서 론
미세알부민뇨(microalbuminuria)는 미세혈관내피세포의 기능장 애 정도를 반영한 심혈관 질환의 독립적인 위험인자이다.1,2) 당뇨병 과 고혈압이 있는 환자뿐 아니라 최근에는 기저 질환이 없는 사람에 서도 미세알부민뇨가 심혈관 질환 및 신장 질환의 경과를 예측하는 중요한 인자로 알려져 있다.3-5) 따라서, 미세알부민뇨의 고위험군을
찾아내는 것은 신장 및 심혈관 질환의 발생을 줄일 수 있다는 점에 서 공중보건학으로 매우 중요하다.6)
고혈압 환자에서 알부민뇨(almubinuria)가 나타날 수 있는 기전으 로 혈관내피 기능장애, 혈관의 손상, 고혈압에 따른 사구체의 직접적 인 압력 증가로 설명될 수 있다.7-9) 60세 이전과 60세 이후에서의 고혈 압의 양상은 다르다. 60세 이전에는 수축기 혈압(systolic blood pres- sure, SBP)과 이완기 혈압(diastolic blood pressure, DBP)이 동시에 증가
Original Article
당뇨병, 만성 콩팥병이 없는 노인에서 수축기 혈압과 알부민뇨의 관계
정영효, 조아라, 정태하, 이용제*
연세대학교 의과대학 가정의학교실
Association between Systolic Blood Pressure and Albuminuria in Elderly People without Type 2 Diabetes or Chronic Kidney Disease
Young-Hyo Jung, A-Ra Cho, Tae-Ha Chung, Yong-Jae Lee*
Department of Family Medicine, Yonsei University College of Medicine, Seoul, Korea
Background: Albuminuria is associated with cardiovascular disease, and the relationship between albuminuria and hypertension is well established.
Systolic blood pressure (SBP, mmHg) has become more important than diastolic blood pressure as an independent risk predictor for cardiovascular events in the elderly. Thus, we examined the relationship between albuminuria and SBP in a general Korean population without type 2 diabetes or chronic kidney disease.
Methods: We analyzed data from the 2011–2013 Korea National Health and Nutrition Examination Survey and included 2,265 participants. SBP was divided into five groups as follows: ≥150 mmHg, 140–149 mmHg, 130–139 mmHg, 120–129 mmHg, and <120 mmHg. Albuminuria was defined as microalbuminuria and/or macroalbuminuria. Multiple logistic regression analyses were conducted to calculate the odds ratios (ORs) for albuminuria.
Results: The proportion of albuminuria decreased with decreasing SBP, from 18.2% in the group with highest SBP to 4.0% in the group with lowest SBP.
After adjusting for age, sex, body mass index, and levels of fasting plasma glucose, triglyceride, and alanine transaminase, the ORs (95% confidence intervals [CI]) for albuminuria according to each of the five groups of SBP were 1.00, 0.538 (95% CI 0.305–0.949), 0.603 (95% CI 0.368–0.991), 0.365 (95% CI 0.219–0.607), and 0.228 (95% CI 0.137–0.378), respectively.
Conclusion: Higher SBP was independently associated with an increased risk of albuminuria in the elderly without diabetes mellitus or chronic kidney disease.
Keywords: Albuminuria; Systolic Blood Pressure; Cardiovascular Disease; Korea
https://doi.org/10.21215/kjfp.2016.6.5.509 eISSN 2233-9116Korean J Fam Pract. 2016;6(5):509-513
KJFP
Korean Journal of Family PracticeReceived March 16, 2016 Revised April 21, 2016 Accepted June 24, 2016 Corresponding author Yong-Jae Lee
Tel: +82-2-2019-3480, Fax: +82-2-3463-3287 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Young-Hyo Jung, et al. Association between SBP and Albuminuria in Elderly People
Korean Journal of Family Practice
KJFP
하지만, 60세 이후에서는 DBP의 변화는 적고, 수축이 혈압이 증가하 는 고립성 수축기 고혈압(isolated systolic hypertension)이 흔하다.10) 노 인에서는 DBP보다 SBP가 높을수록 심혈관 질환, 뇌졸중, 심부전, 말 기 신장질환의 위험도가 더 증가하는 것으로 알려져 있어 SBP의 상 승이 매우 중요하다.11-14)
2014년 발표된 미국 고혈압 가이드라인 The Eighth Joint National Committee (JNC 8)에 따르면, 60세 이상의 고령에서 당뇨병 및 만성 콩팥병이 없는 고혈압 환자는 혈압의 목표치를 다소 완화하여 SBP 150 mmHg 미만, DBP 90 mmHg 미만으로 조절하기로 권고하고 있 다.15) 이러한 배경을 바탕으로 본 연구에서는 국민건강영양조사 자료 를 통해 한국인에서 당뇨병, 만성 콩팥병이 없고, 혈압약을 복용하지 않는 노인에서 SBP와 알부민뇨의 관련성에 대해 알아보고자 한다.
