804
목 적: 대퇴 골두 연골하 스트레스 골절(subchondral stress fracture of the femoral head)은 드문 질환으로서 최근에 주로 부전 골절(insufficiency fracture)의 형태로 발생한 예들에 대해 보고되고 있다. 본 연구에서는 부전 골절 및 피로 골절(fa- tigue fracture) 형태로 발생한 스트레스 골절 환자의 임상적, 방사선학적 특징을 평가하였다.
대상 및 방법: 1998년 1월부터 2003년 4월 사이에 대퇴 골두 연골하 스트레스 골절로 진단 및 치료 받은 8명 10예를 대상 으로, 이들의 임상적 방사선학적 소견에 대해 평균 33개월 추시 결과를 평가하였다.
결 과: 피로 골절의 양상으로는 6명의 젊고 건강한 군인에게서 입대 후 5개월 이내에 발생하였고, 부전 골절의 양상으로는 1명의 노인과 1명의 골형성 부전증 환자에게 발생하였다. 1명을 제외한 모든 환자에서 대퇴 골두 무혈성 괴사의 위험 요 소 및 뚜렷한 선행 외상의 과거력은 있지 않았다. 최초의 단순 방사선 사진상 6명 7예에서 이상 소견이 관찰되었다. 이 중 4예에서 대퇴 골두의 함몰 소견이 관찰되었다. 골 주사 검사상 대퇴 골두에 증가된 흡수 음영 소견이 관찰되었다. 자기 공 명 촬영에서 대퇴 골두 연골하 이상 신호 선(MR crescent sign)과 전반적인 골수의 부종 소견이 관찰되었다.
결 론: 대퇴 골두 연골하 스트레스 골절은 부전 골절 및 피로 골절의 양상으로 모두 나타날 수 있으며, 의심되는 환자의 경 우 골 주사 검사 등을 통하여 조기 진단함으로써 대퇴 골두의 함몰을 방지할 수 있을 것이다.
색인 단어: 스트레스 골절, 연골하 골절, 대퇴 골두
Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul; Department of Orthopedic Surgery, Jeju National University, College of Medicine*, Jeju, Korea
Won Seok Song, M.D., Jong Won Kim, M.D., Jeong Joon Yoo, M.D., Kyung-Hoi Koo, M.D., Kang Sup Yoon, M.D., Sang Rim Kim, M.D.*, Young-Min Kim, M.D., and Hee Joong Kim, M.D.
Subchondral Stress Fracture of the Femoral Head
804
대퇴 골두 연골하 스트레스 골절
송원석ㆍ김종원ㆍ유정준ㆍ구경회ㆍ윤강섭ㆍ김상림*ㆍ김영민ㆍ김희중
서울대학교 의과대학 정형외과학교실, 제주대학교 의과대학 정형외과학교실*
804 804 통신저자 : 김 희 중
서울시 종로구 연건동 28
서울대학교 의과대학 정형외과학교실 TEL: 02-2072-2970∙FAX: 02-764-2718 E-mail: [email protected]
*본 논문의 요지는 2003년도 대한 정형외과학회 추계학술대회에서 발표되었음.
*본 연구는 한국인체기초공학 연구재단의 2002년도 연구비(KOHTERF-2002- 05) 지원으로 이루어진 것임.
Address reprint requests to Hee Joong Kim, M.D.
Department of Orthopedic Surgery, Seoul National University College of Medicine, 28 Yongon-dong, Chongno-gu, Seoul 110-774, Korea
Tel: +82.2-2072-2970, Fax: +82.2-764-2718 E-mail: [email protected]
Purpose: Subchondral stress fracture of the femoral head is a rare condition that usually occurs as an
insufficiency fracture in people with poor bone quality. This study evaluated the clinical and radiograph- ic aspects of the subchondral stress fracture of the femoral head that occurred in the form of an insuffi- ciency or a fatigue fracture.
