Korean J Gastroenterol Vol. 72 No. 4, 209-212 https://doi.org/10.4166/kjg.2018.72.4.209 pISSN 1598-9992 eISSN 2233-6869
CASE REPORT
Korean J Gastroenterol, Vol. 72 No. 4, October 2018 www.kjg.or.kr
면역저하자 환자에서 발생한 무증상 비장낭종 1예
황현중, 백명기, 김범수, 김유진, 강석형
가톨릭관동대학교 의과대학 가톨릭관동대학교 국제성모병원 소화기내과
Asymptomatic Splenic Cysts in an Immunocompromised Patient: Should They Be Investigated
Hyunjung Hwang, Myong Ki Baeg, Pumsoo Kim, Yu Jin Kim and Seok Hyung Kang
Division of Gastroenterology, Department of Internal Medicine, Catholic Kwandong University, International St. Mary's Hospital, College of Medicine, Catholic Kwandong University, Incheon, Korea
Splenic abscess is a rare disease that generally occurs in immunocompromised patients. It is difficult to distinguish between splenic abscesses and cysts using imaging studies, especially if they are asymptomatic. A 50-year-old asymptomatic man who had received steroid therapy for underlying rheumatoid arthritis was referred to a university hospital due to presence of several splenic cysts, with the largest being 3.5 cm in diameter. Percutaneous aspiration was performed, and fluid analysis showed cysts infected by ex- tended-spectrum, beta-lactamase-producing Escherichia coli. The patient was treated with ertapenem for four weeks, and the lesion disappeared on follow-up imaging studies. Splenic abscess should be included as a differential diagnosis of splenic cystic lesions in immunocompromised patients. (Korean J Gastroenterol 2018;72:209-212)
Key Words: Splenic cyst; Splenic abscess; Arthritis, rheumatoid; Percutaneous drainage
Received February 14, 2018. Revised May 2, 2018. Accepted May 15, 2018.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2018. Korean Society of Gastroenterology.
교신저자: 백명기, 22711, 인천시 서구 심곡로100번길 25, 가톨릭관동대학교 국제성모병원 소화기내과
Correspondence to: Myong Ki Baeg, Division of Gastroenterology, Department of Internal Medicine, Catholic Kwandong University, International St. Mary’s Hospital, 25 Simgok-ro 100beon-gil, Seo-gu, Incheon 22711, Korea. Tel: +82-32-290-2923, Fax: +82-32-2290-3879, E-mail: [email protected], ORCID: https://orcid.org/
0000-0002-4807-2447
Financial support: None. Conflict of interest: None.
INTRODUCTION
Splenic abscess is a rare disease, with a rate of 0.05-0.7%
in autopsy studies.1 Splenic abscesses generally occur in pa- tients with immunodeficiency syndrome, chemotherapy, cancer, bone marrow and solid organ transplantation, long-term steroid use, monoclonal antibody use, use of immunosuppressive med- ications, and other conditions, including diabetes mellitus and alcoholism.2 The most common symptoms of splenic abscess are fever (85.1%), left upper quadrant pain (43.3%), and diffuse abdominal pain (14.9%). Physical examination often reveals splenomegaly (50.7%), left upper quadrant tenderness (44.7%), generalized abdominal tenderness (13.4%), and leu-
kocytosis (70.1%).1 The incidence of splenic abscess is thought to be increasing, which may be attributed to increased preva- lence of immunodeficiencies, such as chronic corticosteroid use, aggressive chemotherapy, or organ transplantation.3 The management of splenic abscess usually gives good results and is based on medical therapy with antibiotics and splenec- tomy or percutaneous drainage.4 Successful treatment de- pends on patient's comorbidities, general condition, and the size and topography of abscess.5 Empiric broad-spectrum anti- biotic therapy plays a primary role in the management of splenic abscesses. Percutaneous drainage has been accepted as an effective and less invasive treatment compared with surgical treatment in some patients because such drainage preserves
210 황현중 등. 면역저하자 환자의 무증상 비장낭종 1예
The Korean Journal of Gastroenterology
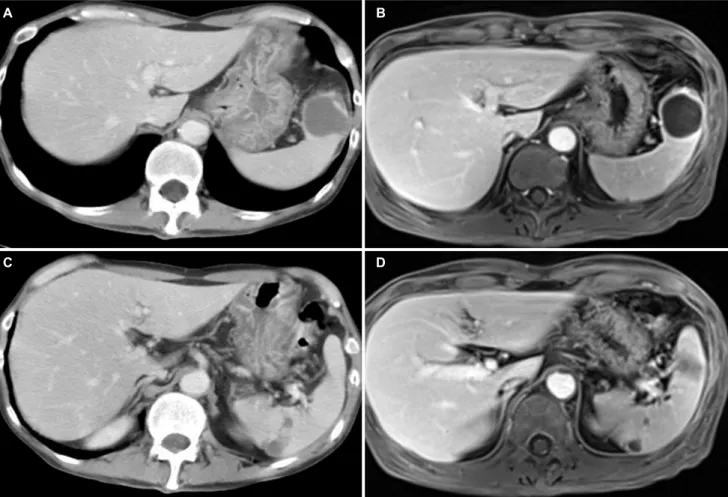
Fig. 1. APCT and MRI showed that 3.5 cm well-capsulized cystic lesion with internal debris in the spleen (A, B) and multifocal lenticular shaped and cystic changes in the periphery of the spleen (C, D). APCT, abdominal-pelvic computed tomography; MRI, magnetic resonance imaging.
