[원저]
혈중 Carotenoids농도와 대사증후군의 관련성
박계원, 김성희, 이건호
대구가톨릭대학교 의과대학 가정의학과Association between Serum Carotenoids and Metabolic syndrome
Ke Won Park, Sung Hi Kim, Geon Ho Lee
Department of Family Medicine, Daegu Catholic University Medical School
Background This study investigated the association between serum carotenoids as antioxidants and metabolic syndrome as a risk factor of cardiovascular disease. In addition, the relationships among oxidative stress, metabolic syndrome and antioxidants were assessed.
Methods From September to December, 533 subjects (>40 yrs, men: 342, women: 181) from one general hospital joined this study. They were grouped into: normal (460), metabolic syndrome without central obesity (13) and metabolic syndrome with central obesity (60). We analyzed associations among 1) serum carotenoids and metabolic syndrome considering central obesity and gender (ANCOVA), 2) serum carotenoids and the 5 components of metabolic syndrome (ANOVA, ANCOVA) and 3) serum carotenoids and risk factors for cardiovascular disease (correlation test) by SPSS 12.0. Serum carotenoid concentrations were adjusted for age, gender, smoking, alcohol use, physical activity, intake of fruits and vegetables and supplement use (vitamins and minerals).
Results Serum carotenoid levels were lower in the presence of metabolic syndrome, with the lowest levels seen in metabolic syndrome with central obesity. Serum levels of β-carotene were lower with most components of the metabolic syndrome and decreased according to increasing numbers of components (negative dose-response relationship, p<0.05).
Conclusions This study showed that serum carotenoids are associated with the metabolic syndrome.
(Korean J Health Promot Dis Prev 2009 ; 9(4):314-320) Key words Carotenoids, metabolic syndrome, oxidative stress, cardiovascular disease
1서 론
대사증후군의 정의에는 여러 기준이 사용되고 있으나, 본 연 구에서는 NCEP ATP II(National Cholesterol Education Program Adult Treatment Panel III) 서태평양지역 권고안 (modified NCEP ATPIII; 허리둘레, 남>90cm, 여>80cm)
1,2)을 이용하였다. 대사증후군이 동반된 경우 심혈관질환 위험율은 50-60% 증가하는데
3), 우리나라 유병율은 연구자에 따라 남녀
∙교신저자 : 김 성 희
∙주 소 : 대구가톨릭대학교병원 가정의학과
∙전 화 : 010-4526-8456
∙E-mail : [email protected]
∙접 수 일 : 2009년 4월 13일 ∙채 택 일 : 2009년 10월 21일
의 차이는 있지만, 20%이하이다
4)(modified ATP III진단기준).
역학조사 결과, 세계적으로 대사증후군은 증가하는 추세이며 특히, 아시아 지역의 증가가 두드러지는 것으로 보고 되고 있다.
이는 당뇨 및 심혈관질환 발생 증가가 예측되고
5-7)보건의료 차 원에서 삶의 질 향상, 사회적 비용 절감, 질병 예방 차원을 위해 서 대사증후군 관리가 중요함을 알 수 있다.
8)대사증후군 기전으 로는 유전요인과 환경요인이 상호작용할 것으로 추정되고 있지 만, 아직은 대부분의 연구가 역학적 연구가 많으며 명확한 원인 이 규명된 것은 아니다.
9)대사증후군에서 산화스트레스가 증가 하여 심혈관질환이 악화되는 반면, 항산화제는 산화스트레스에 의한 유리활성기를 제거하여 심혈관질환에 대한 예방 효과가 있
다.
10,11)음식의 형태로 섭취하는 항산화제로는 carotenoids, vitamin
C, E 등이 있는데, carotenoids는 과일과 야채의 밝은 색깔을 나 타내는 자연 색소로서 음식으로 섭취되는 항산화물질이다. 역학 적 연구들에서 carotenoids는 암을 포함한 만성질환에 예방적 효과를 보이었으나 임상 연구들에서 보충제형태로 다량 복용하 면 암, 심장질환 예방효과가 없어질 뿐만아니라 폐암 등이 고위 험군(흡연, 석면 노출 등)에서 증가하여
12)음식섭취를 통해 얻어 지는 정도의 양에서 carotenoids가 예방효과가 있음이 알려졌다.
