서 론
2009년부터 한국에서 10–19세 사망 원인의 1위는 자살로, 2015년 표준인구 10만 명당 4.2명의 청소년이 자살로 목숨을 잃었다.1) 청소 년 자살의 위험 인자는 복합적이며 다차원적이다.2) 주요 인자로는 우울증, 조현병, 외상 후 스트레스 장애, 수면 장애, 물질 남용 같은
정신과적 질환이 있고, 따돌림 등 생활 사건, 만성 신체 질환 등이 있 다.3) 한편 사회 인구학적 요소로는 가족의 사회경제적 상태, 가족력, 부모 이혼 여부 등 가족 환경요인도 청소년들의 자살에서 중요한 위 험인자로 작용한다.4) 가족의 지지 효과 중 부모의 사회적 지지의 청 소년 자살 예방 효과에 대해 알려진 연구는 많지만,5-9) 형제 유무에 따른 자살 예방적 효과에 대해서는 기존에 알려진 연구가 적고 정확
Received February 23, 2017 Revised April 14, 2017 Accepted May 26, 2017 Corresponding author Jungkwon Lee
Tel: +82-2-3410-2441, Fax: +82-2-3410-0388 E-mail: [email protected]
Copyright © 2017 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2017.7.5.660 eISSN 2233-9116
Korean J Fam Pract. 2017;7(5):660-666
Korean Journal of Family Practice
KJFP
형제 유무와 청소년 우울증상 및 자살 시도와의 관련성:
청소년 건강행태 온라인조사(2015년) 이용
강소연, 이정권*, 고현영, 강윤화, 최인영, 최송화
성균관대학교 의과대학 삼성서울병원 가정의학교실
Associations between Having Siblings and Adolescent Depressive Symptoms and Suicidal Attempts among Korean Adolescents: The 2015 Korean Youth’s Risk Behavior Survey
Soyeon Kang, Jungkwon Lee*, Hyeonyoung Ko, Yunhwa Kang, Inyoung Choi, Songhwa Choi
Department of Family Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Background: The high prevalence of suicide and depression among adolescents is one of the greatest problems in South Korea. There is a lack of research on how siblings influence the prevalence of suicide and depression among Korean adolescents. This study investigated the relationships between having siblings, depressive symptoms, and suicide attempts among Korean adolescents.
Methods: The study subjects were 68,043 Korean adolescents who participated in the Korea Youth Risk Behavior Survey in 2015. We used multiple logistic regression analysis to evaluate the relationships between having siblings and adolescent depressive symptoms and suicide attempts. The following factors were included as covariates: demographic factors (age, sex, economic status, and living arrangements), physical health factors (health condition and effort to reduce weight), mental health factors (sleep satisfaction and stress), and behavioral problems (school violence, drinking, smoking, vaping, and school performance).
Results: The mean (±standard error) age of study subjects was 15.1±0.2 years, and 52.1% were male. A total of 15,894 (23.6%) had depressive symptoms for more than 2 weeks and 1,662 (2.4%) had attempted suicide within the last year. Compared to participants who had siblings, only children had greater odds of depressive symptoms (odds ratio [OR], 1.11; 95% confidence interval [CI], 1.05–1.19) and suicide attempts (OR, 1.19;
95% CI, 1.04–1.36) after adjusting for all covariates.
Conclusion: Having siblings was associated with lower odds of depressive symptoms and suicide attempts among Korean adolescents. These findings suggest that further effort to prevent suicide should be made for adolescents with depressive symptoms and those who have attempted suicide in the past.
Keywords: Republic of Korea; Adolescent; Siblings; Only Child; Depressive Symptoms; Suicide Attempted
강소연 외. 형제 유무와 청소년 우울증상 및 자살 시도와의 관련성
Korean Journal of Family PracticeKJFP
히 형제 유무에 따른 효과보다는 출생 순위10,11) 또는 형제 수12-14)에 관한 연구가 주를 이룬다. 한국 출생아 중 외동의 비율은 1981년 7%
에서 2015년 14%로 증가하는 추세에 있다.2) 저출산이 또 다른 사회 적 문제로 대두되고 있는 상황에서 외동이 증가함에도 불구하고, 형 제의 존재가 청소년 자살 또는 자살의 주요 위험인자인 우울에 예방 적 효과를 지니는 것에 대한 연구는 부족한 실정이다.4,15,16) 또한, 현재 국내에는 형제 유무와 자살의 연관성을 알아본 연구는 없다. 이에 본 연구에서는 형제 유무와 청소년 우울증상 및 자살 시도와의 관 련성을 조사하였다.