방 법
이 연구는 제 5기(2010–2012년) 및 제6기(2013년) 국민건강영양조 사의 자료를 활용하였다. 국민건강영양조사는 우리나라 국민의 건 강 및 식품섭취 현황 등을 종합적으로 파악하는 것을 목적으로 하 며, 연중 조사체계를 통해 3개년도마다 독립적인 순환표본으로 이루 어져 있다. 각 표본은 우리나라 전체 인구를 대표하는 확률표본이 며, 제5기 2차년도(2011년)조사와 제5기 3차년도(2012년) 조사 및 제6 기 1차년도(2013년) 조사의 총 응답자수는 각각 8,518명, 8,058명, 8,018 명이었다. 이 중 만 60세 미만, 만성 콩팥병(chronic kidney disease), 당 뇨병(diabetes mellitus)을 진단받은 수검자를 제외하였다. 또한 고혈 압 약제 복용자와 알부민-크레아티닌 비(albumin to creatinine ratio, ACR), 혈압, 체질량지수(body mass index, BMI), 공복혈당(fasting plasma glucose, FPG) 등의 결측 자료를 제외한 총 2,265명을 최종 연 구대상으로 하였다. 이 연구는 대한민국 질병관리본부의 연구 윤리 심의위원회에서 승인하였다(IRB No. 2011년: 2011-02CON-06-C, 2012 년: 2012-01EXP-01-2C, 2013년: 2013-07CON-03-4C).
1. 연구자료(data collection)
국민건강영양조사는 조사항목에 따라 건강설문조사, 검진조사, 영양조사 3가지 부문으로 구성되어 있다. 연구대상자들의 기본적인 특성을 파악하고 혈압과 알부민뇨의 관계를 알아보기 위하여 건강 설문조사 부문의 성별, 연령, 흡연력, 음주력, 운동, 과거 및 현재 앓고 있는 질환, 신체활동 자료와 검진조사 부분의 신체계측(허리둘레, BMI) 및 혈압 및 혈액 검사자료를 사용하였다.
흡연력은 현재흡연, 과거흡연, 비흡연자의 세 군으로 구분하였다.
설문 조사에서 신체활동의 강도와 횟수가 조사되었으며, 1주일에 중
등도 이상의 운동(몸이 매우 힘들거나 숨이 가쁜)을 1회 이상 한다고 응답한 군을 ‘활발한 신체활동 군’으로 정의하였다. 음주력은 대상 자들이 설문지를 작성하기 전 1달간의 음주활동과 관련된 설문조 사를 통해 조사되었다. 고위험 음주군은 남자 Alcohol Use Disorders Identification Test (AUDIT) 점수 10점 이상, 여자는 6점 이상으로 정 의하였다.
신체계측은 표준화된 장비와 측정방법을 통해 얻었으며, 키는 휴 대용 계측기(Seriter, Bismarck, ND, USA)를 사용하여 0.1 cm 단위까지 측정하였다. 체중은 0.1 kg 단위까지 측정하는 Giant-150N calibrated balance-beam 체중계(Hana, Seoul, Korea)를 사용하여 측정하였고, BMI는 체중을 키의 제곱으로 나누어 계산하였다(kg/m2). 수축기 및 DBP는 환자가 앉은 자세로, 표준화된 측정방법을 사용하여 측정하 였으며, 모든 대상자들은 5분의 간격을 두고 3회 측정하였고, 2번째 와 3번째 측정한 혈압의 평균값을 사용하였다. 혈액 검사는 최소 8시 간 이상 금식을 한 후 아침에 채혈을 하였으며, 소변 검사는 아침 첫 소변을 이용하였다. FPG 및 혈중 지질검사는 Hitachi Automatic Ana- lyzer 7600 (Hitachi, Tokyo, Japan)을 통해 분석하였으며, aspartate transaminase (AST), alanine transaminase (ALT)는 표준화된 동적 방 법(Modular P; Roche Diagnostics, Indianapolis, IN, USA)을 통해 측정 하였다. 비만은 BMI ≥25 kg/m2으로 정의하였으며, 고혈압은 SBP
≥140 mmHg 또는 DBP ≥90 mmHg 또는 고혈압 약제를 복용하고 있 을 경우로 정의하였다. 당뇨병은 FPG가 126 mg/dL 이상 또는 당뇨약 제를 복용 중인 경우로 하였다. 만성 콩팥병은 이전에 의사에 의해 진단받은 자로 정의하였다.