본 연구에서는 다섯가지 carotenoids (
α-carotene,
β-carotene, lycopene, crytoxanthine, lutein) 면접조사를 통해 얻은 보충제 섭취량을 분석 시에 보정하였다)의 혈중 농도를 측정하여 대사 증후군과의 관련성을 알아보고자 하였다.
방 법
1. 연구대상
2005년 9월-12월까지 일개 대학병원에서 본인의 동의를 받 은 40세 이상의 건강검진자 533명(남자 342명, 여자 191명)을 대상으로 설문조사 및 추가 혈액검사를 시행하였다.
2. 연구방법
1) 신체계측 및 설문조사
대상자들의 체질량지수(몸무게/키(m
2), 허리둘레 및 혈압 을 측정하였고, 흡연, 음주, 운동, 비타민제 복용 등의 생활습 관과 질병력, 가족력은 구조화된 설문지를 이용하여 면접조 사를 하였다. 음주는 기간, 술종류(7종류 술의 알콜도수), 음 주빈도(1개월), 1회 음주시 음주량(ml)을 곱하였고, 흡연은 비 흡연, 과거흡연, 현재흡연으로 구분하고 흡연기간(년)에 1일 흡연 평균량(개피)을 곱하여 총흡연양을 구하였다. 운동양은 1주 평균 운동빈도와 운동시간을 곱하여 총운동량을 구하였 고, 비타민제는 비타민종류(4종류)에 따라서 1주 평균 복용 빈도에 복용기간(개월)을 곱하여 총량을 구하였다.
2) 혈청검사
8시간 공복상태에서 혈당, 중성지방, 고비중콜레스테롤을 측정 하였고, 혈청 carotenoids (a-carotene, b-carotene, cryptoxanthine, lycopene, lutein)측정은 HPLC (reverse phase system, Hewlett Packard 1100 series)를 사용하였다.
3) 대사증후군의 정의
본 연구에서는 복부비만 기준을 WHO 서태평양지역의 권
고를 따른modified NCEP-ATP III 기준을 적용하였으며, 아 래의 5가지 진단기준 중에서 3가지 요소 이상 포함되면 대사 증후군으로 정의하였다.
① 고혈압: >130/85 혹은 고혈압병력 (+)
② 허리둘레 남자 >90 cm, 여자 >80 cm
③ 고중성지방혈증: >150 mg/dL
④ 저HDL콜레스테롤혈증: 남자 <40 mg/dL, 여자 <50 mg/dL
⑤ 고혈당: 공복시 >110 mg/dL 혹은 당뇨병력 (+) 3. 분석방법
SAS version 12.0을 이용하여 통계분석을 하였으며 조사대상 자 (533명)의 일반적 특징을 대조군 (460명), 복부비만이 없는 대 사 증후군 (13명), 복부비만이 있는대사증후군 (60명)의 세군으 로 구분하여 비교였다 (
χ2-test, ANOVA). 혈중 carotenoids 농도 는 좌왜도 (Left skewed)분포를 하여 log치환을 시행하였고(이 후, carotenoids 농도는 모두 log치환된 수치를 나타냄), 대사증 후군 위험요소에 따라 혈중 carotenoids 농도를 비교하고 (ANCOVA), 심혈관질환 위험요소와 carotenoids 농도의 상관관 계를 알아보고 (correlation analysis). carotenoids가 대사증후군 예방에 미치는 효과를 분석하였다 (multiple logistic regression analysis). 그리고 대조군 (460명), 복부비만이 없는 대사 증후군 (13명), 복부비만이 있는대사증후군 (60명)의 세군으로 구분하여 carotenoids 농도를 비교하였고 (ANCOVA), 성별에 따라 carotenoids 농도를 비교하였다 (ANCOVA). 분석 시 성별, 나이, 흡연, 운동, 음주, 야채 및 과일의 섭취, 보충제섭취, 체질량지수 및 총콜레스테롤을 보정하였다 (covariates).
결 과
1. 연구대상자의 일반적 특성
40세 이상을 조사대상으로 하였으며 조사대상자 수는 533명
(남자 342명, 여자 191명)으로 대조군 460명, 대사증후군 73명
[복부비만 (-) 13명, 복부비만 (+) 60명]이었고 연령은 대조군이
49.79±6.18 세 대사증후군이 50.50±6.65 로 차이가 없었다. 대사
증후군 유병율은 13.7% (남자 13.16%, 여자 14.66%) 으로 다른
연구들과 비슷하였고.