the spleen and avoids the risk of overwhelming post- splenectomy sepsis.
CASE REPORT
A 50-year-old man was referred to a university hospital for further evaluation of splenic cysts. He had underlying rheuma- toid arthritis that had been treated with methotrexate, sulfasa- lazine, hydroxychloroquine, methylprednisolone, and non-ster- oidal anti-inflammatory drugs for 10 years. He had a history of previous cholecystectomy, which had been performed 8 years ago. He had no neurological, rheumatological, oph- thalmologic, or dermatological symptoms. Physical examina- tion revealed normal blood pressure and body temperature, no abdominal tenderness, and no hepatosplenomegaly.
Laboratory examination indicated no leucocytosis (white blood count of 7.43 103/μL), elevated erythrocyte sed- imentation rate of 15 mm/h, and decreased albumin level
of 2.31 g/dL. Abdominal-pelvic computed tomography, which was taken at the referring hospital, revealed a 3.5 cm cystic lesion with an internal debris in the spleen anterior pole with multifocal lenticular shaped cystic changes in the spleen periphery. The primary differential diagnosis was hemorrhagic cystic degeneration as a sequalae of focal splenic infarct with cystic lymphangioma. However, due to poor image quality, and the presence of internal debris and periphery lesions, liver magnetic resonance imaging was performed for differential diagnosis and showed a 3.5 cm well-capsulized cystic lesion with internal debris and other smaller cystic lesions in the spleen (Fig. 1). The main differential diagnosis using the MRI were cystic lymphangioma, cystic degeneration of other un- usual splenic lesion, or splenic infarct sequalae.
However, given that our patient was immunocompromised, there was a small possibility of splenic abscess. Therefore, the patient underwent ultrasound-guided and fluoroscopic percutaneous catheter drainage for diagnosis and treatment
A
A BB
C
C DD
Hwang H, et al. Asymptomatic Splenic Cyst in a Immunocompromised Subject 211
Vol. 72 No. 4, October 2018
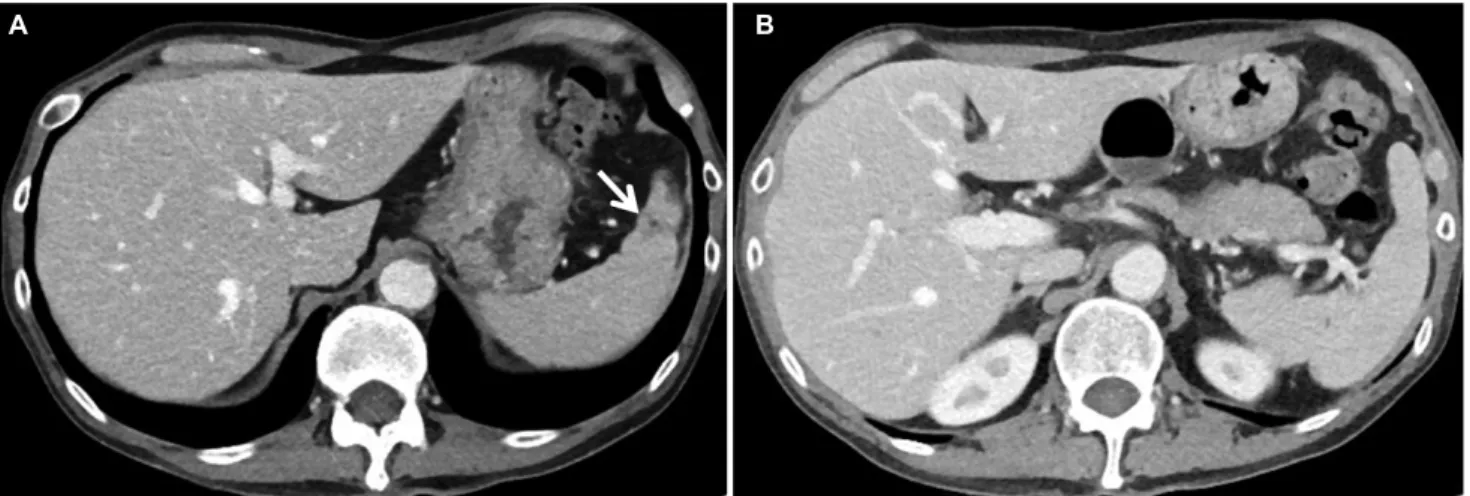
Fig. 2. APCT after one month's treatment showed nearly complete resolution of previous 3.6 cm cystic lesion in the spleen anterior pole, except a tiny 3 mm sized remnant hypodense lesion (A, arrow) and complete disappearance of peripherally multi-located low attenuation in the spleen (B). APCT, abdominal-pelvic computed tomography.
of splenic cyst. Aspiration fluid analysis revealed a turbid, neutrophil-dominant fluid. Our patient developed high fever 12 hours after percutaneous catheter drainage. Blood cul- tures were performed, and intravenous ceftriaxone and met- ronidazole were administered. Extended-spectrum beta-lacta- mase-producing Escherichia coli was cultured in the aspira- tion fluid, and ertapenem was administered for a period of 4 weeks. Follow-up abdominal-pelvic computed tomography showed that splenic infected cysts nearly disappeared after 4 weeks (Fig. 2).
DISCUSSION
Splenic abscess is considered an uncommon entity that has recently been increasing in frequency. This is likely due to increased number of immunocompromised and cancer patients.6 Splenic abscesses are often misdiagnosed because the signs and symptoms are nonspecific as in this case, which had no general symptoms like fever or abdominal pain.