Materials and Methods: Between January 1998 and April 2003, 10 cases of the subchondral stress
fracture of the femoral head in 8 patients were treated. The characteristics of this condition were deter- mined by assessing the clinical course and findings of the radiographs, bone scintigram and MR images.
Results: A fatigue fracture developed in 6 young healthy conscripts within 5 months after recruitment.
An insufficiency fracture developed in one senile patient and in one known osteogenesis imperfecta
patient. All patients except for one did not have any predisposing factors for osteonecrosis and
antecedent trauma. On the initial radiographs, femoral head collapse was observed in 4 hips. Bone
scintigraphs showed increased radionuclide uptake in the femoral head. The MR images demonstrated
an subchondral abnormal signal intensity line (MR crescent sign) and a bone marrow edema pattern.
스트레스 골절은 주로 천골, 대퇴 경부, 경골 간부, 중 족골 등에 빈번하게 발생하는 것으로 알려져 있다7,9,10). Egol 등3)은 젊은 연령에서 정상의 골이 반복적인 과부하 를 받아 생긴 스트레스 골절을 피로 골절(fatigue frac- ture), 노령에서 골다공증, 골연화증 등으로 인해 약화 된 골이 정상적인 부하를 받아 생긴 스트레스 골절을 부 전 골절(insufficiency fracture)이라 정의한 바 있다.
대퇴 골두 연골하 스트레스 골절(subchondral stress fracture of the femoral head)은 비교적 드문 질환으 로 최근에 자기공명 사진과 이와 비교한 병리 소견을 바 탕으로 이에 대한 증례 보고가 발표되고 있다1,16,19,20,22). 그러나 이들의 대부분은 노인 환자나 신장 이식술을 받은 환자에 있어서 부전 골절의 양상으로 발현한 경우에 국한 되고 있으며, 저자들이 문헌 고찰을 통하여 본 바로는 지 금까지 발표된 연구 중 젊은 군인들에게서 발생한 대퇴 골두의 스트레스성 골 병변(stress osteopathy)에 대한 논문이 하나 있을 뿐이다21).
본 연구에서는 부전 골절 및 피로 골절 형태의 대퇴 골 두 연골하 스트레스 골절의 임상적, 방사선학적 특징을 파악하고 조기 진단 및 감별 진단의 중요성에 대해 알아 보고자 하였다.
연구 대상 및 방법
1998년 1월부터 2003년 4월 사이에 대퇴 골두 연골하 스트레스 골절로 진단되어 치료 받은 8명의 환자 10예를 대상으로 하였다(Table 1). 이들은 군 입대 후 시행한 신 병훈련, 태권도 훈련이나 또는 일상 생활 중 심각한 외상 력 없이 고관절의 통증이 발생한 예들로서, 임상적 경과 와 단순 방사선 검사, 골 주사(bone scan) 검사 및 자기 공명 촬영(MRI)상 골절선이 확인되었고 무혈성 괴사의 소견과는 감별되는 특징적 소견을 바탕으로 진단하였고, 1명의 환자에서는 후향적으로 그리고 나머지 환자의 경 우에서는 전향적으로 관찰하였다.
이들은 남자가 7명 여자가 1명으로, 통증 발생 시 평균 나이는 32세(범위, 20-75)였고, 평균 신장은 171 cm (범 위, 155-180 cm), 평균 체중은 63 kg (범위, 47-78 kg) 이었다. 고관절 통증은 양측성인 환자가 2명이었고, 일측 성인 환자가 6명으로 일측성인 경우 우측이 4예, 좌측이 2예이었다.
단순 방사선 사진은 환자들이 고관절 통증이 있은 후 로부터 2주에서 6개월 경과 후 촬영하였고, 전후면 및 측면 방사선 사진을 얻었다. 골 주사 검사는 6명의 환자 에서 시행하였다. 자기 공명 사진은 다양한 기기를 사용 하여 촬영한 0.5-1.5T 범위의 사진이었고, 영상 기법은 Conclusion: A subchondral stress fracture of the femoral head can occur as a fatigue fracture as well
as an insufficiency fracture. Bone scintigraphy is a valuable tool for screening patients suspected of having a subchondral stress fracture.