11)복부비만이 있는 대사증후군이 연령,
흡연 양이 가장 많았다 (p<0.05, Table 1).
Table 1. General characteristic of participants
Control MS†(-central obesity) MS†(+central obesity)
n=533 n=460 n=13 n=60
Men/Women (n) 271 / 146 9 / 4 36 / 24
Age (year) 49.79 ± 2.38 50.08 ± 1.57 52.9 ± 2.68
BMI (kg/m2) 23.81 ± 2.38 24.22 ± 1.57 27.16 ± 2.68*
Waist circum (cm) 82.16 ± 6.9 82.76 ± 5.74 93.58 ± 7.69
- Life style - smoking(pack yr)* Alcohol (g/day) Exercise Vegetable intake Fruits* intake Supplement intake
24.58 ± 15.64 16.71 ± 13.01 1.04 ± 0.06 458.29 ± 9.73 138.10 ± 2.14 0.50 ± 0.03
35.69 ± 114.94 16.72 ± 69.12 0.92 ± 0.31 492.46 ± 65.99 128.54 ± 27.59 0.92 ± 0.21
36.032 ± 66.03 18.74 ± 41.14 0.93 ± 0.14 470.95 ± 27.48 154.78 ± 46.10 0.60 ± 0.10 Values are mean±SD, ANOVA
BMI: Body Mass Index, MS†: Metabolic Syndrome
*p<0.05
Table 2. Serum concentrations of carotenoids and metabolic syndrome components
components of MS† Abdominal obesity Hyper triglyceridemia Low HDL cholesterol Hypertension Hyperglycemia
+ - + - + - + - + -
n 140 350 158 332 98 392 200 290 57 433
α-Carotene (μg/dl) 0.0067 0.0067 0.0057 0.0071** 0.0067 0.0067 0.0066 0.0069 0.0056 0.0068*
β-Carotene (μg/ml) 0.223 0.272** 0.208 0.284** 0.223 0.266* 0.235 0.273* 0.209 0.264**
Lycopene (μg/dl) 0.052 0.064* 0.050 0.066** 0.058 0.061 0.058 0.062 0.048 0.062*
Cryptoxanthine (μg/ml) 0.306 0.321 0.291 0.330 0.245 0.338** 0.326 0.311 0.331 0.315
Lutein (μg/m)l 0.259 0.266 0.268 0.262 0.252 0.267 0.262 0.266 0.264 0.264
Adjusted for age, gender, smoking status, alcohol intake, physical activity, fruit/vegetable intake, vitamin/mineral use ANCOVA, MS†: Metabolic syndrome
*p<0.05, **p<0.005
Table 3. Serum concentrations of caroteroids and number of metabolic syndrome components
n of MS† components 0 1 2 3 ≥4
p value
n (490) 137 157 123 44 29
α-Carotene** (μg/dl) 0.0075 0.0066 0.0060 0.0074 0.0053 0.000
β-Carotene** (μg/ml) 0.314 0.270 0.225 0.226 0.167 0.042
Lycopene (μg/dl) 0.084 0.085 0.071 0.078 0.044 0.126
β-Cryptoxanthine (μg/ml) 0.353 0.323 0.335 0.327 0.233 0.126
Lutein (μg/ml) 0.259 0.259 0.260 0.244 0.258 0.052
Adjusted for age, gender, smoking status, alcohol intake, physical activity, fruit/vegetable intake, vitamin/mineral use ANCOVA, MS†: Metabolic syndrome
*p<0.05, **p<0.005
2. 혈중 carotenoids 농도와 대사증후군의 관련성
β
-carotene은 모든 대사증후군 요소에 대해서 혈중 농도가 유의하게 감소하였고
α-carotene은 고중성지방혈증, 고혈당군 에서 농도가 저하되었다. Lycopene은 복부비만, 고 중성지방혈 증, 고혈당에서, cryptoxanthine은 저HDL혈증에서 각각 농도
가 유의하게 감소 하였다 (p<0.05, Table 2). 대사증후군 항목 수 증가에 따라
β-carotene 농도는 직선상의 유의한 감소를 보 이었으며 (p=0.042)
α-carotene은 유의한 감소를 보이었으나 항 목수가 세가지인 경우에 농도가 증가하였다 (Table 3).
