The Effect of Gait Pattern in Hemiplegia Patients through Progressive Speed Increase Treadmill Training
Lee Hyoungsoo, RPT, Ph.D
ǂDept. of Physical Therapy, Gwangju Health University
점진적인 속도증진 트레드밀 훈련이 뇌졸중 환자의 보행패턴에 미치는 영향
이형수
ǂ광주보건대학교 물리치료과
Abstract
연구목적 : 본 연구의 목적은 8주간의 점진적인 속도증진 훈련이 뇌졸중환자의 족저압, 보행주기, 보행대칭성에 어떠 한 영향을 주는지 알아보는 것이다.
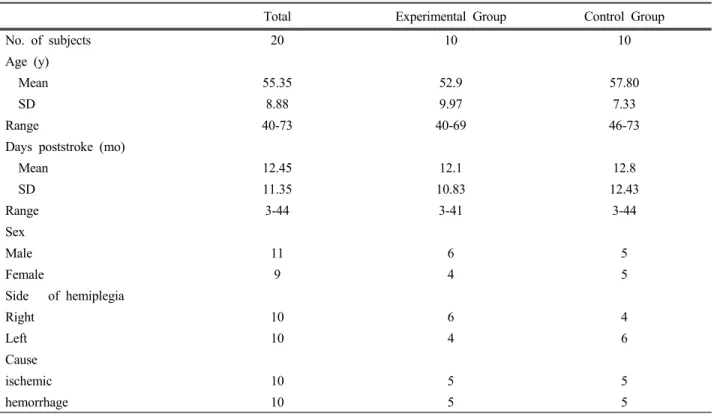
연구방법 : 연구에 참여한 대상자들은 뇌졸중으로 진단 받고 N병원에 입원한 편마비환자 20명(실험군 10명, 대조군 10명)을 대상으로 하였다. 이들은 모두 물리치료와 작업치료를 받았고, 실험군은 주3회, 8주간의 트레드밀 보행훈련를 받았고, 대조군은 받지 않았다. 실험전, 후에 F-scan을 이용하여 보행주기, 보행대칭성을 검사하였다.
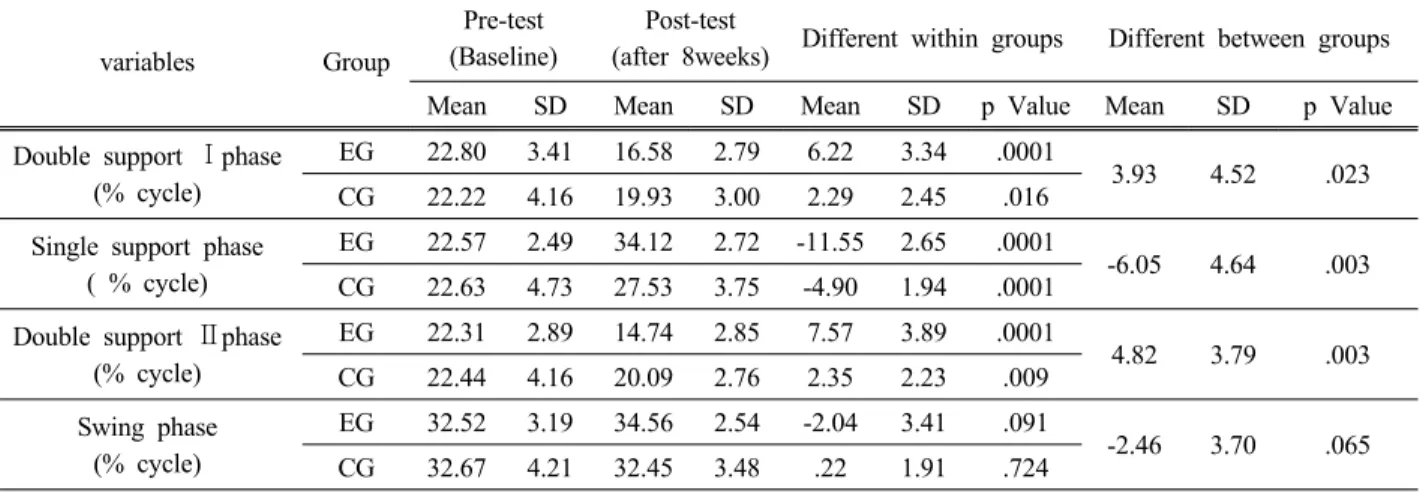
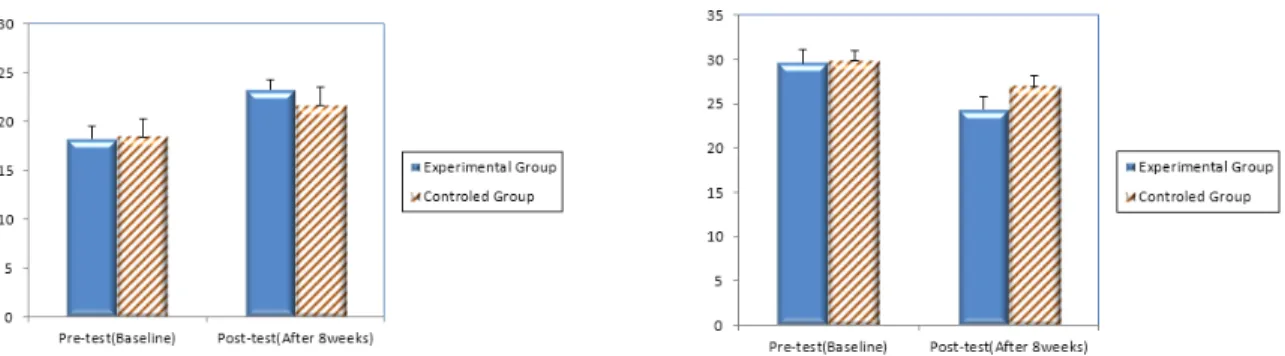
연구결과 : 8주 후, 보행주기는 실험군의 양하지지지기Ⅰ·Ⅱ, 단하지지지기에서 모두 유의하게 증가하였으나, 대조군
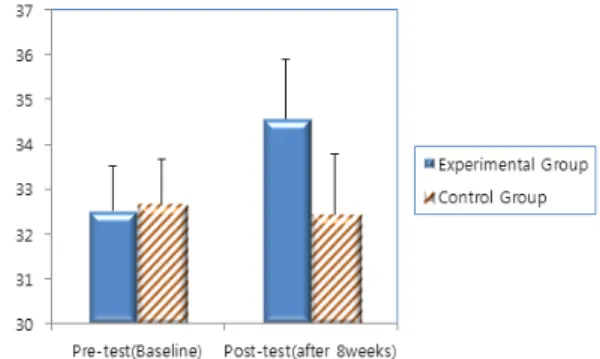
에서는 양하지지지기 Ⅱ, 단하지지지기에서 유의하게 증가하였다. 유각기는 실험군과 대조군 모두 유의하지는 않았다.보행대칭성은 입각기 대칭성에서 대조군과 비교하여 실험군에서 유의하게 증가하였으나, 유각기 대칭성은 실험군과 대 조군 모두 유의하지 않았다.
결론 : 뇌졸중 환자에 있어 보행훈련은 보행주기과 보행대칭성과 를 개선시키며, 특히 점진적인 속도 증진훈련은 양
하지지지기, 단하지지지기, 입각기 보행대칭성에 효과적인 방법으로 사용될 수 있을 것으로 보인다.Key Words : 보행대칭성, 보행주기, 보행훈련, 족저압, 편마비
ǂ