Key Words: Stress fracture, Subchondral, Femoral head
*Time (x-ray), time to initial x-ray after pain development; �others, other MR images except T1-weighted image that show MR crescent sign; �FS, fat sup- pressed;‖Gd, gadolinium enhanced; ¶NWB, non weight bearing.
Pati- ent No.
Age (yr)/
Gender
Ht (cm)/
Wt (kg)
Previous event
Case
No. SideTime (mo) (x-ray)*
Initial x-ray finding
Time (mo) (MRI)
Bone scan
Duration of sx (mo) MR crescent sign Tx
T1 others�
1 22/M 180/78 training 1 R 3 collapse 3 low T2, low THA
2 L 3 radiolucent line 3 low T2, low drilling
2 21/M 171/70 martial art 3 R 2 radiolucent line 5 - FS�T2, high + 6 NWB
4 L 2 normal 5 low FS T2, high + 1.5 NWB
3 21/M 176/60 martial art 5 L 5 normal 5 low FS T1, low + 2 NWB
4 20/M 174/60 training 6 R 3 normal 3 low T2, low + 6 NWB
5 21/M 180/78 training 7 R 0.5 collapse 1 low Proton,low + bone graft
6 22/M 174/60 training 8 L 3 collapse 4 low T2, low 4 NWB
7 75/F 155/47 - 9 R 3 collapse 3 - T2, low + 4 NWB
8 52/M 158/53 heavy lift 10 R 6 osteoporosis 7 - Gd‖T1, high + drilling
Table 1.Patients data
T1-강조 영상, T2-강조 영상 및 프로톤 강조 영상 등이 사용되었다.
이들 환자들에 대하여 평균 33개월(범위, 6-68개월) 추시 기간 동안 이들의 임상 증세의 변화와 이와 연관하 여 단순 방사선 사진 및 자기 공명 사진을 촬영하여 변화 를 살펴보았다.
결 과
환자 군(Table 1)을 살펴보면, 1명의 환자(환자 7)는 특별한 기저 질환이 없는 비교적 건강한 75세의 노인 환 자로 특별한 수상의 과거력 없이 통증이 발생하였고, 1명
의 환자(환자 8)는 52세의 Sillence type Ⅳ의 골형성 부전증(osteogenesis imperfecta) 환자로서 30대 이 후로는 골절의 병력은 존재하지 않았으며 무거운 짐을 나 르는 일을 한 뒤 통증이 발생하였고 4년 전에도 비슷한 양상의 통증이 있었으나 수 개월 경과 후 자연적으로 호 전된 과거력이 있었다. 나머지 6명의 환자는 모두 20대 초반의 건장한 남자로서 신병 훈련 또는 태권도 훈련 도 중 발생한 고관절 통증을 주소로 군병원에서 대퇴 골두 무 혈성 괴사의 진단 후 전역 조치를 받은 환자들이었다.
골형성 부전증 환자 1명의 경우 음주의 과거력이 있었으 나 나머지 환자들에서는 음주나 부신 피질 호르몬 투여 등
A
B C
Fig. 1.Patient 1, cases 1 and 2. A 22-year-old man with bilateral hip pain. (A) AP and frogleg radiographs obtained three months after pain show that the right femoral head had collapsed. In the left femoral head, there is a radiolucent line (arrowhead). (B) AP and frog- leg (postoperative) radiographs obtained seven months after pain shows healing of the subchondral fracture with slight progression of the collapse in the left femoral head. (C) T1 and T2-weighted MR images (top) obtained at about the same time show a diffuse area of low signal intensity on the T1 image, which converted to iso/high signal intensity on T2 images (asterisk, bone marrow edema pat- tern). Linear low signal intensity bands (arrowhead, MR crescent sign) in subchondral area are shown on both images. Coronal T1 and T2-weighted MR images (bottom) obtained seven months after the onset of pain show the resolution of abnormal signal intensi- ty changes and the disappearance of the MR crescent sign.