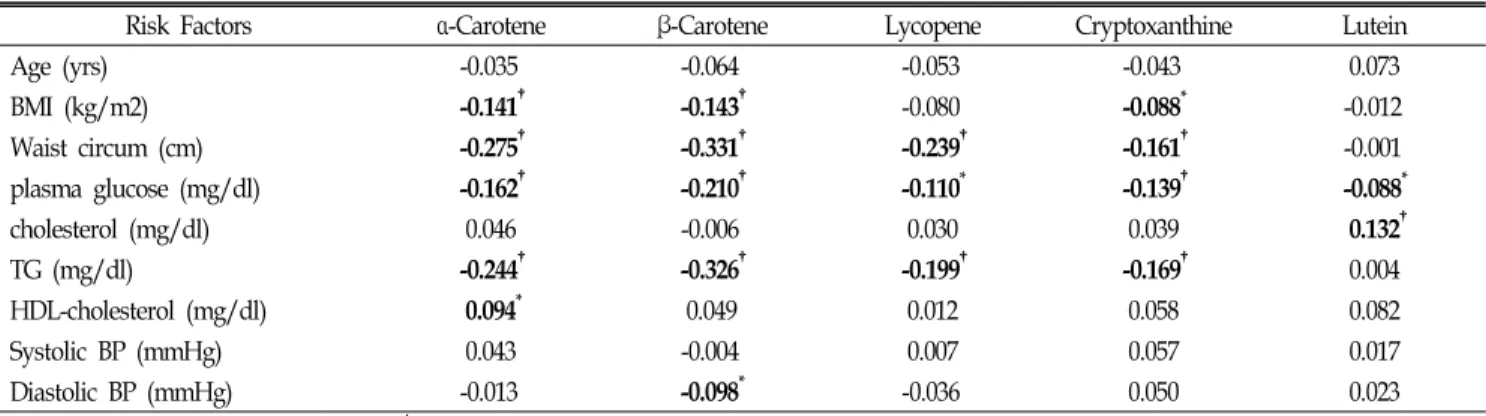
상관분석에서 연령은 혈중 carotenoids 농도와 무관하였다.
α와
β-carotene은 대부분의 대사증후군요소와 역 상관성이 있었고
Table 4. Correlations of carotenoids concentrations and cardiovascular disease risk factors
Risk Factors α-Carotene β-Carotene Lycopene Cryptoxanthine Lutein
Age (yrs) -0.035 -0.064 -0.053 -0.043 0.073
BMI (kg/m2) -0.141† -0.143† -0.080 -0.088* -0.012
Waist circum (cm) -0.275† -0.331† -0.239† -0.161† -0.001
plasma glucose (mg/dl) -0.162† -0.210† -0.110* -0.139† -0.088*
cholesterol (mg/dl) 0.046 -0.006 0.030 0.039 0.132†
TG (mg/dl) -0.244† -0.326† -0.199† -0.169† 0.004
HDL-cholesterol (mg/dl) 0.094* 0.049 0.012 0.058 0.082
Systolic BP (mmHg) 0.043 -0.004 0.007 0.057 0.017
Diastolic BP (mmHg) -0.013 -0.098* -0.036 0.050 0.023
Pearson correlation coefficients. *P<0.05, †P<0.01.