방 법
1. 연구 대상
본 연구는 제11차(2015년) 청소년 건강행태 온라인조사 원시자료 15)를 사용하였다. 이 조사는 정부 승인통계(승인번호 11,758호) 조사 로 교육부, 보건복지부, 질병관리본부 주관으로 시행되었다. 제11차 는 2015년 6월 1일부터 7월 28일까지 전국 중학교 1학년부터 고등학 교 3학년 재학생을 대상으로 지역군 및 학교 유형에 따라 층화하였 다. 층화집락추출법을 사용하여 표본 추출하여 중학교 400개교, 고 등학교 400개교 총 800개교의 70,362명을 대상으로 조사하였으며, 797개교, 68,043명이 조사에 참여하여 96.7%의 참여율을 보였다. 14 개 영역 125개 문항에 대하여 인터넷이 가능한 학교 컴퓨터실에서 표본 학급의 전원을 대상으로 1인 1대 컴퓨터를 배정하고, 무작위로 자리를 배치하여 익명성 자가 기입식 온라인 조사방법으로 수행하 였다.
본 연구는 연구자 소속 기관의 기관윤리심의위원회(Institutional Review Board, IRB)를 통과하였다(IRB no. 2016-11-041).
2. 변수의 정의
종속 변수인 우울증상이 있는 청소년은 ‘최근 12개월 동안, 2주 내 내 일상생활을 중단할 정도로 슬프거나 절망감을 느낀 적이 있었습 니까?’라는 질문에 ‘최근 12개월 동안 있다.’라고 대답한 경우로 정의 하였다. 자살 시도를 해본 청소년은 ‘최근 12개월 동안, 자살을 시도 한 적이 있었습니까?’라는 질문에 ‘최근 12개월 동안 있다’라고 대답 한 경우로 정의하였다.
형제 여부는 현재 함께 살고 있지 않은 가족도 포함하여 현재 가 족 구성원을 모두 표시하라는 항목에서 ‘형, 누나, 오빠, 언니’라는 항 목에 대답하거나 ‘남동생 또는 여동생’이라는 항목에 표시한 경우를 형제가 있는 청소년 군으로 정의하였고 그렇지 않은 군을 외동 군으 로 정의하였다.
위 종속변수와 독립변수에 관련된 교란변수로는 인구학적 요소 에서 연령, 성별, 가정의 경제적 상태, 가족 동거 여부로 지정하였다.
연령, 성별, 가정의 경제적 상태는 각 항목에 자가 기입한 답변을 변 수로 삼았고 가족 동거 여부는 가족과 함께 살고 있다고 답변한 군 과 그 외의 답변을 한 군으로 나누었다. 신체적 건강상태에서는 주관 적 건강상태 인지, 체중조절을 위한 노력 여부로 지정하였다. 주관적 건강상태 인지는 실제 질병 여부와 관계없이 본인이 주관적으로 인 지하고 있는 건강상태를 5점 척도로 표현하였다. 체중조절을 위한 노력에 대해서는 최근 30일 동안, 체중을 조절하기 위해 별다른 노력 을 하지 않았다고 대답한 군과 그 외의 답변을 한 군으로 나누었다.
정신적 건강상태는 수면에 대한 만족도와 스트레스 인지 정도를 교 란변수로 삼았는데, 수면에 대한 만족도는 ‘최근 7일 동안, 잠을 잔 시 간이 피로회복에 충분하다고 생각합니까?’라는 질문에 대한 답변을 기준으로 5개의 군으로 나누었다. 스트레스 인지 정도 또한, 자가 기 입한 답변을 기준으로 분류하였다. 문제 행동에 관해서는 학교 폭 력, 음주, 흡연, 전자담배 사용, 학업성적을 교란변수로 지정하였다.
