후내측 도달법을 이용한 관절경적 슬와낭종 감압술 및 절삭술 - 수술 수기 -
성균관대학교 의과대학 삼성서울병원 정형외과학교실, 천안충무병원 정형외과*, 울산대학교 의과대학 정형외과학교실†
안진환・조용진*・고상훈
†・박준식・김효곤
= 국문 초록=
서 론: 후내측 도달법을 이용한 관절경적 슬와낭종의 감압술 및 절삭술의 수술수기를 보고하고자 하였다.
수술 수기: 슬관절의 관절경적 기본검사 후, 관절내 동반 병리소견이 있을시 이를 관절경적 술식을 이용해 치료하고, 관절경을 전외측 도달법으로 혹은 후내측 도달법으로 위치시켜 후내측부를 관찰하여 후관절낭의 연결구멍을 찾는 것이 가장 중요하며, 경우에 따라서는 낭주름에의해 덮여있어 확인이 어려울수 있으므로 주 의를 요한다. 후관절낭의 연결 구멍을 확인하고 전동절삭기를 후내측 도달법으로 위치시켜 후관절낭의 구멍 을 8 mm 이상 확장한다음 슬와낭종의 감압술을 시행하고, 다시 관절경을 후내측 도달법으로 위치하여 후관 절낭의 확장된 구멍을 통하여 슬와낭종 내부를 관찰하면서 슬와낭종을 덮고 있는 내측피부에서 18 gauge 척추용 바늘을 outside-in 방법으로 찔러 낭종내로 위치한 것을 확인한후 1 1번 blade 로 피부를 조금 절개 하여 낭종을 통한 도달법을 개설한후 전동절삭기를 삽입한다. 관절경으로 낭종의 벽을 관찰하면서 전동절삭 기를 이용하여 낭종의 내부에서 낭종의 벽을 절삭 한다.
결 론: 슬와낭종의 관절경적 치료는 고식적인 관혈적 절개술의 대치방법으로 슬와낭종과 동반된 병변을 관 절경적으로 진단 및 치료할수 있고 후내측 도달법을 이용하므로서 관절경적으로 슬와낭종의 감압술 및 절삭 술을 효과적으로 시행할 수 있으리라 사료된다.
색인 단어: 슬와낭종, 관절경적 낭종 감압술 및 절삭술, 후내측 도달법
Volume 16, Number 2, December 2004
서 론
슬와부 낭종은 A d a m s1 ) 와 B a k e r3 ) 에 의해 기술 된후 그 치료에 다양한 방법들이 제시되었고5 , 6 , 9 , 1 1 , 1 5 , 2 0 -
2 4 ), 단순한 외과적 절제술후에는 재발의 빈도가 높아
1 0 , 2 1 , 2 7 )
, 동반된 슬관절내 병변에 주목하게 되었으며, 최근의 연구2 4 )에 따르면 이러한 동반된 슬관절내 병 변을 잘 치료하는 것과 슬관절내로 연결된 구멍을 찾 아 확공시켜 한방향으로의 관절액의 흐름을 차단시켜
주는 것이 재발을 줄이는데 중요하다고 하였다. 관절 경 수술은 최소 침습적 술식으로서 슬와낭종과 연관 된 슬관절내 병변을 진단 및 치료하고 슬와낭종과 연 결된 슬관절내의 구멍을 찾아 확공하는데 적합하여, 고식적인 관혈적 절제술을 피할수 있고 술후 향상된 결과를 기대할 수 있어 최근 선호되어 왔다2 4 ). 이에 본교실에서는 후내측 도달법을 이용한 관절경적 슬와 낭종의 감압술 및 절삭술의 수술수기를 보고하고자 하였다.
Corresponding Author: Yong Jin Cho, M.D.
Department of Orthopaedic surgery, Cheonan ChungMu Hospital.