Table 5. Serum concentrations of carotenoids and metabolic syndrome without and with obesity
n (490) Control MS†(-central obesity) MS†(+central obesity)
417 13 60
α-Carotene (μg/dl) 0.006 0.005 0.006
β-Carotene†(μg/ml) 0.268a 0.201ab 0.198b
Lycopene (μg/dl) 0.062 0.055 0.050
Cryptoxanthine (μg/ml) 0.322 0.254 0.294
Lutein (μg/ml) 0.267 0.226 0.252
Adjusted for age, gender, smoking status, alcohol intake, physical activity, fruit/vegetable intake, vitamin/mineral use
†p<0.001,
a, ab, b
: multiple comparison ANCOVA, MS†: Metabolic syndrome
Table 6. Serum concentrations of carotenoids and metabolic syndrome according to gender
n (490) Total Control Metabolic syndrome
M (316) F (174) M (271) F (146) M (45) F (28)
α-Carotene (μg/dl) 0.006 0.008† 0.006 0.007† 0.006 0.009†
β-Carotene (μg/ml) 0.216 0.342† 0.233 0.348† 0.176 0.260
Lycopene (μg/dl) 0.064 0,102† 0.054 0.082† 0.055 0.086
β-Cryptoxanthine (μg/ml) 0.282 0.404† 0.292 0.388† 0.300 0.316
Lutein (μg/ml) 0.253 0.261 0.263 0.275 0.241 0.258
Adjusted for age, smoking status, alcohol intake, physical activity, fruit/vegetable intake, vitamin/mineral use
*p<0.05, †p<0.005, ANCOVA MS†: Metabolic syndrome
Table 7. Odds ratio of metabolic syndrome by quartile of carotenoid concentration
n (533) Quartile of serum carotenoid concentration
p trend*
I II III IV
α-Carotene (μg/dl) 2.32(1.00- 5.38) 2.14(0.93-4.92) 1.42(0.60-3.40) 1 0.140
β-Carotene(μg/ml) 5.35(2.16-13.26) 1.95(0.75-5.06) 1.39(0.55-3.51) 1 0.000
Lycopene (μg/dl) 2.08(0.92- 4.72) 1.11(0.43-2.86) 1.14(0.50-2.64) 1 0.233
β-Cryptoxanthine (μg/ml) 1.27(0.60- 2.68) 1.11(0.50-2.43) 0.97(0.45-2.12) 1 0.888
Lutein (μg/ml) 1.43(0.70- 2.92) 0.99(0.46-2.15) 0.70(0.32-1.57) 1 0.340
*Multiple logistic regression analysis, adjusted for age, smoking status, alcohol intake, physical activity, fruit/vegetable intake, vitamin/mineral use.
(p<0.05) lycopene, cryptoxanthine, lutein의 일부 요소들과 역상관 성이 있었다 (Table 4).
β-carotene 농도는 대조군, 복부비만이 없는 대사증후군 그리고 복부비만이 동반된 대사증후군의 순서로 유의하게 감소하였다(p<0.001, Table 5). 남자에서 혈중 carotenoids 농도가 유의하게 낮았다 (lutein 제외, p<0.05, Table 6).
3. 혈중 carotenoids농도에 따른 대사증후군의 위험도 (교차비)
β
-carotene 농도의 4분위수를 기준으로 1분위수의 대사증후 군 위험도는 5.35배 (CI 2.16-13.26) 증가하였으며, 2분위수와 3 분위수에도 위험도가 각각 1.95배, 1.39배 증가하였으나 유의하 지는 않았다.
α-carotene, cryptoxanthine에서도 혈중 농도 저하 에 따른 대사증후군위험도가 증가하는 경향을 보이었으나 유 의하지 않았다 (Table 7).
고 찰
본 연구에서 혈중 carotenoids는 대사증후군에 대한 예방 효과가 있었으며 특히,
β-carotene이 낮은 경우에는 대사증후 군의 위험도가 5배 이상 증가하였다. 대사증후군은 복부비만 과 고인슐린혈증에 의한 이상지지혈증, 고혈압, 혈당장애를 포함 하는 대사장애 집합 체이며 기준으로는 복부비만 중심 의 NCEP ATP III 정의와 고인슐린혈증을 중심 (Gerald Ravean; 1988 Syndrome-X) WHO정의가 광범위하게 사용되 고 있다
5,6)(modified NCEP ATP III기준을 적용하였다). 본 연구에서는
α-carotene,
β-carotene, lycopene, cryptoxanthine, lutein의 5가지 주요 carotenoids를 측정하였는데, 나이, 성, 흡연, 음주, 신체활동, 과일 및 야채섭취, 비타민 및 무기질제 제 복용 등을 보정하였다.
조사대상자의 대사증후군 유병율은 13.7% (남 13.16%, 여 14.61%)으로 다른 연구들과 유사하였으며, 여자의 유병율이 좀 더 높게 나타났으나 유의한 차이는 없었다 (p=0.629).
13)대 사증후군 요소가 있으면 carotenoids농도가 낮아진 것은 다른 연구 결과들과 유사하였고
13,14) β-carotene에서 항산화 작용이 뚜렷하였다.
15,16)복부비만과 중성지방에서 carotenoids와 관련 성이 상대적으로 많은데, 대사증후군에서 복부비만이 가장 중요한 요인으로 여겨지는 바와 같다.
17,18)특히,
β-carotene는 복부비만과의 상관성이 크고 복부비만이 있는 대사증후군에 서 농도가 가장 낮게 측정되어서
β-carotene을 대표적인 산화 스트레스 지표로 추정하는 다른 연구들
19,20)과 비슷하였다.
