대한견・주관절학회지 제1권 제1호 J. of Korean Shoulder・Elbow Society Vol. 1. No. 1. M a r c h , 1 9 9 8
※통신저자 : 김 승 호
서울특별시 강남구 일원동 5 0번지
성균관대학교 의과대학 삼성서울병원 정형외과 Rotator cuff lesions are a frequent cause of pain and disability in the shoul- der, and a number of publications have contributed to the knowledge about the pathogenesis, diagnosis, and treatment of rotator cuff tears4 - 8 , 1 1 , 1 3 - 1 5 , 2 1 )
. Neer1 5 )d e s c r i b e d three stages of rotator cuff lesions. Stage
Ⅰ includes hemorrhage and edema of the tendon, stage Ⅱ, tendinitis and fibrosis,
and stage Ⅲ, incomplete or complete tear- ing of the rotator cuff. This concept of a progressive evolution of the rotator cuff pathology has been widely accepted, Also, the role of mechanical impingement of the tendon under the anterior acromion has been the commonly held view.
However, little information is available on partial-thickness rotator cuff tearing.
Arthroscopic Treatment of Partial-thickness Rotator Cuff Tear
Seung-Ho Kim, M.D., Kwon-Ick Ha, M.D., Ph.D.
Department of Orthopaedic Surgery, College of Medicine, Kyun Kwan University, Samsung Medical Center, Seoul, Korea
Forty-nine partial thickness rotator cuff tears underwent arthroscopic debridement or repair, and were followed up for a minimum of two years. Follow-up evaluations of the results were completed using a detailed functional ques- tionnaire which was comprised of a rating of the UCLA shoulder scale and return to the previous sports activity and job. The average age of the 49 study patients was 46.5 years(range, 14 to 67 years). The patients were divided into four groups on the basis of the onset of the patient’s symptoms. Thirty-five patients(72%) had partial tearing only on the articular surface, six(12%) on the bursal surface, and eight(16%) on both surfaces. Group I consisted of 21 patients with an average age of 56.7. Partial tearing in group I was attributed to the impingement syndrome. In group II, partial tearing of the rotator cuff was related to the anterior instability of the shoulder. This group included 9 patients with an average age of 27.9. In group III, all of the 8 patients were overhead athletes with an average age of 21.8. In this group, no isolated instances of significant trauma were related to the development of the shoulder pain.
In group IV, 11 patients noted that a significant traumatic event preceded the onset of their pain. The average age of the patients was 34.9. Overall, 82% of the patients demonstrated satisfactory results and 18% revealed unsatisfactory results. The worst UCLA score and rate of return to the prior activity was noted in group III. In conclusion, partial thickness rotator cuff tear can be caused by subacromial impingement, instability, repetitive microtrauma, and macrotrauma. Arthroscopic debridement of partial tear of the rotator cuff provides a favorable outcome except in overhead athletes.
Key Words : Rotator cuff tear, Partial-thickness, Arthroscopic treatment
This lack of information is due in part to the difficulty of the diagnosis itself. As the majority of partial-thickness tears occur on the articular surface, the tears are not easily visible during open surgical acromioplasty, and in addition, adjunctive imaging such as arthrography, magnetic resonance image, or ultrasonography is often inadequate to detect a small articu- lar surface tearing. Even though arthros- copy has worked most effectively in the diagnosis of partial-thickness tearing, only a few investigators have described the etiologic factors of partial tearing other than Neer’s impingement3 , 7 ). The purpose of this study was to review our experience with arthroscopically diagnosed partial-thickness rotator cuff tears. The emphasis of this article includes pathome- chanisms of different etiologic groups of partial tearing.
M ATERIALS AND METHODS
Between October 1994 and June 1996, 54 partial thickness rotator cuff tears were treated at the Samsung Medical Center. Forty-nine of these patients were available for a minimum follow-up of two years. The selection criteria was a thick- ness rotator cuff tear, either on the artic- ular or bursal surface. Patients who had glenohumeral arthritis, adhesive capsuli- tis, prior surgery on the shoulder, or pre- vious infection were excluded from this study. The patient’s records, including history, physical findings, mechanism of injury, preoperative evaluation and opera- tive treatment were reviewed. Follow-up evaluations of the results were completed using a detailed functional questionnaire which was comprised of a rating on the
UCLA shoulder scale and return to the previous sports activity or job.