542-3 Ssangyong-dong, Cheonan, 330-090, Chungnam, Korea
Tel : 041-570-7581, Fax : 041-574-3328, E-mail : [email protected]
수술 수기 1. 진단적 관절경 검사
표준 전외측 및 전내측 도달법을 통하여 기본적인 관절경적 관찰을 시행하여 슬관절내 이상 소견을 모 두 확인한다. 후내측 구획의 병변은 전방도달법으로 만 보기에는 한계가 있어 진단적 오류를 범하기 쉬운 부위로 이 부위의 병변이 의심될때는 반드시 후내측 도달법을 이용하여 관찰하여야 한다. 저자는 후내측 도달법의 개설에 대해 자세히 보고한 바2 )가 있으므로 참고하기 바라며(Fig. 1), 이 후내측 도달법을 통해 후내측 구획의 병변 유무을 확인하고, 후내측 관절낭 의 슬와낭종과의 연결구멍을 찾는다.
2. 슬관절내 동반 병변 치료
슬관절의 관절경적 기본검사 후, 관절내 동반 병리 소견이 있을시 이를 관절경적 술식을 통해 치료한다.
반월상 연골판 손상에 대해서는 가능하면 봉합술을 시행하고 그렇지 않을경우 가능한 많은 부위를 남길 수 있게 손상된 반월상 연골판 부분 절제술을 시행한 다. 관절연골의 병변에 대해서는 병변의 정도( O u t- erbridge grade)에 따라 관절연골 성형술(grade II and grade III) 혹은 미세골절술(grade IV)을 시
행한다.
류마토이드 관절염 환자는 활액막제거술, 관절내 유리체에 대해서는 관절경적 제거술, 추벽 증후군 환 자는 추벽 절제술등 진단적 관절경 검사시 관찰된 슬 관절내 동반병변에 대해 관절경적 치료를 시행한다.
3. 슬관절과 슬와낭종과의 연결 구멍 확인
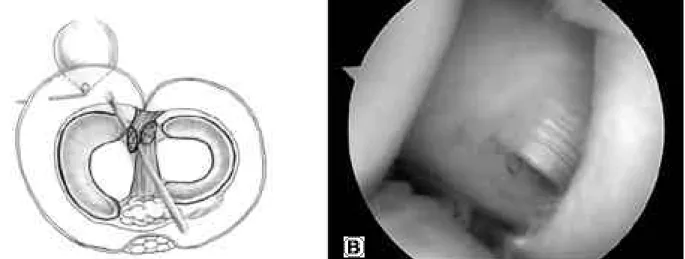
먼저 관절경을 전외측 도달법으로 삽입하여 후내측 부를 관찰하여 후관절낭의 연결 구멍을 찾는 것이 가 장 중요 하다. 전외측 도달법으로 위치한 관절경을 과간 절흔을 지나 후내측 구획에 도달시키기 위해서 는, 전내측 도달법으로 끝이 둥근 투관침을 관절내로 삽입하여 후방 십자 인대와 대퇴내과 사이로 위치시 켜 전진 및 후퇴를 수 회 반복하여 둘 사이의 공간을 확보한다. 관절경으로 관찰하면서 관절경을 약간 전 진시켜 확보된 공간에 관절경 외피를 고정하고 관절 경만을 제거한 후 외피에 끝이 둥근 투관침을 삽입하 고 슬관절을 6 0도 굴곡한 상태에서 후방 십자 인대 와 대퇴내과의 과간 절흔 벽 사이를 지나 후방 구획 에 도달하도록 전진시킨다. 초반에 저항감을 느끼며 어느 정도 전진을 한 후 저항이 사라지면 후내측 구 획에 도달한 것이다. 이때 끝이 둥근 투관침의 끝을 후방 십자 인대쪽으로 향하도록 하여 전진시켜야 대 퇴내과의 과간 절흔 부위쪽 관절 연골부 손상을 피할 수 있다. 저항이 사라지면 끝이 둥근 투관침을 제거 하고 관절경을 다시 관절경 외피 내로 삽입한 후 조 금씩 관절경을 전진 혹은 후진 시키며 주변 구조물을 확인한다. 관절경 시야에 둥근 모양의 대퇴내과 후방 부를 찾아 방향 감각을 되찾은 후 내측 반월상 연골 판 후각부 및 후내측 관절막을 관찰한다. 저자는 낭 주름이 덮여있어 관절낭의 연결구멍을 찾기어려운 경 우에도 후내측 도달법으로 소식자를 삽입하여 철저한 p r o b i n g으로 후내측 관절낭의 연결구멍을 찾을수 있 었으며, 낭주름을 소식자를 이용하여 아래쪽으로 당 겨보면 그 후외측에는 비복근의 내측 두가 위치하고 비복근의 후내측으로 슬와낭종과의 연결구멍이 있는 것을 관찰하게 된다(Fig. 2). 전외측 도달법으로 후 관절낭의 연결구멍이 잘 관찰되지 않는 경우 후내측 도달법으로 관절경을 위치시켜 연결구멍을 찾고 필요 에 따라서는 7 0도 관절경을 이용한다.