* *
* *
T1
T2
T1
T2
의 대퇴 골두 무혈성 괴사의 위험 요소는 존재하지 않았다.
6명의 환자 7예에서, 최초 단순 방사선 사진상 뚜렷한 이상을 보였다. 이 중 4예에서는 대퇴 골두의 전상방에 붕괴 소견이 관찰 되었고(Fig. 1), 2예에서는 방사선 투 과성 선(radiolucent line)이, 1예에서는 골다공증 소견 이 관찰되었다. 나머지 3예에서는 최초 단순 방사선 사진 에서 뚜렷한 이상 소견은 보이지 않았다(Fig. 2). 시행된 골 주사 검사에서는 모두 대퇴 골두에 증가된 흡수 음영 이 관찰되었다.
최초의 자기 공명 촬영은 환자에 따라 통증 발생 후 1 개월에서 7개월 사이에 시행되었다. 병변은 1명(환자 2)
2예의 경우에서만 대퇴 골두의 후상방에 존재하였고, 나 머지 예에서는 모두 대퇴 골두의 전상방에 존재하였다.
자기 공명 사진상 공통적으로 T1-강조 영상에서 경계가 불명확한 부분적 또는 광범위한 저신호 강도(low signal intensity) 소견이 나타났으며, 이들은 T2-강조 영상 또는 지방 억제 영상(fat suppressed image)에서 고신 호강도(high signal intensity)로 전환되었다(골수 부 종 양상, bone marrow edema pattern). 또한 모든 예에서 연골하 골판(subchondral plate)에 평행하게 주 행하는 불규칙한 모양의 이상 신호 강도선(연골 하 골절 선, MR crescent sign)10,11)이 관찰되었다(Fig. 1-4).
Fig. 2.Patient 4, case 6. A 20-year-old man with right hip pain. (A) AP and lateral radiographs obtained three months after pain show no definite abnormality. Bone scan in the inset shows increased radionuclide uptake in the right femoral head. (B) T1 and T2-weight- ed MR images (top) show bone marrow edema pattern on the femoral head and neck area (asterisk). Fracture line (arrowhead) in the subchondral area is shown. T1 and fat suppressed T1-weight- ed images (bottom) obtained fourteen months after the onset of pain show the resolution of abnormal signal intensity changes.
* *
T1 T2
T1 FS T1
A
B
A B
Fig. 3.Patient 7, case 9. A 75-year-old woman with right hip pain. (A) AP and frogleg radiographs obtained three months after pain show slight collapse of the femoral head (arrowhead). (B) T1 and T2-weighted axial MR images show bone marrow edema pattern (asterisk) with fracture line (arrowhead).
T1 T2
*
이러한 이상 신호 강도 선은 7예에서는 T1-강조 영상에 서 저신호 강도의 소견으로 관찰되었고 다른 강조 영상에 서는 다양한 신호 강도로 나타났다. 나머지 3예에서는 각각 가돌리늄(gadolinium) 조영 T1-강조 영상, 지방 억제 T2-강조 영상과, T2-강조 영상에서만 연골하 골 절선이 관찰되었다(Fig. 3).