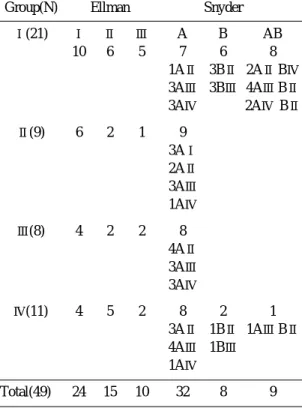
The average age of the 49 study patients was 46.5 years(range, 14 to 67 years). Eleven patients were female and 38 male. The dominant arm was involved in 35 patients and the nondominant arm in 14. The patients were followed up for a minimum of 2 years with the average fol- low-up being 30.1 months(range 24 to 44 months). The duration of symptoms aver- aged 39.4 months(range, 6 to 192 months). Thirty-five patients(72%) had partial tearing only on the articular sur- face, six(12%) on the bursal surface, and eight(16%) on both surfaces. The degree of involvement was classified using the E l l m a n’s and Snyder’s grading system and summarized in Table 1. Treatment of the partial-thickness tear was either arthro-
Table 1. Grade of Cuff tear
Group(N) Ellman Snyder
Ⅰ(21) Ⅰ Ⅱ Ⅲ A B AB
10 6 5 7 6 8
1AⅡ 3BⅡ 2AⅡBⅣ 3AⅢ 3BⅢ 4AⅢBⅡ
3AⅣ 2AⅣ BⅡ
Ⅱ(9) 6 2 1 9 3AⅠ 2AⅡ 3AⅢ 1AⅣ
Ⅲ(8) 4 2 2 8 4AⅡ 3AⅢ 3AⅣ
Ⅳ(11) 4 5 2 8 2 1
3AⅡ 1BⅡ 1AⅢBⅡ 4AⅢ 1BⅢ
1AⅣ
Total(49) 24 15 10 32 8 9
scopic debridement of the torn cuff ten- don or arthroscopic repair of the large flap of the tendon depending on the size of the tear. All grade Ⅰ lesions in the E l l m a n’s system were debrided and grade
Ⅱ lesions were debrided when the flap had frayed and fibrillated, or repaired arthroscopically if the lesion had a signifi- cant large flap. All grade Ⅲ tears were repaired arthroscopically.
The patients were divided into four groups on the basis of the onset of the their symptoms. Group Ⅰ consisted of 21 patients. The etiology of the partial tear- ing of group Ⅰ attributed to the impinge- ment syndrome. The average age of the group Ⅰ patients was 56.7 years(range 37 to 67 years), consisting of 13 males and 8 females. In group Ⅱ patients, partial tearing of the rotator cuff was related to the anterior instability of the shoulder.
This group included 9 patients, consisting of 8 males and 1 female. The average age of the patients was 27.9 years(range, 18 to 38 years). In group Ⅲ, all of the 8 patients were overhead athletes, either at the professional or collegiate level. All patients were male with an average age of 21.8 years(range, 18 to 24 years). Four patients were professional baseball play- ers, including two pitchers. One patient was a professional badminton player and three were collegiate tennis players. In this group, no isolated instances of signif- icant trauma were related with the devel- opment of the shoulder pain. In group Ⅳ, all patients noted that a significant trau- matic event preceded the onset of their pain. This group consisted of 11 patients with 9 males and 2 females. The average age of the patients was 34.9 years(range, 14 to 59 years). Two of these patients
were actively involved in athletic activi- ties at a recreational level. One was a ski coach and the other, a water skier. The other 9 patients were not involved in ath- letics on any regular basis.
SURGICAL TECHNIQUES
After the induction of general anesthe- sia, the patient was placed on the operat- ing table in the lateral decubitus position.
Standard arthroscopic portals were made and a complete diagnostic examination was performed. Viewing from the posteri- or portal, partial thickness tears were debrided by using a full radius synovial resector which was introduced through the anterior portal. When the partial- thickness tear of the articular surface had a large flap, only the margin of the flap was debrided, and then arthroscopic repair was performed. Viewing from the posterior portal, an additional anteroinfe- rior portal was made just proximal to the subscapularis tendon. An 18-gauge spinal needle was inserted into the supraspinatus tendon, just lateral to the anterior acromion, so as to pierce the intact ten- don and the torn flap. A Shuttle-Relay (Linvatec, Zimmer) was introduced through the spinal needle and the end of the Shuttle-Relay was retrieved from the joint out of the anteroinferior portal. A nonabsorbable suture(No 2 Ethibond) was loaded in the eyelet of the Shuttle-Relay, and the other end of the Shuttle-Relay was pulled with the suture. A second 18- gauge spinal needle was inserted about 1
㎝ apart from the first needle in order to pierce the intact tendon and the flap.