4. 슬와낭종 감압술
관절경을 전외측 도달법으로 삽입하여 후내측 관절 낭의 연결구멍을 확인한 후 먼저 basket forcep을 Fig. 1. The posteromedial portal is made by transillumination
technique. The arthroscope is positioned at anterolateral portal and then advanced between the lateral aspect of medial femoral condyle and posterior cruciate ligament and reached at posteromedial compartment. While viewing the posteromedial compartment, the posterome- dial portal is made by outside- in technique.
후내측 도달법으로 삽입하여 낭주름의 일부를 절제하 고 다시 전동 절삭기를 후내측 도달법으로 위치시켜 후관절낭의 연결구멍을 8 mm 정도로 확장하여 슬 와낭종의 감압술을 시행한다(Fig. 3). 이때 특히 비 복근 내측 두의 내측에 있는 관절낭을 충분히 절제하 여야 효과적인 감압술이 될 수 있다. 연결구멍이 충 분히 확공되면 노란색의 슬와낭종액(cystic fluid)이 흘러나오는 것을 관찰할 수 있다.
5. 슬와낭종 절삭술
관절경을 후내측 도달법으로 위치시켜 대퇴내과 후 방부를 찾아 방향 감각을 되찾은 후 후관절낭의 확장 된 구멍을 통하여 전진시킨다. 이때 비복근의 내측 두의 후 내방으로 관절경을 전진 시키면 슬와낭종 내 부에 도달할 수 있으며, 슬와낭종 내부를 관찰하면서 슬와낭종을 덮고있는 내측 피부에서 광선투영을 이용 하여 신경, 혈관의 손상을 피하도록 18 gauge 척추 용 바늘을 outside-in 방법으로 찔러 낭종 내로 위 치한 것을 확인한후 1 1번 blade 로 피부를 조금 절 개하여 낭종을 통한 도달법을 개설한 후 이를 통해 전동절삭기를 삽입한다(Fig. 4). 관절경으로 낭종의 벽을 관찰하면서 전동절삭기를 이용하여 낭종의 내부 에서 낭종의 벽을 절삭한다. 이때 절삭기의 칼날은 낭종벽 안쪽을 향하게 하여 신경 및 혈관 조직이 위 치한 낭종의 외측벽 쪽으로는 가능하면 전동절삭기의 칼날이 닿지 않도록 주의하면서 낭종의 벽만을 제거
하도록 하여야 하며, 낭종의 내부를 잘 관찰하여 이 상 증식된 활액막이나 비정상적인 섬유성 조직이 증 식되어 있으면 이를 같이 제거한다. 또한 슬와낭종의 연결구멍의 입구는 불규칙적인 섬유성 조직들이 증식 되어있는 경우가 많고 이를 제거하면 슬와낭종 내부 에 이르게 되며, 노란색의 낭종액이 흘러나오는 것을 관찰할 수 있다(Fig. 5).