소변 알부민과 크레아티닌 농도는 같은 검사실에서 측정되었고, 혈액 및 소변의 크레아티닌 농도는 비색적 방법으로, 소변 알부민은 비탁계 면역 분석법을 사용하여 측정하였다(Hitachi Automatic Ana- lyzer 7600). ACR을 사용하여 알부민뇨의 양에 따라 미세알부민뇨 (microalbuminuria, ACR=30–299 mg/g creatinine [Cr])와 거대알부민뇨 (macroalbuminuria, ACR ≥300 mg/g Cr)로 구분하였으며, 알부민뇨는 미세알부민뇨와 거대알부민뇨를 모두 포함하는 것으로 정의하였다.
2. 통계 분석(statistical analysis)
혈압군을 SBP가 150 mmHg 이상, 140–149 mmHg, 130–139 mmHg, 120–129 mmHg, 120 mmHg 미만으로 총 5개 군으로 나누었고, 각각 의 군에 따른 각 임상적 특징들은 평균±표준오차 또는 퍼센트로 표 시하였다. 연속 변수에 대해서는 일원배치분산분석(one-way ANO- VA test)을 사용하였고 명목변수에 대해서는 카이제곱(chi-square test) 검정을 사용하였다. 혈압군에 따른 알부민뇨의 연관성을 알아 보고자 성별, 연령, BMI, FPG, 중성지방(triglyceride), ALT를 보정한
정영효 외. 노인에서의 수축기혈압과 알부민뇨와의 관계 Korean Journal of Family Practice
KJFP
다중 로지스틱 회귀분석(multiple logistic regression analysis)을 통해 교차비(odds ratios, ORs)와 95% 신뢰구간(95% confidence intervals, CIs)을 구하였다. 통계적 유의성은 P<0.05일 경우 유의한 것으로 보았 으며, 통계 분석은 IBM SPSS Statistics (ver. 22.0 for windows; IBM Co., Armonk, NY, USA)를 통해 수행하였다.
결 과
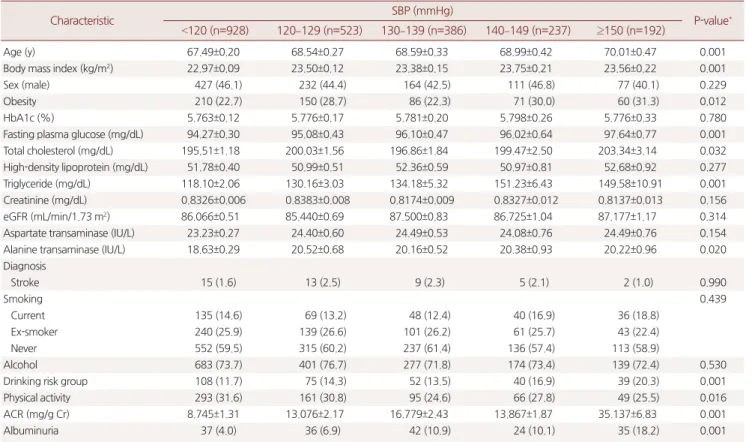
SBP에 따른 5개의 군에 따라 나눈 임상적인 특징은 Table 1과 같다.
SBP가 증가할수록 나이, BMI, FPG, 총 콜레스테롤, 중성지방, ALT 및 위험 음주율이 증가하였고, 활발한 신체활동의 빈도는 감소하였다.