Immunocompromised states may increase the risk of infection and can lead to disease progression, sepsis, and even death.
In the case of splenic cystic lesions, management is based upon both clinical history and imaging studies. Usually, if cystic lesion with benign imaging characteristics (e.g., either a cyst or a homogenous, low-attenuated lesion with no enhance- ment and smooth margins) is detected in an asymptomatic patient, further evaluation and follow-up imaging are not usu- ally required. However, if CT findings are inconclusive, MRI can be performed with follow-up imaging at 6-12 months after
the initial assessment of growth.7 In cases where differential diagnosis for infection or neoplasm are needed, needle aspi- ration may be considered. Although needle aspiration of the spleen is reluctantly performed, due to the perceived risk of bleeding and difficulty of access, it has been shown to be relatively safe with high specificity.8 In immunocompromised cases, such as ours, either the close, short-term clinical fol- low-up with imaging or diagnostic needle aspiration should be considered. Splenic abscesses are usually not diagnosed by radiologic findings, but in conjunction with clinical presentations. Isolated splenic abscesses are rare and more commonly found with concomitant hepatic abscesses, which were absent in our patient. CT findings of splenic abscess usually show hypoattenuation of the nodules, suggesting necrosis. There may also be wedge-shaped, low attenuation lesions representing infarcts due to septic emboli. When ab- scesses become organized and encapsulated, there may be peripheral enhancement of postcontrast images with en- hancement of septations,9,10 which were not found in this case. Infectious lesions are similar to simple cysts or cystic lymphangioma on MRI as they are typically hypo to isointense on T1 weighted imaging and hyperintense on T2 weighted imaging.9 However, infectious lesions or cystic lymphangiomas differ from simple cysts as they are sometimes presented with possible capsule or septation enhancement.11
Organisms associated with splenic abscesses are gram-pos- itive cocci (Streptococci, Staphylococci), gram-negative bacilli (Escherichia coli, Klebsiella pneumoniae), anaerobes, and fungi. Klebsiella pneumoniae and Escherichia coli have been
A
A BB
212 황현중 등. 면역저하자 환자의 무증상 비장낭종 1예
The Korean Journal of Gastroenterology
reported to occur frequently in Southeast Asia.12 Considering the increase in extended-spectrum beta-lactamases-producing microbes in recent years, as well as the fact that these usually occur in immunocompromised patients, carbapenems (imipenem, meropenem, doripenem, and ertapenem) should be considered as the first-line treatment.13
Successful immune suppression may prevent an upregu- lated host response to serious infections and lead to sepsis.14 In a case without septic conditions, appropriate treatments, such as percutaneous drainage and antibiotics can treat splenic abscess concurrently without interruption of dis- ease-modifying antirheumatic drugs.