Then, a second Shuttle-Relay was intro- duced and retrieved out of the anteroinfe-
rior portal. The other end of the nonab- sorbable suture at the anteroinferior por- tal, was loaded into the eyelet of the Shuttle-Relay, and the Shuttle-Relay was pulled back out of the skin just lateral to the anterior acromion. Subacromial bur- soscopy was performed and the nonab- sorbable suture was tied using the slip knot technique. When the subacromial bursa was inflamed, arthroscopic bursec- tomy and anterior acromioplasty were performed. Viewing from the posterior subacromial portal, an electrocautery was introduced through the lateral portal, thickened soft tissue on the under surface of the anterior acromion and coracoacro- mial ligament were morcellated. A 5-㎜
cylindrical burr(Vortex, Linvatec) was introduced through the lateral subacromi- al portal and the lateral margin of the anterior one-third of the acromion was thinned. A trough about 1㎜ deep, was created from the posterior end of the acromioclavicular joint to the lateral mar- gin of the acromion and was used as a reference line for the following procedure.
An arthroscope was inserted through the lateral portal, and the burr through the posterior portal. Beginning from the ref- erence trough, the undersurface of the anterior acromion was resected. The thickness of resection was checked using the tip of the burr. When osteophytes on the undersurface of the distal clavicle were noted, partial resection of the distal 1㎝ of the clavicle was performed concur- rently. Any fraying or tearing on the bursal surface of the rotator cuff was debrided. After skin closure and dressing, an arm sling with pillow(Ultrasling, DonJoy) was applied
R E H A B I L I TAT I O N
When the patient was seen for the first time in the outpatient clinic, conservative treatment initiated. Conservative treat- ment included nonsteroidal anti-inflam- matory medication, local steroid injection into the subacromial space, and a home- therapy rehabilitation kit, or a regular basis hospital cuff rehabilitation program.
Conservative treatment was continued for at least 6 months, before consideration of operative intervention. When symptoms persisted after the adequate period of con- servative treatment, arthroscopic treat- ment was planned. After the arthroscopic debridement or repair, an immediate rehabilitation program was initiated, which included cold pack massage during operation day, passive range of motion from the second day, and progressive strengthening of the rotator cuff muscle.
The patient was educated on how to use the home-therapy-kit preoperatively and encouraged to use the kit daily. When the patient had severe resting pain, especially at night, and motion limitation, PCA (patient-control-anesthesia) was induced in the recovery room after the operation.
These patients felt comfortable during the early period after the operation and could initiate the regular rehabilitation program with minimal pain.
When the partial-thickness tears were repaired, only gentle pendulum and pas- sive motion exercises with rope and pulley were permitted for 3 weeks after the operation. Gentle strengthening exercises were added from the fourth week for the internal and external rotation of the arm at the side position. Athletic activities
such as throwing and serving a ball was started 6 months after the operation.
S TAT I S T I C S
Statistical analyses were performed with the SPSS software package(SPSS for win- dows Release 7.51, SPSS Inc USA). Dun- c a n’s multiple range test was performed to determine the differences in results between each group. Pearson’s rank corre- lation coefficient was calculated to deter- mine the relationship between the final result and the various parameters, such as patient group, grade of partial-thickness tear, severity of trauma, age of patient, sex, sports activity, selection of treatment, dominance of arm and type of acromion.
All analyses were set at 95% confidence interval for statistical significance.
R ATING SYSTEM
The UCLA shoulder rating system was used to evaluate the final results of the patients. The rating system evaluates the pain, function, active forward flexion, strength of forward flexion, and satisfac- tion of the patient. The maximum score on the rating system is 35 points. Excel- lent(34-35) or good(28-33) scores are deemed as satisfactory and fair(21-27) or poor(0-20) are rated as unsatisfactory.
The pain score was also graded using the analog scale from 0 to 10. Return to the previous job or level of athletic activity was evaluated using four grades. Grade 0 represented no limitation of athletic activ- ities and a complete return to prior job.