산화스트레스, 항산화제와 대사증후군, 심혈관질환 사이의 관련성은 여러 연구들에서 보고되며
21,22), 심혈관질환의 기전은
혈관내막의 손상 및 기능장애, 저비중콜레스테롤의 침착 그리 고 저비중지단백 함유 탐식세포가 동맥평활근층으로 이동하는 과정을 통해서 동맥경화가 진행하는데, 여기에 대사증후군 요 소들과 항산화물질들이 직. 간접적으로 관여한다.
20)즉, 유리활 성기에 의해 형성된 산화스트레스가 저비중지단백을 산화시키 고 (ox-LDL) 이를 탐식세포가 탐식하여 foamy세포로 되는 과 정에서 대사증후군 요소들은 유리활성기를 생성하는 산화스트 레스로 작용하며
18)항산화제는 유리활성기 생성을 억제하는 환 원제작용을 한다.
21,22)항산화제의 분류는 1) 항산화단백질 2) 세포내 항산화효소 3) 세포외 항산화물질로 분류할 수 있으며 세포외 항산화물질로는 carotenoids와 Vitamin C, E등이 있고, 이중에서 carotenoids는 지단백질의 산화적 변형을 차단하여 동맥경화를 예방하는 역할을 한다.
23,25)미국 영양조사 결과에 서도 대사증후군은 혈중 carotenoids, 비타민 C농도가 저하된 상태였으며, 식생활에서도 과일과 채소의 섭취가 적었다.
27)대사증후군이 산화스트레스를 유발하여 동맥경화를 악화시 키고, 항산화제는 산화스트레스 를 제거하여 동맥경화를 예 방하는 역할을 하여, 대사증후군이 진행하여 심혈관질환으로 귀착되는 원인-결과의 관계임을 알 수 있다. 따라서 대사증후 군과 혈중 carotenoids의 관련성은 산화스트레스, 대사증후군, 심혈관 질환 그리고 항산화제 사이의 관련성도 추정할 수 있
다.
10,11)본 연구에서도 위의 관련성 통계적 검정력은 낮았지
만 전반적으로 혈중 carotenoids는 대사증후군에 대한 예방 효과가 있었고
β-carotene이 대표적이었다 (다중 로지스틱회 귀분석에서 저농도군에서 대사증후군의 위험이 증가하였다;
교차비=5.3, 신뢰구간 2.16-13.26).
대사증후군에 대한 사회적 관심이 높아지는 이유는 대사증 후군이 해당되는 고위험군을 선별하여 생활습관 교정을 통한 위험인자 제거를 한다면, 최종적으로 심혈관질환 의 예방이 가 능하기 때문이다.
28)건강 생활습관 중에서 식이와 운동의 중요 성이 강조되며
29)사회적, 개인적 차원의 노력들이 시행해되고 있다. 이 중에서 약제의 형태로 항산화제를 추가하는 보충요법 도 많이 적용되고 있으며 그 효과에 대한 연구들도 다수 발표 되고 있다. 항산화 보충체 섭취에 대해서, 단면연구(역학적)에 서는 항산화제 혈중농도 증가와 건강수준 향상 사이에 관련성 이 있는 반면에 임상연구(보충제 투여)에서는 보충요법에 따른 암, 심혈관 질환등의 만성질환에 대한 예방효과는 소실될 뿐만 아니라 고위험군에서는 역효과를 초래하여 서로 상반되는 결 과를 보여주고 있다.
30,31)실험연구에서 carotenoids가 다량 보 충되었음을 감안하여 혈중농도가 역치(threshold) 이상에서는 오히려 역작용을 하기때문에, 충분한 식이 섭취 이상의 보충제 요법은 권장되지 않고 있다.
12)본 연구는 대사증후군-심혈관질환, 산화스트레스-항산화제
사이에서, 혈중 carotenoids와 대사증후군의 관련성을 알아보 고자 하였다. 항산화제와 심혈관질환에 관한 연구는 다수 있 지만 ‘혈중
β-carotene 농도 저하와 지방간에 대한 연구’
15)처 럼 질병 이전의 단계 즉, 대사증후군(1차, 2차 예방의 개입이 가능한 단계)과의 관련성에 관한 연구는 부족한 편이다. 대사 증후군 진단은 임상적용이 간단하여 예방적 개입을 위한 screening이 활성화되면 만성질환 예방에 많은 기여를 할 수 있다. 대사증후군을 이용한 위험도 추정이 일상적으로 가능 하기 위해서 더 이상의 연구가 필요하다.