모든 환자들에 대해서 처음에는 비체중 부하의 보존적
치료를 시행하였다. 대퇴 골두의 붕괴 소견이 심하지 않 고 보존적 치료를 시행한 6예에서는 통증이 점차 완화되 었고, 6개월 뒤에는 모두 소실되었으며 추시 자기 공명 사진을 시행한 예에서(증례 1-6) 이와 상응하여 이상 소 견이 정상화되었다. 이들의 평균 통증 지속 기간은 4개월 (범위, 1.5-6개월)이었다. 다발성 천공술(multiple dri- lling)을 시행한 2예의 경우는 모두 시술 후 2개월 경과
A
C
E
B
D
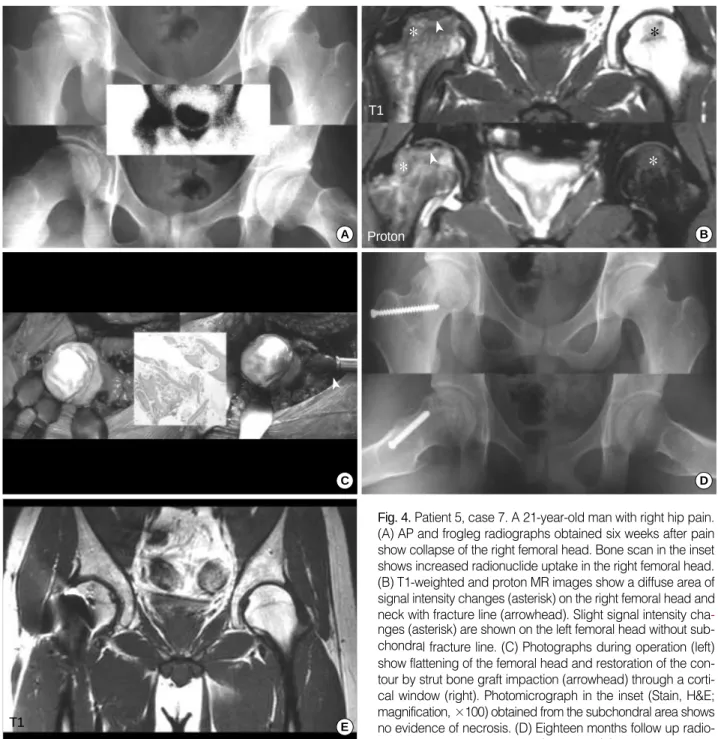
Fig. 4.Patient 5, case 7. A 21-year-old man with right hip pain.
(A) AP and frogleg radiographs obtained six weeks after pain show collapse of the right femoral head. Bone scan in the inset shows increased radionuclide uptake in the right femoral head.
(B) T1-weighted and proton MR images show a diffuse area of signal intensity changes (asterisk) on the right femoral head and neck with fracture line (arrowhead). Slight signal intensity cha- nges (asterisk) are shown on the left femoral head without sub- chondral fracture line. (C) Photographs during operation (left) show flattening of the femoral head and restoration of the con- tour by strut bone graft impaction (arrowhead) through a corti- cal window (right). Photomicrograph in the inset (Stain, H&E;
magnification, ×100) obtained from the subchondral area shows no evidence of necrosis. (D) Eighteen months follow up radio- graphs show no progression of collapse. (E) T1-weighted coro- nal MR image obtained twenty months after the onset of pain shows the resolution of abnormal signal intensity changes including the fracture line.
*
* *
*
T1
Proton
T1
후 통증의 소실을 나타냈다.
대퇴 골두의 붕괴가 심하였던 2예의 경우에 대해서는 각각 인공 고관절 전치환술과 지주 골 이식술(strut bone graft)을 시행하였다. 인공 고관절 전치환술을 시행한 환 자(환자 1)는 통증 발생 후 5개월이 경과하여 본 정형외과 를 방문하였다. 이 환자는 최초 대퇴 골두 무혈성 괴사로 진단하여 골두 붕괴가 심한 우측에는 인공 고관절 전치환 술을, 붕괴가 없는 좌측에는 다발성 천공술을 시행하였 다. 또 지주 골 이식술을 시행한 환자(환자 5)는 통증 발 생 후 6주만에 방문하였고, 최초 단순 방사선 사진과 비 교하여 붕괴가 진행되는 소견을 보였다. 이 환자에 대해 장골에서 채취한 지주 골을 대퇴 경부에 창을 내어 삽입 함으로써 대퇴 골두의 함몰을 다시 펼 수 있었고, 추시 사 진상 더 이상의 함몰은 관찰되지 않았다. 수술 시 얻은 연 골하 골 부위의 망상골 조각(cancellous bone chips) 의 조직 검사에서 무혈성 괴사의 소견은 관찰되지 않았 다(Fig. 4).