Fig. 2. (A) It is the most important procedure to find the opening of connection between joint cavity and popliteal cyst at posterome- dial compartment using anterolateral or posteromedial portal. In some cases the capsular fold overlie the opening of connec- tion, so thorough probing with probe which is positioned at the posteromedial portal is mandatory. (B) Arthroscopic view shows the opening of connection. The probe is inserted from posteromedial portal and then meticulous probing is performed to find the openig at the posteromedial capsule. After the capsular fold which overlie the opening being displaced inferiorly by the probe, the opening is shown at the posteromedial side of the medial head of gastrocnemius.
Fig. 3. When the opening of connection which is located just posteromedial side of medial head of gastrocnemius is visualized, it is enlarged about 8 mm by the arthroscop- ic decompressive procedure of popliteal cyst using bas- ket forcep at first and then arthroscopic shaver which is approached via the posteromedial portal.
고 찰
슬와낭종은 1 8 4 0년 A d a m s1 )에 의해 처음 기술되 고 1 8 7 7년 B a k e r3 )에 의해 B a k e r’s cyst 로 명명된
후 그 원인과 치료에 있어 많은 논란이 있어왔다
5 , 6 , 9 , 1 1 , 1 2 , 1 5 , 1 6 , 2 0 - 2 4 )
. 그러나 단순한 관혈적 절제술 후에는 재발이 많아1 0 , 2 1 , 2 7 )
동반된 관절내 병변을 치료하는 것 이 중요하다고 인식되어왔다. 슬와낭종과 이와 연관
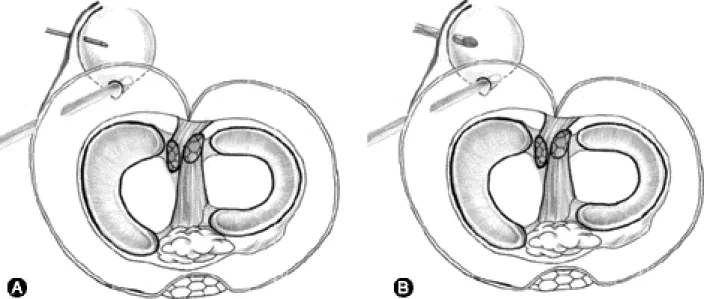
Fig. 4. The arthroscope is positioned at the posteromedial portal and advanced into popliteal cyst via enlarged opening to visualize the inside of popliteal cyst. (A) While visualizing the inside of popliteal cyst, a 18 gauge spinal needle is introduced by out- side-in technique from medial side of the skin overlying popliteal cyst. And then we make trans-cystic portal at the site of spinal needle by incising the skin with # 11 blade and (B) arthroscopic shaver is introduced within popliteal cyst via trans-cys- tic portal, and arthroscopic cystectomy is performed to shave the inner wall of popliteal cyst with arthroscopic shaver.
Fig. 5. (A) Viewing from the posteromedial portal shows the opening of connection which is positioned just postero- medial side of the medial head of gastrocnemius. And then the arthroscope is advanced behind the medial head of gastrocnemius into the popliteal cyst. (B) Occasional- ly, there are irregular arranged fibrotic tissues at the entrance to popliteal cyst. While removing the fibrotic tissues by the shaver via trans-cystic portal, the yellow- ish cystic fluid gush out. (C) After removal of fibrotic tissues, we can see the inner wall of popliteal cyst and perform cystectomy.