SBP ≥150 mmHg 군을 기준으로 할 때, SBP가 낮아질수록 알부민뇨 의 ORs는 낮았다. 보정을 하지 않을 경우 OR 0.505 (95% CI 0.289–
0.884), OR 0.548 (95% CI 0.337–0.891), OR 0.332 (95% CI 0.201–0.546), OR 0.186 (95% CI 0.114–0.305)이었으며, 성별, 연령, FPG, 중성지방, ALT값을 보정한 다중 로지스틱 회귀분석에서는 각각 OR 0.538 (95%
CI 0.305–0.949), OR 0.603 (95% CI 0.368–0.991), OR 0.365 (95% CI 0.219–0.607), OR 0.228 (95% CI 0.137–0.378)이었다(Table 2).
고 찰
저자들은 당뇨병, 만성 콩팥병이 없는 60세 이상의 고혈압 노인 환
Table 1. Baseline characteristics according to SBP groups
Characteristic SBP (mmHg)
P-value*
<120 (n=928) 120–129 (n=523) 130–139 (n=386) 140–149 (n=237) ≥150 (n=192)
Age (y) 67.49±0.20 68.54±0.27 68.59±0.33 68.99±0.42 70.01±0.47 0.001
Body mass index (kg/m2) 22.97±0.09 23.50±0.12 23.38±0.15 23.75±0.21 23.56±0.22 0.001
Sex (male) 427 (46.1) 232 (44.4) 164 (42.5) 111 (46.8) 77 (40.1) 0.229
Obesity 210 (22.7) 150 (28.7) 86 (22.3) 71 (30.0) 60 (31.3) 0.012
HbA1c (%) 5.763±0.12 5.776±0.17 5.781±0.20 5.798±0.26 5.776±0.33 0.780
Fasting plasma glucose (mg/dL) 94.27±0.30 95.08±0.43 96.10±0.47 96.02±0.64 97.64±0.77 0.001
Total cholesterol (mg/dL) 195.51±1.18 200.03±1.56 196.86±1.84 199.47±2.50 203.34±3.14 0.032
High-density lipoprotein (mg/dL) 51.78±0.40 50.99±0.51 52.36±0.59 50.97±0.81 52.68±0.92 0.277
Triglyceride (mg/dL) 118.10±2.06 130.16±3.03 134.18±5.32 151.23±6.43 149.58±10.91 0.001
Creatinine (mg/dL) 0.8326±0.006 0.8383±0.008 0.8174±0.009 0.8327±0.012 0.8137±0.013 0.156
eGFR (mL/min/1.73 m2) 86.066±0.51 85.440±0.69 87.500±0.83 86.725±1.04 87.177±1.17 0.314
Aspartate transaminase (IU/L) 23.23±0.27 24.40±0.60 24.49±0.53 24.08±0.76 24.49±0.76 0.154
Alanine transaminase (IU/L) 18.63±0.29 20.52±0.68 20.16±0.52 20.38±0.93 20.22±0.96 0.020
Diagnosis
Stroke 15 (1.6) 13 (2.5) 9 (2.3) 5 (2.1) 2 (1.0) 0.990
Smoking 0.439
Current 135 (14.6) 69 (13.2) 48 (12.4) 40 (16.9) 36 (18.8)
Ex-smoker 240 (25.9) 139 (26.6) 101 (26.2) 61 (25.7) 43 (22.4)
Never 552 (59.5) 315 (60.2) 237 (61.4) 136 (57.4) 113 (58.9)
Alcohol 683 (73.7) 401 (76.7) 277 (71.8) 174 (73.4) 139 (72.4) 0.530
Drinking risk group 108 (11.7) 75 (14.3) 52 (13.5) 40 (16.9) 39 (20.3) 0.001
Physical activity 293 (31.6) 161 (30.8) 95 (24.6) 66 (27.8) 49 (25.5) 0.016
ACR (mg/g Cr) 8.745±1.31 13.076±2.17 16.779±2.43 13.867±1.87 35.137±6.83 0.001
Albuminuria 37 (4.0) 36 (6.9) 42 (10.9) 24 (10.1) 35 (18.2) 0.001
Values are presented as mean±standard error or number (%), unless otherwise indicated.
SBP, systolic blood pressure; eGFR, estimated glomerular filtration rate; ACR, albumin to creatinine ratio; Cr, creatinine.
*P-value was calculated by chi-square or ANOVA.