본연구의 제한점으로는 첫째, 병원검진자료이고 대상자 수 가 충분하지 않아서 일반화하기에는 대표성이 부족하고, 둘 째, 단면연구여서 원인-결과에 대한 추론이 어려운 점과 셋 째, 대사성질환에서 유전적 감수성이 중요한데 여기에 대한 개인적 차이가 고려되지 못한 점 등이 있다.
요 약
연구배경
항산화제인 carotenoids와 심혈관질환 위험인자인 대사증 후군의 관련성을 알아보고자 하였다.
방 법
2005년 9월-12월 사이, 일개 대학병원에서 40세 이상의 검강 검진 수검자 533명을 대상으로 대사증후군 및 위험요소에 따른 혈중 carotenoids 농도를 비교하고 (ANCOVA), carotenoids 농 도가 대사증후군에 미치는 영향을 분석하였다(multiple logistic regression analysis). 통계분석은 SPSS 12.0을 이용하였으며, carotenoids 측정값은 나이, 성별, 흡연, 음주, 육체적 활동량, 과 일 및 채소의 섭취량, 비타민 및 미네랄 보충제 복용량에 대해 보정하였다.
결 과
대사증후군에서 일부 혈중 carotenoids의 농도가 저하되었다 (p<0.05).
β-carotene은 대부분의 대사증후군 항목에서 유의한 농도 저하를 보이고(p<0.05) 대사증후군 항목 수 증가에 따른 음의 용량- 반응 관계가 있었으며(p<0.01),
β-carotene농도 1사분위에서 대사 증후군의 위험도가 5.35배 증가하였고(p<0.01). 복부비만이 동반된 대사증후군에서 농도가 가장 낮았다(p<0.01). 혈중 carotenoids 농도는 남자가 여자보다 낮게 측정되었다(Lutein 제외).
결 론
본 연구에서 carotenoids는 대사증후군을 예방하는 경향을 보이었으며 특히,
β-carotene에서 유의하였다.
중심단어
carotenoids, 대사증후군
참고문헌
1. Song JH, Kim EK, Shin C, Kim SS, Kim JK, Jung MH, et al. Metabolic syndrome and its alternative definition for prevalent diabetes mellitus in Korean population; The Ansan study. Korean J Lipidol.
2003;13(1):9-12.
2. Earls S, Wane H. Prevalence of the metabolic syndrome among US adults: Findings from the third national health and nutrition examination survey. JAMA. 2002;287(93):356-359.
3. Qing Q, Weoguo G, Lei Z, et al. Metabolic syndrome and cardiovascular disease. Ann Cli Biochem. 2007;44:232-63.
4. Yamamoto A, Temba H, Horibr H, Mabuchi H, Saito Y, Matsuzawa Y, et al. Life style and Cardiovascular risk factors in Japanese population-from an epidemiologic survey on lipid levels in japan 1990 part: influence of Life style and excess body weight on HDL cholesterol and other lipid parameters in men. J of Atheroscler Thromb. 2003;10:165-75.
4. Choi KM, Lee JS, Park HS, Baik SH, Choi DS, Kim SM. Relationship between sleep duration and the metabolic syndrome: Korean National Health and Nutrition Survey 2001. Int J of Obesity. 2008;32(7):1091-97.
5. Grundy GM. Obesity, metabolic syndrome and cardiovascular disease. J Clini Endocrinol Meta. 2004;89:2585-600.
6. Ford ES, Giles WH, Dietz WH. Prevalence of metabolic syndrome among US adults; findings from National Health and Nutritional Examination Survey. JAMA 2002;287:356-359.
7. Reaven GM. Role of insulin resistance, Diabetes. 1988;37:1595-607 8. Christos P, Demostenes P, Michael W, Chrostdolous S. Diet, Exercise
and the Metabolic syndrome. Rev Diabetic Stud. 2006;3:118-26.
9. Han JH, Choi YE. Metabolic Syndrome and Oxidative Stress, Antioxidants. Korean Journal of Family Medicine. 2006;27:773-781 10. Charambos A, Dimitris T, Costas T, Palvos T, Christodoulous S.
Oxidative stress, Antioxidant Vitamins, and Artherosclerosis. Herz.