된 슬관절내 병변의 진단에는 초음파, 관절조영술, 컴퓨터 단층촬영, 자기공명영상 등이 있으며8 , 1 8 , 2 0 )
, 특히 자기공명영상은 비침습적인 진단법으로 높은 해 상도로 동반된 관절내 병변을 확인할 수 있고 특이성 이 높아 최근 선호되고 있다1 9 , 2 5 , 2 6 ). 후관절낭의 연결 구멍의 빈도는 보고자마다 다르며4 , 5 , 9 , 1 3 , 2 2 )
, Lindgren 과 W i l l e n1 7 )은 정상 성인의 5 0 %에서 존재한다고 하 였다. 또한 J a y s o n과 D i x o n1 2 )및 L i n d g r e n1 6 )에 따 르면 슬관절내에서 슬와낭종으로 관절액이 지속적으 로 유출되는 밸브기전이 있어 이를 간과하는 경우 재 발의 원인이 될수 있다고 하였다. Baker3 )에의해 동 반된 관절내 병변이 기술된 이후 많은 저자들이 슬관 절내 동반 병변을 보고하고 있으며, 그 빈도는 4 1 % 에서 8 5 %로 다양하다4 , 7 , 2 3 , 2 7 ). 슬와낭종과 연관된 슬 관절내 병변으로는 내측 반월상연골판 손상, 특히 후 각부의 손상이 가장 많은 것으로 보고되어 왔으나
6 , 1 2 , 2 4 )
, Rupp2 3 )등은 슬관절경 수술을 시행하였던 1 0 0 명의 환자와 대조군 1 0 0명을 대상으로 최근의 전향 적인 연구에서 슬와낭종의 유병율은 2 0 %였고, 슬와 낭종을 가졌던 8 5 %의 환자가 관절연골의 병변이, 7 0 %의 환자가 내측 반월상 연골판의 손상이 관찰되 어 슬와낭종이 없는 환자군에 비해 유의한 차이를 보 였다. 특히 저자들은 관절연골 병변에 주목하여 슬와 낭종 환자군에서 grade III 와 grade IV의 연골병 변이 7 0 %를 차지하고 있어 슬와낭종이 없었던 환자 군의 6 %보다 진행된 연골병변을 가지고 있었으며,
이런 환자들에 있어서 전례에서 술후 슬와낭종이 잔 존하여 그 결과가 나빴다고 보고하면서 진행된 연골 병변이 있을 때 관절경적 수술의 한계가 있음을 지적 하였다. 그러나 이들은 주로 전방도달법을 사용하였 으며, 후관절낭의 연결구멍이나 밸브기전의 차단에 대한 기술은 없어 이러한 결과가 도출되었을 수도 있 으리라 사료되었다. 저자는 본 술식을 이용하여 1 2 개월이상 추시 관찰이 가능하였던 1 1예의 관절경적 슬와낭종 감압술 및 절삭술을 시행하였으며, 추시관 찰 기간중 슬와낭종의 재발은 관찰되지 않았으나 (Fig. 6), 슬관절내 동반된 병변에 따른, 특히 관절 연골 병변이 있었던 예에 주목하여 그 임상적 결과를 보고할 예정이다.
그동안 제시되었던 슬관절과 슬와낭종의 연결구멍 을 차단하는 치료법을 살펴보면 H u g h s t o n1 1 )등은 단 순 관절낭 봉합술을, Childress6 )는 비복근과 반막양 근의 건을 이용하여결손부위를 보강하였으며, R a u s c h n i n g2 0 )은 비복근 내측두의 건을 경상이식하 였으나 이러한 방법으로는 비복근과 반막양근은 서로 겹쳐져있어 후관절낭의 연결구멍을 찾는 것이 어려워 정확한 관절낭 봉합이 쉽지않고 시간이 지날수록 슬 관절 굴신 운동때 관절내압을 견디지 못하여 파열이 일어날수 있다. 최근에는 최소 침습적인 치료법으로 관절경을 이용한 술식으로 관절경으로 슬관절내 병변 을 진단 및 치료하고 슬와낭종은 관혈적 절제술을 시 행하였던 초기 술식으로 부터 슬와낭종의 발생기전에
Fig. 6. (A) A preoperative image of MRI of a patient with popliteal cyst shows huge popliteal cyst at posteromedial compartment of the knee. (B) An image of MRI of the same patient at postoperative 12 months shows disappearance of popliteal cyst .