Grade Ⅰ was mild limitation in athletic activities and return to prior job. Grade
Ⅱ was rated when the patient had mod-
erate to severe limitation of their athletic activities or moderate limitation to the job even though the patient continued prior job or sports activities. Grade Ⅲ r e p r e- sented complete inability to return to prior athletic activities or previous job.
Grade 0 and Ⅰ were classified as favor- able returns, while grade Ⅱ and Ⅲ w e r e classified as unfavorable returns. We put an emphasis on the grade of returning to prior job or athletic activity for the evalu- ation of the final results. After all, because the return to the prior level of job or activities reflects a more functional condition of the patients after the treat- ment and is also a goal of the treatment i t s e l f .
R E S U LT S
Clinical findings
In group Ⅰ, all of the twenty-one patients revealed clinical findings consis- tent with the impingement syndrome.
The average age of the patients was 56.7 years with the range being 37 to 67.
There were 13 males and 8 females.
Using the Ellman’s grading system for this group, there were included 10 grade
Ⅰ’s, 6 grade Ⅱ’s, and 5 grade Ⅲ’s . History of minor trauma was recalled in 11 of the patients. But the traumas in these patients were not associated with the onset of the symptoms. No trauma was discovered in the remaining 10 patients. The dominant arm was involved in 13 patients while the nondominant arm was involved in 8. Seven patients demon- strated only an articular surface tear(one AⅡ lesion, 3 AⅢ lesions, 3 AⅣ lesions), 8 patients demonstrated partial tearing on both the articular and bursal surfaces(2 A
ⅡBⅣ lesions, 4 AⅢBⅡ lesions, 2 AⅣBⅡ lesion). And 6 patients had only bursal surface tears(3BⅡ, 3BⅢ). All patients had a positive impingement sign. In all of the group Ⅰ patient, subacromial space revealed severe thickening of the inflamed bursa and multiple osteophytes in the undersurface of the anterior acromion and acromioclavicular joint. Additional find- ings included a type Ⅰ superior labral anterior to posterior(SLAP) lesion in 3 patients, and a type Ⅱ SLAP lesion in 3 patients. None of the patients were involved in any rigorous sports activity.
No patient revealed more than a grade Ⅰ anterior translation under general anes- thesia. Radiographs of the shoulder revealed curved anterior acromion in 11 patients, a hook-like anterior acromion in 8 patients, and a flat acromion in 2.
Arthroscopic subacromial decompression was performed in all patients. Fifteen patients underwent arthroscopic debride- ment for the tear, and 6 patients recieved arthroscopic repair to the torn flap of the rotator cuff.
In group Ⅱ, all of the nine patients, 8 males and 1 female, had recurrent anteri- or instability of the shoulder. The average patient age was 27.9 years(range, 18 to 38 years). The dominant arm was involved in 7 patients. In this group, the partial tear occurred on the articular sur- face in all patients. According to Ellman’s classification of the tears, there were 6 grade Ⅰ’s, 2 grade Ⅱ’s, and 1 grade Ⅲ lesion. In Snyder’s classification system, there were 3 AⅠ’s, 2 AⅡ’s, 3 AⅢ’s, and 1 AⅣ lesion. All but one patient recalled a significant traumatic event in the ini- tial dislocation of the shoulder. All patients revealed a Bankart lesion and
one patient had a type Ⅱ SLAP lesion.
Impingement sign Ⅰ was positive in 4 patients while negative in 5. The subacro- mial space revealed a normal bursa, except in 2 patients with mild inflamma- tion of the bursal tissue. No patient had a significant spur on the undersurface of the anterior acromion. Radiographs demonstrated flat acromion in 6 patients and curved acromion in 3 patients. There was no hook-like anterior acromion.
Arthroscopic Bankart repair was per- formed on all patients using the suture anchor technique. Arthroscopic debride- ment of the tear was performed in 8 of the patients, and arthroscopic repair of A
Ⅳ lesion in 1 patient. No patient under- went subacromial decompression. In this group, 3 patients had been involved in athletic activities. These included tennis, basketball, and soccer, but at the recre- ational level.
Group Ⅲ included 8 male patients with an average age of 21.8 years(range, 18 to 24 years). All patients were overhead ath- letes, either at the professional or colle- giate level. Four patients were professional baseball players, including two pitchers.