고 찰
1972년 Todd 등18)이 대퇴 골두 골소주(trabecular)만 의 피로 골절을 보고한 이후, 대퇴 골두 연골하 골의 스 트레스 골절에 대한 몇몇 보고1,2,16,20,22,23)가 있었으나 이 들 대부분은 부전 골절의 양상으로 발생한 예만을 포함 하고 있다. 본 연구에서는 부전 골절의 양상으로 발생한 2예(노인 환자 및 골형성 부전증환자)뿐만 아니라, 20대 의 젊은 군인에게서 발생한 피로 골절 양상의 스트레스
골절을 포함하고 있다.
연구 대상 환자들에 대한 진단은 기본적으로 일련의 자 기 공명 사진을 바탕으로 하였다. 최초 자기 공명 사진 상 골절선(fracture line) 및 골절선 주변의 골수 부종 양상 (bone marrow edema pattern) 소견을 관찰할 수 있 었으며, 이러한 소견은 추시 사진상 소실되었다. 그러나 이러한 골절 선은 모든 영상에서 관찰되지는 않았으며 일 부 절단면에서만 관찰할 수 있었다. 일찍이 Visuri21)는 자기 공명 사진상의 가역적인 골수 부종 소견을 바탕으로 10명의 군인에서 발생한 대퇴 골두의 스트레스성 골 병변 에 대해 기술한 바 있는데, 이는 대퇴 골두 연골하 골의 스트레스 골절이 젊고 건강한 사람에게서 피로 골절의 형 태로도 발생할 수 있음을 시사하는 것으로, 만약 좀더 해 상도가 좋은 자기 공명 사진을 이용하였더라면 골절선을 발견하였을 가능성이 있다.
골수 부종 양상은 고관절의 일과성 골다공증(transient osteoporosis of the hip)의 특징적인 자기 공명 사진 소견이다. 일과성 골다공증의 원인에 대해서는 아직 명 확하게 밝혀지지 않았으나 대퇴 골두 연골하 골절이 그 원인 중 하나일 것이라는 보고도 있다5,15). 본 연구의 경 우에 있어서도 4예의 경우 초기 단순 방사선 촬영상 뚜렷 한 골절 등의 이상소견이 관찰되지 않았으며 시간이 경과 됨에 따라 증세가 소실되는 것을 관찰할 수 있었다. 만약 이들의 경우에 자기 공명 촬영에서 골절선을 확인하지 못 하였더라면 고관절의 일과성 골다공증으로 진단되었을 것이다. 또한 Miyanishi 등13)은 고관절의 일과성 골다 공증으로 진단하였던 12예의 후향적 연구에서, 자기 공 명 사진상 연골하 골절선을 확인할 수 있었다고 보고하였 다. 이러한 연골하 골절선은 자기 공명 사진의 일부 절단 면에서만 확인할 수 있으므로, 일과성 골다공증으로 진 단하기 위해서는 여러 절단면에서 다양한 신호 강도로 얻 은 자기 공명 영상을 세심히 관찰하여 골절선이 없음이 확인되어야 할 것이다.
대퇴 골두의 연골하 골절 및 골수 부종 양상은 대퇴 골 두 무혈성 괴사의 경우에 있어서도 관찰되므로 스트레스 골절과의 감별이 용이하지 않을 수 있다. 본 연구의 환자 의 경우도 젊은 군인의 경우에는 모두 대퇴 골두 무혈성 괴사로 전역 조치를 받고 방문하였고, 첫째 환자의 경우 에는 본 병원에서도 최초에 대퇴 골두 무혈성 괴사로 진 단 후 치료하였던 경우로 후향적으로 본 연구의 대상으 Fig. 5.A typical case of osteonecrosis of the femoral head (ONFH).
Subchondral fracture (arrowhead) occurs inside the necrotic por- tion surrounded by a reactive line of an abnormal signal intensity (arrows). The bone marrow edema pattern (asterisk) is only shown outside the necrotic area.
*
* *
*
T1
T2
로 포함되었다.