학교 폭력은 ‘최근 12개월 동안, 친구, 선배, 성인에게 폭력을 당해 병 원에서 치료를 받은 적이 있습니까?’라는 항목에 1번 이상으로 기입 한 군을 학교 폭력을 당한 군으로 정의하였다. 음주는 ‘제사, 차례 혹 은 종교의식 때 몇 모금 마셔본 것을 제외하고 지금까지 1잔 이상 술 을 마셔본 적이 있습니까?’라는 질문에 ‘있다’라고 대답한 경우로 지 정하였다. 흡연, 전자담배 사용도 같은 방법으로 정의하였다. 학업성 적은 자가 기입한 답변을 기준으로 5개의 군으로 나누었다.
3. 자료분석 방법
제11차(2015년) 청소년 건강행태 온라인조사 원시자료는 복합 표 본 설계된 자료임을 고려하여 질병관리본부에서 산출한 가중치를 적용하였다.
종속변수의 유무에 따른 연구 대상자의 특성의 빈도와 백분율을 비교에는 카이제곱검정을 이용하였다. 형제 유무와 각각 우울증상 여부 또는 자살 시도 여부의 관련성은 로지스틱 회귀분석을 이용하 여 분석하였다. 모델 1은 연령, 성별, 가정의 경제적 상태, 가족 동거 여부로 보정하였고, 모델 2로 모델 1의 보정변수와 신체적 건강상태, 정신적 건강상태, 문제행동 보정한 후 다변량 로지스틱 회귀분석을 하였다. 형제 유무에 따른 자살 시도 여부는 우울증상 여부와 달리 모델 1, 2 분석 시 추가로 우울증상까지 보정하여 분석하였다. 모든 분석은 5% 유의수준에서 양측검정을 시행하였고, PASW statistics 18.0 (IBM Co., Armonk, NY, USA)를 이용하였다.
Original Article
Korean Journal of Family Practice
Soyeon Kang, et al. Having Siblings and Adolescent Depressive Symptoms and Suicidal Attempts
Korean Journal of Family Practice
KJFP
결 과
본 연구 대상자들의 일반적 특성은 Tables 1, 2와 같다.
총 대상자는 68,043명으로 총 대상의 평균 나이는 15.1±0.2세였다.
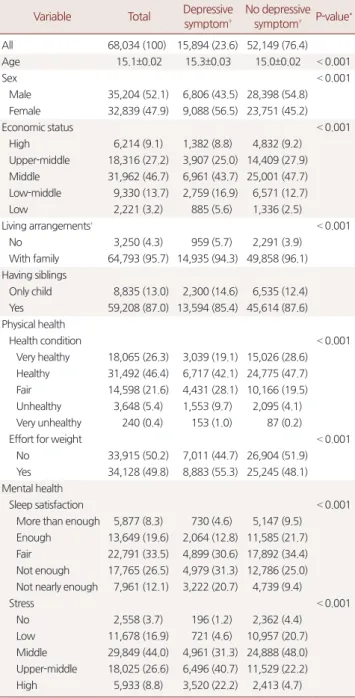
총 대상자의 23.6%가 지난 12개월 동안 2주 내내 일상생활을 중단할 정도의 슬프거나 절망감을 느낀 우울증상이 있었다고 답했다. 우울 증상은 높은 연령, 여성, 낮은 집안 경제상태, 가족과 동거하지 않는 경우, 외동인 경우에서 높게 나타났다. 신체적 건강상태(주관적인 건
강상태 또는 체중 조절을 위한 노력)나 정신적 건강상태(수면의 만 족도 또는 스트레스 인지) 모두 우울증상이 있는 군에서 나쁜 결과 를 보였다. 또한, 문제행동 항목에서도 우울증상을 가진 청소년들이 학교폭력, 음주, 흡연, 전자담배 경험률이 유의하게 높았고, 학업 성 적이 낮은 경향을 보였다.