One patient was a professional badminton player and three were collegiate tennis players. No isolated instances of signifi- cant trauma was recorded for this group.
Although one of the patients demonstrated a minor traumatic event, the onset of the pain was not associated with this trau- matic event. Most of their shoulder pain developed while either serving or throwing a ball. The average period of participation of overhead athletic activity for these patients was 11 years(range, 7 to 16 years). These patients revealed a grade Ⅰ lesion in 4, grade Ⅱ lesion in 2, and a
grade Ⅲ lesion in another 2 under Ellman`s system. All tears occurred on the articular surface of the rotator cuff at the insertion area. The supraspinatus was involved in 6 and infraspinatus in 2 patients. According to Snyder’s classifica- tion, four patients had AⅡ lesions, three had AⅢ lesions, and one had an AⅣ lesion. In one patients, however the pos- terosuperior labrum demonstrated a flap tear. No patient, except one, demonstrat- ed a sign of anterior instability of the shoulder such as a Bankart lesion, Hill- Sachs lesion, or anterior capsular tearing.
One collegiate tennis player who had a posterosuperior labral tear demonstrated a patulous anterior capsule. Upon physical examination under anesthesia, he revealed a grade Ⅱ anterior translation. As well as an arthroscopic anterior capsular plication with a No-2 Ethibond suture, arthroscopic debridement of the labral flap and partial- thickness rotator cuff tear were per- formed. The dominant arm was involved in all patients. Impingement sign was pos- itive in 7 of the patients, but an impinge- ment test with injection of local anesthet- ics into the subacromial space did not sig- nificantly relieve the pain. The subacromi- al space demonstrated a moderately inflamed bursa in 2 patients, and were normal in 6. The bursal surface of the rotator cuff was normal in all patients.
Radiographs of these patients revealed flat acromion in 6 patients and curved in two.
The acromioclavicular joint was normal in the x-ray. No spur on the undersurface of anterior acromion was noted in the sub- acromial bursoscopy. In this group, the onset of pain was insidious and was not related to the impingement syndrome, sig- nificant traumatic event, or frank disloca-
tion of the shoulder. Arthroscopic debride- ment was performed in 6 patients and arthroscopic repair in 2 patients. Partial- thickness rotator cuff tear in this group is attributable to the chronic repeated micro- trauma to the rotator cuff which resulted in a tension overload in the follow-through phase of throwing, pitching, and serving of balls. The articular surface of the supraspinatus, which is relatively avascu- lar at the insertional area, yielded to a tensile force during the eccentric contrac- tion of the cuff in the follow-through p h a s e .
Group Ⅳ had 11 patients consisting of 7 males and 4 females. The average age of the patients was 34.9 years(range, 14 to 59 years). Four of these patients were actively involved in athletic activities(one ski coach, one water skier, one soccer player, and one wrestler). The other 7 patients were not regular athletes. All patients noted that a significant traumat- ic event preceded the onset of their pain.
These traumas consisted of a direct blow on the shoulder during falling in 5 patients, indirect impact during falling on the outstretched arm in 4 patients, sud- den traction injury of abducted shoulder while water skiing in one patient, and a twisting injury for the one wrestler. All patients experienced sharp, severe pain at the traumatic event and their pain decreased in severity in the days following the accident, but was never completely relieved. They did not recall any shoulder symptoms before the traumatic event.
E l l m a n’s grade Ⅰ lesion was found in four patients, grade Ⅱ in 5, and grade Ⅲ in two. Eight of the tears were founded on the articular surface, two were located on the bursal surface, and one had a tear
on both surfaces of the rotator cuff(AⅡ lesion: 3, AⅢ lesion: 4, AⅣ lesion: 1, BⅡ lesion:1, BⅢ lesion: 1, AⅢ BⅡ lesion: 1).
The dominant arm was involved in 5 patients and the nondominant arm was in four. Impingement signs were positive in 3 patients. Radiographs of the shoulder revealed a flat acromion in 6 patients, a curved acromion in 4 patients, and a hooked acromion in one patient. The sub- acromial bursa was inflamed in 2 patients and a small spur was noted in one patient. The spur change was noted in a 59 year-old female who sustained a severe fall on the shoulder, otherwise she had no other previous history of shoulder pain before the index trauma. Associated find- ings of these patients included three type
Ⅱ SLAP lesions and one partial anteroin- ferior labral tear. Three patients from this group underwent an arthroscopic repair of the partial-thickness tear while the other had arthroscopic debridement.