대한 이해가 더해감에 따라 외과적 슬와낭종 절제술 없이 슬관절내 동반병변을 관절경적으로 진단 및 치 료하고 관절경적 슬와낭종 감압술 및 절삭술을 시행 하는 술식으로 발전되어왔다1 5 ). Sansone 과 D e Ponti 2 4 )는 관절경적 술식으로 동반된 관절내 병변 의 적절한 치료 및 한 방향으로의 관절액 흐름을 차 단하는 것이 중요하다고 하였으며, 90%의 환자에서 내측반월상 연골판 후각부 손상이 있어 선택적 반월 상연골판 절제술을 시행하여 반월상 연골판 체부 (meniscal body)와 후각부사이에 슬와낭종과의 연 결구멍을 찾아 확공하여 좋은 결과를 보였으나, 진행 된 관절연골 병변이 있었던 6예의 환자중 1예는 추 시시 슬와낭종이 지속되었고 일상생활에서도 통증을 호소하였다고 보고하였다. 따라서 동반된 진행된 관 절연골병변이 있는경우 그 결과가 다소 좋지않음을 예견할 수 있으나, 이를 R u p p2 3 )등이 보고하였던 grade III 와 grade IV의 관절연골 병변이 있었던 환자의 전예에서의 술후 슬와낭종의 잔존과 비교해보 면 관절내 연결구멍을 찾고 이를 확공시켜 한방향으 로의 관절액의 흐름을 차단하는 것이 슬와낭종의 잔 존을 막을수 있는 중요한 방법이 될 수 있다는것으로 사료되었다. 또한 이들은 후관절낭의 구멍을 확장시 켜도 관절구조물의 약화는 없었다고 하였으나 S a n- sone 과 De ponti2 4 )의 술식은 내측 반월상 연골판 후각부 손상이 있을 때 전방도달법으로 내측 후각부 를 모두 절제하여 연결구멍을 찾았고, 이는 생역학적 으로 바람직하지 않을 것으로 사료되며, Johnson1 3 ) 등은 후관절낭의 관절 막주름 뒤의 연결구멍을 기술 하였던 바 저자의 경험으로도 내측 반월상 연골판 후 각부를 완전히 절제하지 않고도 후관절낭의 연결구멍 을 전외측 및 후내측 도달법으로 확인할 수 있어 가 능한 생역학적으로 중요한 내측 반월상 연골판 후각 부를 남겨놓는 것이 바람직할 것으로 사료된다.
K a n e k a s u1 4 )등은 류마토이드 관절염 환자에서 활막 절제술 및 관절경적 낭종절제술을 시행하여 우수한 결과를 보고하였다. 슬와 낭종의 관절경적 술식의 장 점은 관절내 동반 병변을 동시에 해결할 수 있으며, 슬와 낭종 자체의 감압술 및 절삭술이 가능하여 재발 을 줄일 수 있는 술식으로 피부 절개가 적음으로 조 기 보행과 관절 운동이 가능하여 술후 회복이 빠른 술식이라 할 수 있겠다. 저자들도 후내측 도달법을 이용하여 후관절낭의 확공된 연결구멍을 통해 슬와낭 종 내부를 관찰할수 있었으며, 슬와낭종 내부의 비정 상적인 활액막 비후나 섬유성 증식 및 막성 낭을 안 전하게 제거할 수 있었다. 따라서 저자들은 슬와낭종 과 관련된 모든 병리소견을 안전하고 효과적으로 진
단 및 치료할 수 있는 술식으로 본 수술 수기를 보고 하는 바이다.
결 론
저자들의 후내측 도달법을 이용한 관절경적 슬와낭 종 감압술 및 절삭술은 최소 침습적 술식으로서 관절 경적으로 동반된 슬관절내 병변을 진단 및 치료하고 특히 후관절낭의 연결구멍을 찾고 확공하여 한방향으 로의 관절액의 흐름을 차단 할수 있으며, 또한 슬와 낭종의 내벽의 병리소견도 효과적이고 안전하게 제거 하여 재발을 줄일 수 있는 술식으로 본 수술수기를 보고하는 바이다.