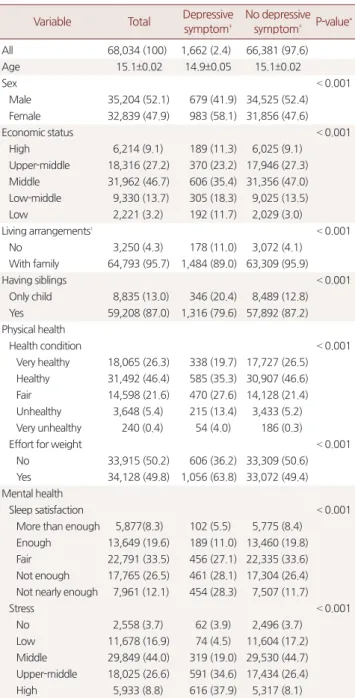
Table 2에서 나타난 자가 기록한 자살 시도 여부에 따른 대상자 특 성 차이는 약간 다르긴 하지만 전체적으로는 자가 기록된 우울증상 여부에 따른 차이와 비슷한 흐름을 보였다. 총 대상자의 2.4%가 지난 12개월 동안 자살을 시도한 적이 있다고 대답했다. 우울증상과 다르 게 자살 시도를 한 적이 있는 경우에서 평균 연령이 더 낮았으며 집 안 경제 상태가 낮은 군뿐만 아니라 가장 높은 군에서의 비율도 더 높았다. 여성, 가족과 동거하지 않는 경우, 외동인 경우에서 높게 나 타났으며 그 비율은 20.4%로 우울증상을 갖고 있지 않은 군에서 비 율인 12.8%보다 높았다.
신체적 건강상태(주관적인 건강상태 또는 체중조절을 위한 노력) 또는 정신적 건강상태(수면의 만족도 또는 스트레스 인지) 모두 자 살 시도를 해 본 군에서 나쁜 결과를 보였다. 문제 행동에서는 자살 시도를 해본 청소년들이 학교폭력, 음주, 흡연, 전자담배 경험률이 유의하게 높았고 학업 성적은 가장 낮거나 가장 높은 군에서 높게 나타나는 경향을 보였다.
Table 1. Comparison of characteristics of participants by self-reported
symptom of depression
Variable Total Depressive symptom‡
No depressive symptom‡ P-value*
All 68,034 (100) 15,894 (23.6) 52,149 (76.4)
Age 15.1±0.02 15.3±0.03 15.0±0.02 < 0.001
Sex < 0.001
Male 35,204 (52.1) 6,806 (43.5) 28,398 (54.8) Female 32,839 (47.9) 9,088 (56.5) 23,751 (45.2)
Economic status < 0.001
High 6,214 (9.1) 1,382 (8.8) 4,832 (9.2) Upper-middle 18,316 (27.2) 3,907 (25.0) 14,409 (27.9) Middle 31,962 (46.7) 6,961 (43.7) 25,001 (47.7) Low-middle 9,330 (13.7) 2,759 (16.9) 6,571 (12.7)
Low 2,221 (3.2) 885 (5.6) 1,336 (2.5)
Living arrangements† < 0.001
No 3,250 (4.3) 959 (5.7) 2,291 (3.9)
With family 64,793 (95.7) 14,935 (94.3) 49,858 (96.1) Having siblings
Only child 8,835 (13.0) 2,300 (14.6) 6,535 (12.4) Yes 59,208 (87.0) 13,594 (85.4) 45,614 (87.6) Physical health
Health condition < 0.001
Very healthy 18,065 (26.3) 3,039 (19.1) 15,026 (28.6) Healthy 31,492 (46.4) 6,717 (42.1) 24,775 (47.7) Fair 14,598 (21.6) 4,431 (28.1) 10,166 (19.5) Unhealthy 3,648 (5.4) 1,553 (9.7) 2,095 (4.1) Very unhealthy 240 (0.4) 153 (1.0) 87 (0.2)
Effort for weight < 0.001
No 33,915 (50.2) 7,011 (44.7) 26,904 (51.9) Yes 34,128 (49.8) 8,883 (55.3) 25,245 (48.1) Mental health
Sleep satisfaction < 0.001
More than enough 5,877 (8.3) 730 (4.6) 5,147 (9.5) Enough 13,649 (19.6) 2,064 (12.8) 11,585 (21.7) Fair 22,791 (33.5) 4,899 (30.6) 17,892 (34.4) Not enough 17,765 (26.5) 4,979 (31.3) 12,786 (25.0) Not nearly enough 7,961 (12.1) 3,222 (20.7) 4,739 (9.4)
Stress < 0.001
No 2,558 (3.7) 196 (1.2) 2,362 (4.4)
Low 11,678 (16.9) 721 (4.6) 10,957 (20.7) Middle 29,849 (44.0) 4,961 (31.3) 24,888 (48.0) Upper-middle 18,025 (26.6) 6,496 (40.7) 11,529 (22.2) High 5,933 (8.8) 3,520 (22.2) 2,413 (4.7)
Table 1. Continued
Variable Total Depressive symptom‡
No depressive symptom‡ P-value* Behavioral problem
School violence < 0.001
No 66,486 (97.7) 15,068(94.7) 51,418 (98.6)
Yes 1,557 (2.3) 826(5.3) 731 (1.4)
Drinking < 0.001