Performed he type Ⅱ SLAP lesion was fixed with a suture anchor and the anteroinferior labral flap was debrided since it was small in size and not related with increased anterior translation under a n e s t h e s i a .
O U T C O M E
The patients were followed-up for an average of 30.1 months. Based on the UCLA scoring system, there were 29(59%) excellent, 11(23%) good, 6(12%) fair, and 3(6%) poor results. Overall, 82% of the patients demonstrated satisfactory results while 18% had unsatisfactory results (Table 2).
In 21 of the group Ⅰ patients, 16 revealed excellent, 3 good, one fair, and
one poor result. Overall, 90% of the patients were rated as having an excellent result in the UCLA score. Two patients (10%) with unsatisfactory results had E l l m a n’s grade Ⅲ tears, while another had S n y d e r’s AⅣ lesion and yet another had an AⅣBⅡ l e s i o n .
In 9 of the group Ⅱ patients, 5 patients demonstrated an excellent reult, 3 good, and one fair result. Overall, 89% of the patient were rated as having a satisfacto- ry result and 11% were rated as having unsatisfactory results. The patient with the fair result had an Ellman’s grade Ⅲ tear which is equivalent to a Snyder’s AⅣ l e s i o n .
In group Ⅲ, excellent results were recorded in one, good in 2, fair in 3, and poor in 2 patients. Overall, 38% of these patients were rated as having satisfactory results, while 62% were rated as having unsatisfactory results. One excellent result was recorded in the patient with E l l m a n’s grade Ⅰ tear, and two good results were recorded in Ellman’s grade Ⅰ and grade Ⅱ. Five unsatisfactory results occurred in Ellman’s grade Ⅱ or grade Ⅲ t e a r s .
In group Ⅳ, seven of the 11 patients revealed excellent results, 3 good, and one fair. Overall, 91% of them were rated as having satisfactory results. The one fair result occurred in Ellman’s grade Ⅱ w h i c h was Snyder’s AⅢ l e s i o n .
Table 2. UCLA score
Group(N) Excellent Good Fair Poor
Ⅰ00(21) 16(76%) 3(14%) 1(05%) 1(5%)
Ⅱ00(09) 05(56%) 3(33%) 1(11%)
Ⅲ00(08) 01(13%) 2(25%) 3(37%) 2(25%)
Ⅳ00(11) 07(64%) 3(27%) 1(09%) Total(49) 29(59%) 11(23%)0 6(12%) 3(6%)
D u n c a n’s multiple range test revealed that the percentage of unsatisfactory results was greater in group Ⅲ than the other group(p=0.18).
RETURN TO ACTIVITY
In 49 patients, 24(49%) returned to their prior jobs or sports activities with no limitations related to the shoulder(grade 0), while 25(51%) had some limitation returning their prior job or sports.
Thirteen(27%) out of 25 patients revealed some mild limitation(grade Ⅰ). Eight patients(16%) showed moderate to severe limitations in returning to the prior level even although there was no change in job or sports. Four patients(8%) failed to return to the prior job or sports due to the shoulder pain. Overall, 76% of the patients demonstrated a favorable return and 24% an unfavorable return. The best returns was recorded in group Ⅱ p a t i e n t s , while the worst returns were in group Ⅲ patients. Six(75%) out of 8 patients in group Ⅲ demonstrated unfavorable return. Return to the prior job and sports are summarized in Table 3.
No patient had returned completely to the prior level. Only two patients in group Ⅲ had a grade Ⅰ return to the their prior level of sports activities. These two patients were collegiate tennis players who had Ellman’s grade Ⅰ tear in the
supraspinatus tendon, and were rated as having excellent and good results on the UCLA scoring system respectively.
One collegiate tennis player who had an excellent UCLA score complained of occa- sional pain during the serving motion. In 2 pitchers, the one who had Ellman’s grade Ⅱ tear revealed a fair score and a grade Ⅱ return to the activity, while the one who displayed an Ellman’s grade Ⅲ tear revealed a poor result and a grade Ⅲ return to pitching. The other two baseball players who had an Ellman’s grade Ⅰ a n d
Ⅱ tears showed a fair UCLA score and a grade Ⅱ and Ⅲ return to baseball respec- tively. One collegiate tennis player who had an Ellman’s grade Ⅰ tear and a good UCLA score, and one professional bad- minton player who had a grade Ⅲ t e a r and a poor score, revealed grade Ⅱ returns to the their respective sports a c t i v i t i e s .