2003;28:628-38.
11. Cherubini, A. Vigna, G. B. Zuliani, G. Ruggiero, C. Senin, U. Fellin,
R.. Role of Anti-Oxidants in Atherosclerosis: Epidemiological and Clinical Update. Preview Current Pharmaceutical Design. 2005;
11(6):2017-2032.
12. Paiva SA, Russell RM. Beta-carotene and other carotenoids as antioxidants. J Am Coll Nutr. 1999;18(5):426-433.
13. Kim BS, Prevalence of metabolic syndrome; among the clients of comprehensive medical examination center in one university hospital. Korean J Heath Promot Dis prev. 2001:2;17-26.
14. Lean ME. Han TS, Morison CE, Waist circumference as a measure of indicating need for weight management. BMJ 1995;311:158-61.
15. Witte K. Clark A. Cieland J. Chronic heart failure and micronutrient.
J of the American College of Cardiology. 2001;37(7);1765-74.
16. Park SK, Lee HJ, Lee DH, Lee SK, Chun BY, Kim SA, et al. Association of Non Fatty Liver with the metabolic Syndrome and serum carotenoids. J Prev Med Public Health.2008;4:(1):39-44.
17. Ford ES, Mokdad AH, Giles WH, Brown DW, The metabolic syndrome and antioxidant concentrations: findings from the Third National Health and Nutrition Examination Survey. Diabetes.
2003;52(9):2346-52.
18. Evans RW, Shaten J, Day BW, et al. Prospective association between lipid soluble antioxidants and coronary artery disease in men. The Multiple Risk Factor Trial. Am J Epidemiology. 1998;147:180-6.
19. Kardinal AFM, Kok FJ, Ringstad J, et al. Antioxidants in adipose tissue and risk of myocardial infarction: EURAMIC study. Lancet.
1993;342:1979-84.
20. Ross R. The pathogenesis of atherosclerosis: A prospective for the 1990s. Nature. 1993:362:801-9.
21. Price JF. Fowkes FGR. Antioxidant vitamins in the prevention of cardiovascular disease: epidemiologic evidence. Eur Heart J.
1997;18:719-21.
22. Nuttal SL. Kendall MJ. Martin U. Antioxidant therapy for the prevention of cardiovascular disease. QJ Med. 1999.92:239-44.
23. Rice-Evans CA. Diplock AT. Current status of antioxidant therapy.
Free Radic Biol Med. 1993;15:77-96.
24. Earl S. Ford, Ali H. Mokdad, Wayne H. Giles, David W. Brown.
The Metabolic Syndrome and Antioxidant Concentrations. Diabetes.
2003;52:2346-52.
25. Shigetada F, Takuya F, Michio S, Masanori I, Yukio Y, Yoshimitsu N, et al. Increased oxidative stress in obesity and its impact on metabolic syndrome. J of Clinical Investigation. 2004;114(12):1752-61.
26. Boris H, Philppe G, Estelle N, Sandrine C, Eric BM, Jhon C, et al. Metabolic Syndrome is Associated with Elevated Oxidative Stress and Dysfunctional Dense High-Density Lipoprotein Particles Displaying Impaired Antioxidative Activity. J of Clini Endocrinology
& Metabolism. 2004;89(10):4964-71.
27. Christos P, Demostenes P, Michael W, Chrostdolous S. Diet, Exercise and the Metabolic syndrome. Rev Diabetic Stud. 2006;3:118-26.
28. Steven AE, Madeleine FD, Kantilal BP, Susan M, Subhas CK, Robin LW. Scavenging of Nitrogen Dioxide, Thiyl, and Sulfonyl Free Radicals by the Nutritional Antioxidant β-Carotene. J of Biological Chemistry. 1996;271(8):3988-94.
29. Lyn Patrick, ND. Beta-Carotene: The Controversy Continues.
Alternative Medicine Review. 2000;5(6):530-545.
30. Deepak PV, Marc SP, Shelly KS, Amy H, Eric JT. Use of antioxidant vitamins for the prevention of cardiovascular disease: meta-analysis of randomized trials. The Lancet. 2003;361:2017-23.
31. Charles HH, Julie EB, Joann EM, Meir S, Bernard R., Nancy C, et al. Lack of effect of long-term supplementation with beta carotene on the incidence of malignant neoplasms and cardiovascular disease.
The New England Journal of Medicine. 1996;334(18):1145-49.