No 40,842 (59.2) 7,847 (48.8) 32,995 (62.4) Yes 27,201 (40.8) 8,047 (51.2) 19,154 (37.6)
Smoking < 0.001
No 56,415 (82.6) 12,135 (75.9) 44,280 (84.6) Yes 11,628 (17.4) 3,759 (24.1) 7,869 (15.4)
Vaping < 0.001
No 61,388 (89.9) 13,636 (85.4) 47,752 (91.3) Yes 6,655 (10.1) 2,258 (14.6) 4,397 (8.7)
School performance < 0.001
High 8,615 (12.6) 1,678 (10.6) 6,937 (13.2) Upper-middle 17,075 (25.1) 3,515 (21.9) 13,560 (26.0) Middle 18,952 (27.9) 4,148 (26.2) 14,804 (28.5) Low-middle 15,994 (23.6) 4,164 (26.3) 11,830 (22.8) Low 7,407 (10.8) 2,389 (15.0) 5,018 (9.5) Values are presented as number (%) or mean±standard deviation.
*P-values are obtained by Chi-squre test. †Living arrangements was categorized as whom live with family or not. ‡Depressive symptom was defined that partici- pants had ever felt hopelessness or grief for more than 2 weeks so that stopped daily life in last year.
강소연 외. 형제 유무와 청소년 우울증상 및 자살 시도와의 관련성
Korean Journal of Family PracticeKJFP
형제 유무에 따른 우울증상의 오즈비(odds ratio)는 Table 3에 제시 하였다. 외동인 경우 형제를 가진 군에 비해 우울증상을 갖는 관련 성이 유의하게 높았고(오즈비, 1.20; 95% 신뢰구간, 1.15–1.27), 기본적 인 인구 특성 변수로 보정한 경우 교차비가 더 낮아지기는 하지만 여 전히 유의하게 높음을 알 수 있었다(오즈비, 1.18; 95% 신뢰구간, 1.12–
1.24). 신체적, 정신적 건강상태 및 문제행동까지 추가적으로 보정하 더라도 외동인 경우 우울증상과 관련성이 높았다(오즈비, 1.11; 95%
신뢰구간, 1.05–1.18). 형제 유무에 따른 자살 시도의 오즈비는 Table 4
에 제시하였다. 외동인 경우 형제를 가진 군에 비해 자살 시도와 관 련성이 유의하게 높음을 알 수 있었고(오즈비, 1.75; 95% 신뢰구간, 1.55–1.99), 이는 우울증상과의 관련성보다 더 크기가 컸다. 기본적인 Table 2. Comparison of characteristics of participants by self-reported
history of suicide attempted
Variable Total Depressive symptom‡
No depressive symptom‡ P-value*
All 68,034 (100) 1,662 (2.4) 66,381 (97.6)
Age 15.1±0.02 14.9±0.05 15.1±0.02
Sex < 0.001
Male 35,204 (52.1) 679 (41.9) 34,525 (52.4) Female 32,839 (47.9) 983 (58.1) 31,856 (47.6)
Economic status < 0.001
High 6,214 (9.1) 189 (11.3) 6,025 (9.1)
Upper-middle 18,316 (27.2) 370 (23.2) 17,946 (27.3) Middle 31,962 (46.7) 606 (35.4) 31,356 (47.0) Low-middle 9,330 (13.7) 305 (18.3) 9,025 (13.5)
Low 2,221 (3.2) 192 (11.7) 2,029 (3.0)
Living arrangements† < 0.001
No 3,250 (4.3) 178 (11.0) 3,072 (4.1)
With family 64,793 (95.7) 1,484 (89.0) 63,309 (95.9)
Having siblings < 0.001
Only child 8,835 (13.0) 346 (20.4) 8,489 (12.8) Yes 59,208 (87.0) 1,316 (79.6) 57,892 (87.2) Physical health
Health condition < 0.001
Very healthy 18,065 (26.3) 338 (19.7) 17,727 (26.5) Healthy 31,492 (46.4) 585 (35.3) 30,907 (46.6) Fair 14,598 (21.6) 470 (27.6) 14,128 (21.4) Unhealthy 3,648 (5.4) 215 (13.4) 3,433 (5.2) Very unhealthy 240 (0.4) 54 (4.0) 186 (0.3)
Effort for weight < 0.001