Table 2. Logistic regression results for predicting albuminuria
Systolic blood pressure (mmHg)
≥150 140–149 130–139 120–129 <120
Unadjusted 1 0.505 (0.289–0.884) 0.548 (0.337–0.891) 0.332 (0.201–0.546) 0.186 (0.114–0.305)
Model I 1 0.540 (0.307–0.952) 0.603 (0.368–0.988) 0.366 (0.221–0.607) 0.226 (0.137–0.373)
Model II 1 0.538 (0.305–0.949) 0.603 (0.368–0.991) 0.365 (0.219–0.607) 0.228 (0.137–0.378) Values are presented as odds ratio (95% confidence interval).
Model I, sex, age, body mass index adjusted; Model II, sex, age, body mass index, fasting plasma glucose, triglyceride, alanine transaminase adjusted.
Young-Hyo Jung, et al. Association between SBP and Albuminuria in Elderly People
Korean Journal of Family Practice
KJFP
자에서 SBP과 알부민뇨의 관계를 조사하였으며, SBP가 감소할수록 알부민뇨의 위험도가 감소하였다. Kim 등16)의 연구에 의하면, SBP가 130–139 mmHg 또는 DBP가 85–89 mmHg의 고혈압 전 단계(prehy- pertension)군에서도 SBP가 120–129 mmHg 또는 DBP 80–84 mmHg 의 고혈압 전 단계군보다 미세알부민뇨의 위험성이 높다고 하였다.
고혈압 약제 치료를 받고 있는 환자군에서도 130 mmHg 및 DBP 80 mmHg 이상인 군에서 알부민뇨의 위험도가 높았다.17) 본 연구에서 도 SBP 150 mmHg 미만인 군은 SBP 150 mmHg 군보다 알부민뇨의 위험도가 낮았다. 저자들은 알부민뇨에 영향을 미칠 수 있는 고혈압 약제를 복용 중인 환자를 제외함으로써 기존의 연구와 차별점을 두 었다.18)
알부민뇨는 심혈관 질환의 발생을 예측하는 독립적인 위험인자 로 알려져 있다.19-23) 고혈압 환자에서 알부민뇨가 나타날 수 있는 기 전으로는 혈관내피 기능장애,7) 동맥 경직도의 증가, 사구체 기저 막 의 변성에 의한 막의 투과성 증가 등으로 설명할 수 있다.9,20,24-26) 또한, 알부민뇨가 고혈압을 유발하거나 혈압을 악화할 수 있는 역의 관계 도 설명할 수 있다. 당뇨병과 고혈압이 없는 1,499명을 대상으로 한 전향적 연구에서 소변 ACR이 가장 높았던 4사분위군에서 고혈압 발생의 위험도가 OR은 1.93 (95% CI 1.21–3.09)으로 높았다.27) 이러한 기존의 선행 연구는 콩팥 및 혈관 내피의 잠재적 손상이 역으로 고 혈압으로 진행할 수 있다는 점을 시사한다.
미국 고혈압 가이드라인 JNC 8에서는 당뇨병과 만성 콩팥병이 없 는 60세 이상 노인에서는 SBP를 150 mmHg, DBP를 90 mmHg 이하로 덜 엄격하게 조절할 것을 권고하고 있다.15) 그러나 이와는 반대로 노 인에서도 혈압을 엄격하게 조절하는 것이 좋다는 반대의 역학 연구 도 있다. 심혈관 질환이 있는 60세 이상의 고령에서 SBP를 150 mmHg 이하로 조절한 군에 비해 140 mmHg 이하로 엄격하게 조절한 군에 서 심혈관 질환과 뇌졸중이 더 적게 발생했다는 연구가 발표된 바 있다.28) 또한 당뇨병이 없는 성인에서 SBP를 140 mmHg로 조절한 군 에 비해 120 mmHg 이하로 더 엄격하게 조절한 군에서 총 사망률, 심 혈관 질환이 적었다는 후속 연구도 엄격한 혈압 조절의 근거를 뒷받 침한다.29) 따라서 향후 노인 고혈압 환자에서 심혈관 질환을 예방하 기 위한 적절한 SBP에 대한 대규모의 전향적인 연구가 필요하다.
이 연구는 다음과 같은 제한점이 있다. 첫째, 이 연구는 단면연구 이기에 인과관계에 대한 원인-결과 관계를 설명할 수 없다. 둘째, 알 부민뇨를 측정하기 위한 소변 검사가 아침에 단 한 번 이루어졌다는 점이다. 일반적으로 금식 후 오전에 채취된 소변은 다른 시간대의 소 변보다 더 농축된다. 따라서 이러한 검사의 한계점으로 인해 알부민 뇨의 위-양성의 위험도가 높았을 수 있었을 것으로 본다.