C O R R E L ATION OF UCLA SCORE AND FUNCTIONAL RETURN WITH
VARIOUS FA C TO R S
The multiple linear regression method was used to evaluate the difference between the final results for the different groups. Group Ⅲ patients demonstrated a significantly lower UCLA score and func- tional return compared to the other groups. Pearson’s correlation coefficient for the patient group was highest in sev- eral various factors. The type of acromion sex, selection of treatment, associate SLAP lesion, stability, and arm domi- nance had less of an influence on the final UCLA score and functional return than did the differences of the groups of the patients.
Table 3. Return to Activity
Group(N) Grade O Ⅰ Ⅱ Ⅲ
I 00(21) 14(67%) 4(19%) 2(09%) 1(05%)
Ⅱ00(09) 06(67%) 3(33%)
Ⅲ00(08) 2(25%) 4(50%) 2(25%)
Ⅳ00(11) 04(36%) 4(36%) 2(18%) 1(09%) Total(49) 24(49%) 13(27%)0 8(16%) 4(08%)
In group Ⅲ, the UCLA score and func- tional return were related to the Ellman’s grade of rotator cuff tear. Patients with large cuff tears demonstrated lower UCLA scores and functional returns. In the other group, there was no significant correlation between the size of the cuff tear and UCLA score or functional r e t u r n .
D I S C U S S I O N
Since Neer’s description of rotator cuff disease, three stages of this extrinsic mechanical impingement of the rotator cuff under the anterior acromion has been accepted as the primary cause of cuff tearing. Subacromial decompression of the impinging area, either open or arthroscop- ically, provides a promising result and has been well proven by biomechanical ratio- n a l e .
However, most of the literature to date had been addressing the full thickness rotator cuff tear or the bursal surface tear. With the increased application of arthroscope in shoulder surgery, increased numbers of partial thickness rotator cuff tears in the articular surface has been recorded. Recently, other mechanisms for the rotator cuff tear have been postulat- ed. Walch et al.22 described impingement of the posterior superior glenoid rim against the articular surface of the rota- tor cuff during the abducted and exter- nally rotated positions of the shoulder.
This internal impingement plays a role of partial thickness rotator cuff tear on the articular surface.
Instability of the glenohumeral joint is also associated with an articular surface partial tear. Increased glenohumeral
translation causes elongation of the rota- tor cuff tendon beyond the physiologic limits and results in tendon failure.
Repetitive overhead athletes are prone to overuse and fatigue of the rotator cuff. Eccentric overloading during the throwing mechanism may result in intrin- sic failure of the tendon fiber of the cuff, which compromise the function of the cuff to hold the humeral head centered in the glenoid, resulting in secondary impingement and further cuff injury.
Also, acute trauma may also cause rota- tor cuff tear in the younger population.
The results of arthroscopic treatment of partial thickness rotator cuff varied according to the authors. Various factors, such as patient population, arthroscopic technique, and the size of the partial tear may influence the results of the treat- ment. Most of the literature exclude these factors. Recently Gartsman et al7 ). evalu- ated articular surface partial-thickness rotator cuff tears, in which they separat- ed the patients into three different groups based on the primary cause of the cuff tear. The impingement group comprised the largest portion of these patients, and were older in age than the other groups.
Overall, 88% of the patients had satisfac- tory results after the average follow-up of 32.3 months. In their series, no difference could be found among the three patient subgroups. This result is contradictory to our present study. The partial thickness rotator cuff tear in the present study was caused by four different etiologies. They were impingement, instability. tension overload, and trauma. The tension over- load group scored the worst final results in the UCLA score and return to activity.
These patients were young athletes who
were involved in repetitive overhead motion. In Gartsman’s series, the infor- mation about the patient’s activity in the subgroups is lacking7 ).
The UCLA scores were similar for the impingement, instability, and trauma groups. However, return to activity was observed best in the instability group (100%), followed by the impingement group(86% satisfactory return), and then the trauma group(72% satisfactory r e t u r n )
The final results of the UCLA score and functional return within the subgroup were related to the size of cuff tear.
Although we could not calculate the sta- tistical difference due to the small num- bers for each grade of cuff tear, the patient with the larger size of tear revealed a poorer outcome.