대퇴 골두 무혈성 괴사의 경우, 괴사가 발생되면 우선 괴사 부위의 외연을 따라 재생 과정이 진행되어 소위 반 응 영역(reactive zone)이 형성되는데 이는 괴사 부위 측의 혈관이 풍부한 육아 조직과 그 외측의 신생골 형성 부위로 이루어지며, 자기 공명 사진상 T1-강조 영상에 서 저신호 강도의 띠(low signal intensity band), T2- 강조 영상에서는 double line sign으로 나타난다8,14,17). 이와 같은 괴사부 외연의 이상 신호 강도 띠는 무혈성 괴 사 시 가장 먼저 나타나는 자기 공명 영상 소견이다. 무혈 성 괴사 시 연골하 골절은 재생 과정이 어느 정도 진행한 후 괴사부의 내부에 발생하기 때문에4,6)자기 공명 사진 상 연골하 골절선 바깥쪽으로 반응 영역인 이상 신호 강 도 띠가 존재하며, 골수 부종 소견도 괴사부 바깥쪽에서 만 관찰된다(Fig. 5). 그러나 대퇴 골두의 연골하 골절의 경우에는 대퇴 골두 무혈성 괴사에서 보이는 저신호 강도 의 띠, 즉 괴사골 주변의 반응 영역이 관찰되지 않으며, 또한 골수 부종 양상이 골절선 인접 부위까지 나타난다19). 본 연구 대상자 중 6예에 있어서 단순히 체중 부하 보 행만을 억제하여 통증은 시간이 경과함에 따라 호전되었 고, 이와 더불어 추시 자기 공명 사진상 이상 신호 소견이 소실되었다. 이러한 시간 경과에 따른 임상적, 방사선학 적 호전 소견은 대퇴 골두 스트레스 골절의 특징적인 소 견으로 보고 되고 있다14,16,20). 그러나 본 연구의 2예 및 다른 보고의 경우에 나타나듯이 대퇴 골두 연골하 스트레 스 골절은 골두의 붕괴를 초래하여 수술적 치료를 필요로 할 수 있다.
대퇴 골두 연골하 스트레스 골절을 고관절 통증의 한 원인으로서 인식하는 것은 다른 질환과의 감별 진단 및 발병 후 추가적인 손상(골두 함몰)을 피할 수 있다는 점에 서 중요하다고 판단된다. 따라서 부전 골절 및 피로 골절 을 포함한 스트레스 골절이 대퇴 골두에도 발생할 수 있 다는 것을 염두에 두고, 고관절 부위의 통증을 호소하는 환자에 대한 감별 진단의 하나로 고려하여야 할 것이다.
특히 골 주사 검사는 의심이 가는 환자의 선별 검사로서 큰 도움이 될 것으로 생각된다.
결 론
대퇴 골두 연골하 골의 스트레스 골절은 부전 골절 및 피로 골절의 양상으로 나타날 수 있으며, 조기 진단 및 감
별 진단이 치료 및 예후의 측면에서 매우 중요할 것으로 판단된다.
참고문헌
1. Bangil M, Soubrier M, Dubost JJ, et al: Subchondral insuffi- ciency fracture of the femoral head. Rev Rhum Engl Ed, 63: 859- 861, 1996.
2. Buttaro M, Gonzalez Della Valle A, Morandi A, Sabas M, Pietrani M and Piccaluga F:Insufficiency subchondral fracture of the femoral head. Report of 4 cases and review of the literature. J Arthroplasty, 18: 377-382, 2003.
3. Egol KA, Koval KJ, Kummer F and Frankel VH: Stress frac- tures of the femoral neck. Clin Orthop, 348: 72-78, 1998.
4. Glimcher MJ and Kenzora JE: The biology of osteonecrosis of the human femoral head and its clinical implications. Ⅲ. Discus- sion of the etiology and genesis of the pathological sequelae. com- ments on treatment. Clin Orthop, 140: 273-312, 1979.