결론적으로, 당뇨병, 만성 콩팥병이 없는 60세 이상의 고혈압 노인
환자에서 SBP가 감소할수록 알부민뇨의 위험도가 낮았다. 따라서 노인 연령에서도 SBP가 가능한 낮게 조절 되는 것이 심혈관 질환의 조기 예방적 차원에서 유익이 될 수 있음을 제시하였다.
요 약
연구배경:
알부민뇨는 심혈관 질환과 관련이 있으며, 고혈압과 알부 민뇨와의 관계는 많은 연구에서 알려져 있다. 노인에서 수축기 혈압 은 심혈관 질환의 예측 인자로 이완기 혈압보다 중요하다. 그래서 본 연구에서는 당뇨 및 만성 콩팥병이 없는 고령의 한국인에게 있어 수 축기 혈압과 알부민뇨와의 관계를 분석하고자 한다.방법:
2011–2013년의 한국 국민건강영양조사 자료를 이용하였으며, 해당 년도에서 2,265명의 대상자를 선정하여 연구를 진행하였다. 대 상자를 수축기 혈압에 따라 150 mmHg 이상, 140–149 mmHg, 130–139 mmHg, 120–129 mmHg 120 mmHg 미만의 다섯 그룹으로 나누 어 알부민뇨와의 관계를 확인하였다. 알부민뇨는 미세알부민뇨와 거대알부민뇨를 모두 포함하는 것으로 정의하였다. 혈압군에 따른 알부민뇨의 연관성을 알아보고자 성별, 연령, 체질량지수, 공복혈당, 중성지방(triglyceride), alanine transaminase (ALT)를 보정한 다중 로 지스틱 회귀분석(multiple logistic regression analysis)을 통해 교차비 (odds ratios, ORs)를 구하였다.
결과:
알부민뇨의 비율은 수축기 혈압이 가장 높은 그룹에서 18.2%, 가장 낮은 그룹에서 4.0%로 수축기 혈압이 감소할수록 감소하였다.나이, 성, 체질량지수, 공복혈당, 중성지방, ALT 값을 보정한 후에 각 수축기 혈압 그룹에 따른 알부민뇨의 ORs 값은 1.00, 0.538 (95% con- fidence intervals [CI] 0.305–0.949), 0.603 (95% CI 0.368–0.991), 0.365 (95% CI 0.219–0.607), 0.228 (95% CI 0.137–0.378)이었다.
결론:
60세 이상의 당뇨 및 만성 콩팥질환이 없는 노인에게 있어 수 축기 혈압이 높을수록 알부민뇨의 위험성이 높았다.중심단어:
알부민뇨; 수축기 혈압; 심혈관 질환; 대한민국REFERENCES
1. Hillege HL, Janssen WM, Bak AA, Diercks GF, Grobbee DE, Crijns HJ, et al.
Microalbuminuria is common, also in a nondiabetic, nonhypertensive pop- ulation, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity. J Intern Med 2001; 249: 519-26.
2. Hillege HL, Fidler V, Diercks GF, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, et al. Urinary albumin excretion predicts cardiovascular and noncardio- vascular mortality in general population. Circulation 2002; 106: 1777-82.
3. de Zeeuw D, Remuzzi G, Parving HH, Keane WF, Zhang Z, Shahinfar S, et
정영효 외. 노인에서의 수축기혈압과 알부민뇨와의 관계 Korean Journal of Family Practice
KJFP
al. Albuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation 2004; 110: 921-7.
4. Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF, Hoogwerf B, et al. Al- buminuria and risk of cardiovascular events, death, and heart failure in dia- betic and nondiabetic individuals. JAMA 2001; 286: 421-6.
5. Yudkin JS, Forrest RD, Jackson CA. Microalbuminuria as predictor of vas- cular disease in non-diabetic subjects. Islington Diabetes Survey. Lancet 1988; 2: 530-3.
6. Schrier RW, Estacio RO. The effect of angiotensin-converting enzyme in- hibitors on the progression of nondiabetic renal disease: a pooled analysis of individual-patient data from 11 randomized, controlled trials. Ann Intern Med 2001; 135: 138-9.