REFERENCES
01) Adams R : Chronic rheumatoid arthritis of the knee joint. J Med Science. 17:520-522, 1840(Cited form Vahvancen V: Popliteal cyst. A follow-up study on 42 operatively treated patients. Acta Orthop Scand, 44:303-310, 1973)
02) Ahn JH and Ha CW: Posterior Trans-Septal Portal for Arthroscopic Surgery of the knee Joint.
Arthroscopy: The J. of Arthroscopic and Related Surgery, 16(7):774-779, 2000.
03) Baker WM: On the formation of synovial cysts in the leg in connection with disease of the knee joint .St Barotholomew’s Host, 13:254-264, 1877(Cited form Vahvaned V: Popliteal cyst. A follow-up study on 42 operatively treated patients. Acta Orthop Scand, 444:303-310, 1973)
04) Burleson RJ, Bickel WH and Dahlin DC : Popliteal cyst. A clinicopathological surgery. J Bone Joint Surg 38A:1265-1274, 1956.
05) Chae IJ, Han SB, Lee KH and Kim TH: Analysis of Associated Intra-articular Lesions in Popliteal Cyst under Arthroscopic in Adults. J Korean Knee Society, 12-1:112-118, 2000.
06) Childress HM. : Popliteal cysts associated with undiagnosed posterior lesion of the medial meniscus.
The significance of age in diagnosis and treatment. J Bone Surg Am 54:1487-1492, 1970.
07) Gristina AG, Wilson PD: Popliteal cysts in adults and children. A review of 90 cases. Arch Surg 8 8 : 357-363, 1964.
08) Hall FM: Baker cysts. 203(2):577-578, 1997
09) Han CD, Shin SI and Park BM: A Clinical study of the popliteal cyst-an analysis of 90 cases.: J of Korean Orthop Assoc. 253:433-438, 1986.
10) Harvery JP and Corcos J: Large cysts in lower leg originating in the knee occurring in patients with rheumatioid arthritis. Arthr Rheum 3:218-228, 1960.
11) Hughston JC, Baker CL and Mello W: Popliteal cyst: A surgical approach. Orthopaedics. 14(2):147- 150, 1991.
12) Jayson MIV and Dixon A St J.: Valvular mecha- nism in juxtaarticular cysts. Ann Rhem Dis 29:415- 420, 1970.
13) Johnson LL, van Dyk GE, Johnson CA, et al: The popliteal bursa(Baker’s cyst): An arthroscopic per- specitive and the epidemiology. Arthroscopy 13:66- 72,1997.
14) Kanekasu K, Nagashima K, Yamauchi D and Yamakado K: A clinical study of arthrocopic cys- tectomy on politeal cysts associated with rheumatoid arthritis. Ryumachi.:37(6):761-769, 1997.
15) Ko SH and Ahn JH: Popliteal cystoscopic excision- al debridement and removal of capsular fold of valvular mechanism of large recurrent popliteal Cyst. Arthroscopy, 20(1):37-44, 2004.
16) Lindgren PG : Gastrocnemio-semimembranosus bursa and its relation of the knee joint. III Pressure measurements in joint and bursa. Acta Radiol Diagn 19:377-388, 1978.
17) Lindgren PG and Willen R: Gsatrocnemio-semi- membranosus bursa and its relation to the knee joint.
I. Anatomy and histology. Acta Radiol Diagnosis, 18:497-511,1977.
18) Maffulli N, Regine R, Carrillo F, Minelli S and Beaconsfield T: Ultrasonographic scan in knee pain in athletes. Br J Sports Med, 26:93-96, 1992.
19) Miller TT, Staron RB, Koenigsberg T. et al: MR imaging of Baker cysts: Association with internal derangement, effusion and degenerative arthropathy.