The number of immunocompromised patients is increasing, and their symptoms may be nonspecific. Furthermore, radio- logical findings often have substantial overlap, which pre- cludes a specific diagnosis of simple cyst or abscess on the basis of imaging findings alone.11 Splenic abscess should be considered in the differential diagnosis of splenic cystic le- sions in immunocompromised patients, especially in lesions accompanied by internal debris or peripheral splenic infarcts.
REFERENCES
1. Chou YH, Hsu CC, Tiu CM, Chang T. Splenic abscess: sonographic diagnosis and percutaneous drainage or aspiration. Gastrointest Radiol 1992;17:262-266.
2. Ng KK, Lee TY, Wan YL, et al. Splenic abscess: diagnosis and management. Hepatogastroenterology 2002;49:567-571.
3. Green BT. Splenic abscess: report of six cases and review of the literature. Am Surg 2001;67:80-85.
4. de Bree E, Tsiftsis D, Christodoulakis M, Harocopos G, Schoretsanitis G, Melissas J. Splenic abscess: a diagnostic and
therapeutic challenge. Acta Chir Belg 1998;98:199-202.
5. Schiavo L, Scalera G, De Sena G, Ciorra FR, Pagliano P, Barbarisi A. Nonsurgical management of multiple splenic abscesses in an obese patient that underwent laparoscopic sleeve gastrectomy:
case report and review of literature. Clin Case Rep 2015;3:
870-874.
6. Tung CC, Chen FC, Lo CJ. Splenic abscess: an easily overlooked disease? Am Surg 2006;72:322-325.
7. Heller MT, Harisinghani M, Neitlich JD, Yeghiayan P, Berland LL.
Managing incidental findings on abdominal and pelvic CT and MRI, part 3: white paper of the ACR incidental findings committee II on splenic and nodal findings. J Am Coll Radiol 2013;10:
833-839.
8. Keogan MT, Freed KS, Paulson EK, Nelson RC, Dodd LG.
Imaging-guided percutaneous biopsy of focal splenic lesions: up- date on safety and effectiveness. AJR Am J Roentgenol 1999;
172:933-937.
9. Gaetke-Udager K, Wasnik AP, Kaza RK, et al. Multimodality imag- ing of splenic lesions and the role of non-vascular, image-guided intervention. Abdom Imaging 2014;39:570-587.
10. Ricci ZJ, Oh SK, Chernyak V, et al. Improving diagnosis of atrau- matic splenic lesions, part I: nonneoplastic lesions. Clin Imaging 2016;40:769-779.
11. Urrutia M, Mergo PJ, Ros LH, Torres GM, Ros PR. Cystic masses of the spleen: radiologic-pathologic correlation. Radiographics 1996;16:107-129.
12. Lee WS, Choi ST, Kim KK. Splenic abscess: a single institution study and review of the literature. Yonsei Med J 2011;52:
288-292.
13. Shakya P, Shrestha D, Maharjan E, Sharma VK, Paudyal R. ESBL production among E. coli and klebsiella spp. Causing urinary tract infection: a hospital based study. Open Microbiol J 2017;
11:23-30.
14. Richter A, Listing J, Schneider M, et al. Impact of treatment with biologic DMARDs on the risk of sepsis or mortality after serious infection in patients with rheumatoid arthritis. Ann Rheum Dis 2016;75:1667-1673.