In conclusion, partial-thickness rotator cuff tear occur most commonly as an impingement of the rotator cuff into the anterior acromion. Cuff failure also occurs in relation to glenohumeral insta- bility, significant trauma of the shoulder, and tensile overload from repetitive over- head athletic activity. Arthroscopic debridement or repair of the partial tear provides favorable results except in the tension overload group. In this group, the majority of the patients proved to have unfavorable outcomes.
REFERENCES
01) Altchek DW, et al : Arthroscopic acromioplas- ty. Technique and results. J Bone Joint Surg Am 1990;72A: 1198-207.
02) Andrews JR, Broussard TS, Carson WG : Arthroscopy of the shoulder in the management of partial tears of the rotator cuff: a preliminary
report. Arthroscopy 1985;1:117-22.
03) Blevins FT, Hayes WM, Warren RF : Rotator cuff injury in contact athletes. Am J Sports Med 1996;24:263-267.
04 ) Ellman H : Shoulder arthroscopy: current indica- tions and technique. O r t h o p e d i c s 1 9 8 8 ; 2 : 4 5 - 5 1 . 05) Ellman H : Diagnosis and treatment of incom-
plete rotator cuff tears. Clin Orthop 1 9 9 0 ; 2 5 4 : 64-74.
06) Esch JC, et al : Arthroscopic subacromial decompression: results according to the degree of rotator cuff tear. Arthroscopy 1988;4:241-9.
07) Gartsman GM, Nilne JC : Articular surface partial-thickness rotator cuff tears. J Shoulder Elbow Surg 1995;4:409-415.
08) Hawkins RJ, Mohtadi N : Rotator cuff prob- lems in athletes, in DeLee JC, Drez D Jr(eds):
Orthopaedic Sports Medicine : Principles and Practice. Philadelphia, WB Saunders Company, 1994, pp 623-656.
09) Hawkins RJ, Morin WD, Bonutti PM : Surgi- cal treatment of full-thickness rotator cuff tears in patients 40 years of age and younger. Orthop Trans 17: 1024, 1993-1994.
10) Ltoi E, Tabata S : Rotator cuff tears in the ado- lescent. Orthopedics 16:78-81, 1993
11) Jerosch J, Muller T, Castro WM : The inci- dence of rotator cuff rupture:An anatomic study.
Acta Orthop Belg 57:124-129, 1991.
12) Jobe FB, Kritne RS : Shoulder pain in the over- head or throwing athlete. The relationship of anterior instability and rotator cuff impingement.
Orthopedic Rev 1989;28:963-75.
13) Ling SC, Chen CF, Wan RX : A study on vas- cular supply of the supraspinatus tendon. S u r g Radiol Anat 12:161-165, 1990.
14) Lohr JF, Uhthoff HK : The microvascular pat- tern of the supraspinatus tendon. Clin Orthop 254:35-38, 1990.
15) Neer CS : Anterior acromioplasty for the chron- ic impingement syndrome in the shoulder. J Bone Joint Surg 1972;54:41-50.
16) Nirschl RP : Shoulder tendinitis. Elbow and shoulder: American Academy of Orthopedic Surgeons Symposium on Upper Extremity Injuries in Athletes. St. Louis, Missouri:C.V.
Mosby Co., 1986:322-37.
17) Nirschl RP : Prevention and treatment of elbow and shoulder injuries in the tennis player. C l i n
Sports Med 1988;7:289-308.
18) Ogilvie-Harris DJ, Wiley AM : Arthroscopic surgery of the shoulder. J Bone Joint Surg Br 1986;68B:201-7.
19) Ryu RKN : Arthroscopic subacromial decom- pression: a clinical review. Arthroscopy 1 9 9 2 ; 8:141-7.
20) Snyder SJ, Pachelli AF, Del Pizzo W, Friedman MJ, Ferkel RD, Pattee G : Partial
thickness rotator cuff tears: Results of arthro- scopic treatment. Arthroscopy 1991;7:1-7.
21) Tibone JE, Elrod B, Jobe FW, et al : Surgical treatment of tears of the rotator cuff in athletes. J Bone Joint Surg 68A: 887-891, 1986.
2 2 ) Walch G, Liotard JP, Boileau P, Noel E : Poatero-suoerior impingement in the throwing athletes. L Shoulder Elbow Surg 1:238-245, 1992.