Radiology 201:247-250, 1996.
20) Rauschning W : Popliteal cyst (Baker ’s cyst)in adults. II: Capsuloplasty with and without a pedicle graft. Acta Orthop Scand, 51:547-557, 1980.
21) Rauschning W and Lindgren PG: Popliteal cysts (Baker’s cysts) in adults. I: Clinical and roentgeno- logical results of operative excision. Acta Orhtop Scand 50:583-591, 1979.
22) Roh KJ, Kim DW and Yoo JD.: Significance of Arthroscopy in Patients with Popliteal Cysts of Knees: J of Korean Orthop. A s s o c. 32-2:309-312, 1997.
23) Rupp S, Seil R, Jochum P and Kohn D: Popliteal Cysts in Adults Prevalence, Associated intraarticular lesions and results after arthroscopic treatment. The American Journal of Sports Med. 30-1:112-115, 2002.
24) Sansone V and De Ponti A: Arthroscopic Treat- ment of Popliteal Cyst and Associated Intra-articular Knee Disorders in Adults. A r t h r o s c o p y, 15-4:368- 372,1999.
25) Sansone V. De Ponti A, Minio Paluello G and Del Maschio A.: Popliteal cysts and intra-articular disor- ders of the knee: critical reexamination based on magnetic resonance imaging. Int Orthop 1 9 : 2 7 5 - 279, 1995.
26) Stone KR, Stoller D. De Cari A, et al: The fre- quency of Baker’s cysts associated with meniscal tears. Am J Sports Med 24: 670-671, 1996.
27) Vahvanen V: Popliteal cyst. A follow-up study on 42 operatively treated patients. Acta Orthop Scand 44:303-310, 1973.
─ Abstract ─
Arthroscopic Decompression and Shaving of Popliteal Cyst Using Posteromedial Portal
-Technical Note-
Jin Hwan Ahn, M.D., Yong Jin Cho, M.D.*, Sang Hun Ko, M.D.†, Jun Sik Park, M.D., Hyo Kon Kim, M.D.
Departments of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University, Seoul, Korea, Department of Orthopedic Surgery, ChungMu Hospital, Cheonan, Korea*,
Department of Orthopedic Surgery, Ulsan University College of Medicine, Ulsan, Korea†
P u r p o s e: To present the surgical procedure of arthroscopic decompression and shaving of popliteal cyst using posteromedial portal.
Operative technique: After diagnostic knee arthroscopic examination, if there is associated intra-artic- ular pathology with popliteal cyst, appropriate arthroscopic procedure has to be performed to adress the associated intra-articular pathology. It is the most important procedure to find the opening of connection between joint cavity and popliteal cyst at posteromedial compartment using anterolateral or posteromedial portal.
In some cases the capsular fold overlie the opening of connection, so thorough diagnostic examnation is mandatory. When the opening of connection is visualized, it is enlarged about 8 mm by the arthroscopic decompressive procedure of popliteal cyst using arthroscopic shaver which is approached via the postero- medial portal. After then arthroscope is positioned at posteromedial portal and advanced into popliteal cyst via enlarged opening to visualize the inside of popliteal cyst. While visualizing the inside of popliteal cyst, a 18 gauge spinal needle is introduced by outside-in technique from medial side of the skin overly- ing popliteal cyst. And then we make trans-cystic portal at the site of spinal needle by incising the skin with # 11 blade and arthroscopic shaver is introduced within popliteal cyst via trans-cystic portal, and arthroscopic cystectomy is performed to shave the inner wall of popliteal cyst with arthroscopic shaver.
D i s c u s s i o n: The arthroscopic procedure for popliteal cyst is an alternative of traditional surgical removal of popliteal cyst and it is expected to diagnose and to manage associated intra-articular pathology and to perform arthroscopic decompression and cystectomy effectively using posteromedial portal.
Key Words: Popliteal cyst, Arthroscopic decompression and cystectomy, Posteromedial portal