5. Karagkevrekis CB and Ainscow DA: Transient osteoporosis of the hip associated with osteogenesis imperfecta. J Bone Joint Surg, 80-B: 54-55, 1998.
6. Kim YM, Oh HC and Kim HJ: The pattern of bone marrow oedema on MRI in osteonecrosis of the femoral head. J Bone Joint Surg, 82-B: 837-841, 2000.
7. Kiuru MJ, Pihlajamaki HK and Hovuo JA: Fatigue stress in- juries of the pelvic bones and proximal femur. Evaluation with MR imaging. Eur Radiol, 13: 605-611, 2003.
8. Kubo T, Yamazoe S, Sugano N, et al: Initial MRI findings of non traumatic osteonecrosis of the femoral head in renal allograft recipients. Magn Reson Imaging, 5: 1017-1023, 1997.
9. Lassus J, Tulikoura I, Konttinen YT, Salo J and Santavirta S:Bone stress injuries of the lower extremity. a review. Acta Orthop Scand, 73: 359-368, 2002.
10. Maitra RS and Johnson DL: Stress fractures. Clinical history and physical examination. Clin Sports Med, 16: 259-274, 1997.
11. Mitchell DG, Joseph PM, Fallon M, et al: Chemical-shift MR imaging of the femoral head: An in vitro study of normal hips and hips with avascular necrosis. Am J Roentgenol, 148: 1159-1164, 1987.
12. Mitchell DG, Rao VM, Dalinka MK, et al: Femoral head avas- cular necrosis: Correlation of MR imaging, radiographic staging,
radionuclide imaging, and clinical findings. Radiology, 162: 709- 715, 1987.
13. Miyanishi K, Yamamoto T, Nakashima Y, et al: Subchondral changes in transient osteoporosis of the hip. Skeletal Radiol, 30: 255- 261, 2001.
14. Nakamura T, Matsumoto T, Nishino M, Tomita K and Ka- doya M:Early magnetic resonance imaging and histologic findings in a model of femoral head necrosis. Clin Orthop, 334: 68-72, 1997.
15. Noorda RJ, Van der Aa JP, Wuisman PI, David EF, Lips PT and van der Valk P:Transient osteoporosis and osteogenesis imperfecta. A case report. Clin Orthop, 337: 249-255, 1997.
16. Raffi M, Mitnick H, Klug J and Firooznia H: Insufficiency fracture of the femoral head: MR imaging in three patients. Am J Roentgenol, 168: 159-163, 1997.
17. Sakamoto M, Shimizu K, Iida S, Akita T, Moriya H and Nawata Y:Osteonecrosis of the femoral head: A prospective study with MRI. J Bone Joint Surg, 79-B: 213-219, 1997.
18. Todd RC, Freeman MAR and Pirie CJ: Isolated trabecular fa-
tigue fractures in the femoral head. J Bone Joint Surg, 54-B: 723-728, 1972.
19. Uetani M, Hashimi R, Ito M, et al: Subchondral insufficiency fracture of the femoral head: Magnetic resonance imaging findings correlated with micro-computed tomography and histopathology.
J Comput Assist Tomogr, 27: 189-193, 2003.
20. Vande Berg BC, Malghem J, Goffin EJ, Duprez TP and Mal- dague BE:Transient epiphyseal lesions in renal transplant recip- ients. Presumed insufficiency stress fractures. Radiology, 191: 403- 407, 1994.
21. Visuri T: Stress osteopathy of the femoral head. 10 military recruits followed for 5-11 years. Acta Orthop Scand, 68: 138-141, 1997.
22. Yamamoto T and Bullough PG: Subchondral insufficiency frac- ture of the femoral head. A differential diagnosis in acute onset of coxarthrosis in the elderly. Arthritis Rheum, 42: 2719-2723, 1999.
23. Yamamoto T, Schneider R and Bullough PG: Subchondral insufficiency fracture of the femoral head. Histopathologic correla- tion with MRI. Skeletal Radiol, 30: 247-254, 2001.