7. Deckert T, Feldt-Rasmussen B, Borch-Johnsen K, Jensen T, Kofoed-En- evoldsen A. Albuminuria reflects widespread vascular damage. The Steno hypothesis. Diabetologia 1989; 32: 219-26.
8. Williams SA, Boolell M, MacGregor GA, Smaje LH, Wasserman SM, Tooke JE. Capillary hypertension and abnormal pressure dynamics in patients with essential hypertension. Clin Sci (Lond) 1990; 79: 5-8.
9. Deen WM. What determines glomerular capillary permeability? J Clin In- vest 2004; 114: 1412-4.
10. Franklin SS, Jacobs MJ, Wong ND, L’Italien GJ, Lapuerta P. Predominance of isolated systolic hypertension among middle-aged and elderly US hyper- tensives: analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension 2001; 37: 869-74.
11. Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, et al.
Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reduc- tions in blood pressure: overview of randomised drug trials in their epide- miological context. Lancet 1990; 335: 827-38.
12. Hsu CY, McCulloch CE, Darbinian J, Go AS, Iribarren C. Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kid- ney disease. Arch Intern Med 2005; 165: 923-8.
13. Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression from hypertension to congestive heart failure. JAMA 1996; 275: 1557-62.
14. Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhäger WH, et al.
Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hyperten- sion in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350: 757-64.
15. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311: 507-20.
16. Kim BJ, Lee HJ, Sung KC, Kim BS, Kang JH, Lee MH, et al. Comparison of
microalbuminuria in 2 blood pressure categories of prehypertensive sub- jects. Circ J 2007; 71: 1283-7.
17. Kim YS, Kim HS, Oh HY, Lee MK, Kim CH, Kim YS, et al. Prevalence of mi- croalbuminuria and associated risk factors among adult Korean hyperten- sive patients in a primary care setting. Hypertens Res 2013; 36: 807-23.
18. Vejakama P, Thakkinstian A, Lertrattananon D, Ingsathit A, Ngarmukos C, Attia J. Reno-protective effects of renin-angiotensin system blockade in type 2 diabetic patients: a systematic review and network meta-analysis. Diabe- tologia 2012; 55: 566-78.
19. Jensen JS, Feldt-Rasmussen B, Strandgaard S, Schroll M, Borch-Johnsen K.
Arterial hypertension, microalbuminuria, and risk of ischemic heart disease.
Hypertension 2000; 35: 898-903.
20. Stehouwer CD, Smulders YM. Microalbuminuria and risk for cardiovascu- lar disease: Analysis of potential mechanisms. J Am Soc Nephrol 2006; 17:
2106-11.
21. Cerasola G, Cottone S, Mulè G. The progressive pathway of microalbumin- uria: from early marker of renal damage to strong cardiovascular risk pre- dictor. J Hypertens 2010; 28: 2357-69.
22. Chico A, Tomás A, Novials A. Silent myocardial ischemia is associated with autonomic neuropathy and other cardiovascular risk factors in type 1 and type 2 diabetic subjects, especially in those with microalbuminuria. Endo- crine 2005; 27: 213-7.
23. Yuyun MF, Adler AI, Wareham NJ. What is the evidence that microalbumin- uria is a predictor of cardiovascular disease events? Curr Opin Nephrol Hy- pertens 2005; 14: 271-6.
24. Weir MR. Microalbuminuria and cardiovascular disease. Clin J Am Soc Nephrol 2007; 2: 581-90.
25. O’Rourke MF, Safar ME. Relationship between aortic stiffening and micro- vascular disease in brain and kidney: cause and logic of therapy. Hyperten- sion 2005; 46: 200-4.
26. Smulyan H, Safar ME. Systolic blood pressure revisited. J Am Coll Cardiol 1997; 29: 1407-13.
27. Wang TJ, Evans JC, Meigs JB, Rifai N, Fox CS, D’Agostino RB, et al. Low- grade albuminuria and the risks of hypertension and blood pressure pro- gression. Circulation 2005; 111: 1370-6.
28. Bangalore S, Gong Y, Cooper-DeHoff RM, Pepine CJ, Messerli FH. 2014 Eighth Joint National Committee panel recommendation for blood pres- sure targets revisited: results from the INVEST study. J Am Coll Cardiol 2014; 64: 784-93.
29. SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, et al. A randomized trial of intensive versus standard blood- pressure control. N Engl J Med 2015; 373: 2103-16.