Primary Malignant Fibrous Histiocytoma of the Chest Wall Misdiagnosed as Traumatic Hemothorax
Ki-Eun Hwang, M.D.
1, June-Seong Hwang, M.D.
1, Kyung-Min Kim, M.D.
1, Jae-Wan Jung, M.D.
1, Su- Jin Oh, M.D.
1, Eun-Kyoung Kim, M.D.
1, Dae-Woon Ryu, M.D.
2, Keum-Ha Choi, M.D.
3, Eun-Taik Jeong, M.D.
1and Hak-Ryul Kim, M.D.
1Departments of
1Internal Medicine,
2Cardiothoracic Surgery, and
3Pathology, Institute of Wonkwang Medical Science, Wonkwang University School of Medicine, Iksan, Korea
Malignant fibrous histiocytoma (MFH), a type of sarcoma, is a malignant neoplasm with uncertain origins that arise from both the soft tissues and the bone. The occurrence of MFH on the chest wall is extremely rare. We hereby report a case of a 72-year-old woman who was incidentally detected with MFH after a traffic accident.
Keywords: Histiocytoma, Malignant Fibrous; Thoracic Wall; Hemothorax
Case Report
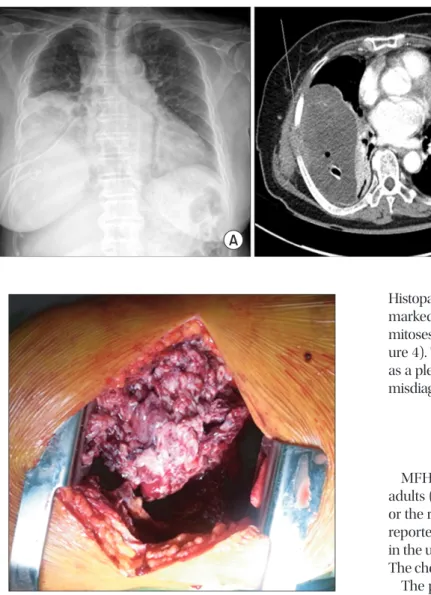
A 72-year-old woman complained of right-sided chest pain and orthopnea following a traffic accident that occurred 1 month previously. Chest radiography and computed tomog- raphy revealed large amounts of right pleural effusion and a
Copyright © 2014
The Korean Academy of Tuberculosis and Respiratory Diseases.
All rights reserved.
Introduction
Malignant fibrous histiocytoma (MFH) is the most common malignant soft tissue tumor. MFH occurs most commonly in the extremities (70−75%), followed the trunk and retroperi- toneum. It is a frequently occurring soft tissue tumor with ag- gressive biological behavior. Primary MFH of the chest wall is especially rare.
We report a case of a 72-year-old woman in whom MFH was detected incidentally after she had a traffic accident. We describe this unusual case and review the literature.
CASE REPORT
http://dx.doi.org/10.4046/trd.2014.76.6.289ISSN: 1738-3536(Print)/2005-6184(Online) • Tuberc Respir Dis 2014;76:289-291
289
Address for correspondence: Hak-Ryul Kim, M.D.
Department of Internal Medicine, Wonkwang University School of Medicine, 460 Iksan-daero, Iksan 570-974, Korea
Phone: 82-63-859-2583, Fax: 82-63-855-2025 E-mail: [email protected]
Received: Feb. 12, 2014 Revised: Mar. 4, 2014 Accepted: Mar. 12, 2014
cc