성낭종과비교시큰병변이차지하는비율이의 미있게많았다.
2)
각화낭성치성종양(
재발률: 15.8%)
과치성정각화낭종(
재발률: 0.0%)
의재발률에통계학적으로의미있는차이는없었다
.
이는치성정각화낭종의증례수가 적기 때문으로생각되며(17
증례),
이후증례수를늘려검토 해갈필요가있다.
3)
큰낭종성병변의경우,
생검에서확정진단으로표피가 착각화를나타내는각화낭성치성종양은보다근치성 의높은수술방식을택하는것이바람직하다고생각 한다.
References
1. Barnes L, Eveson JW, Reichart P. World Health Organization classification of tumours, pathology and genetics of tumours of the head and neck. Lyon: International Agency for Research on Cancer; 2005:3067.
2. Philipsen HP. Keratocysts in the jaws. Tandlaegeblader 1956;60:
96380.
3. 原田昌和, 山元 学. 当科における過去18年間の歯原性角化嚢胞
症例の検討. 日口外誌 1988;34:65763 .
4. Ahlfors E, Larsson A, Sjögren S. The odontogenic keratocyst: a benign cystic tumor? J Oral Maxillofac Surg 1984;42:109.
5. Shear M. The aggressive nature of the odontogenic keratocyst: is it