No 33,915 (50.2) 606 (36.2) 33,309 (50.6) Yes 34,128 (49.8) 1,056 (63.8) 33,072 (49.4) Mental health
Sleep satisfaction < 0.001
More than enough 5,877(8.3) 102 (5.5) 5,775 (8.4) Enough 13,649 (19.6) 189 (11.0) 13,460 (19.8) Fair 22,791 (33.5) 456 (27.1) 22,335 (33.6) Not enough 17,765 (26.5) 461 (28.1) 17,304 (26.4) Not nearly enough 7,961 (12.1) 454 (28.3) 7,507 (11.7)
Stress < 0.001
No 2,558 (3.7) 62 (3.9) 2,496 (3.7)
Low 11,678 (16.9) 74 (4.5) 11,604 (17.2) Middle 29,849 (44.0) 319 (19.0) 29,530 (44.7) Upper-middle 18,025 (26.6) 591 (34.6) 17,434 (26.4) High 5,933 (8.8) 616 (37.9) 5,317 (8.1)
Table 2. Continued
Variable Total Depressive symptom‡
No depressive symptom‡ P-value* Behavioral problem
School violence < 0.001
No 66,486 (97.7) 1,379 (82.3) 65,107 (98.1) Yes 1,557 (2.3) 283 (17.7) 1,274 (1.9)
Drinking < 0.001
No 40,842 (59.2) 759 (45.0) 40,083 (59.6) Yes 27,201 (40.8) 903 (55.0) 26,298 (40.4)
Smoking < 0.001
No 56,415 (82.6) 1,114 (66.5) 55,301 (83.0) Yes 11,628 (17.4) 548 (33.5) 11,080 (17.0)
Vaping < 0.001
No 61,388 (89.9) 1,293 (77.1) 60,095 (90.2) Yes 6,655 (10.1) 369 (22.9) 6,286 (9.8)
School performance < 0.001
High 8,615 (12.6) 220 (13.1) 8,395 (12.6) Upper-middle 17,075 (25.1) 289 (18.0) 16,786 (25.2) Middle 18,952 (27.9) 381 (22.5) 18,571 (28.1) Low-middle 15,994 (23.6) 389 (22.4) 15,605 (23.6) Low 7,407 (10.8) 383 (24.0) 7,024 (10.5) Values are presented as number (%) or mean±standard deviation.
*P-values are obtained by Chi-squre test. †Living arrangements was categorized as whom live with family or not. ‡Suicidal attempts were defined that partici- pants had ever done those in last year.
Table 3. Odds ratio†
for depressive symptom according to whether having siblings or not
Variable Unadjusted Model 1‡ Model 2§
Having siblings 1 1 1
Only child 1.21 (1.15 1.28)* 1.19 (1.12 1.24)* 1.11 (1.05 1.19)* Values are presented as odds ratio (95% confidence interval).
†Estimated by logistic regression analysis. ‡Adjusted for age, sex, economic sta- tus, living arrangements. §Adjusted for the variables in model 2, plus health con- dition, stress, sleep satisfaction, effort for weight, school violence, drinking, smoking, vaping, school performance.
*P<0.001.
Table 4. Odds ratio†
for suicide attempted according to whether hav- ing siblings or not
Variable Unadjusted Model 1‡ Model 2§
Having siblings 1 1 1
Only child 1.75 (1.55 1.99)** 1.38 (1.21 1.57)** 1.19 (1.04 1.36)* Values are presented as odds ratio (95% confidence interval).
†Estimated by logistic regression analysis. ‡Adjusted for age, sex, economic sta- tus, living arrangements. §Adjusted for the variables in model 2, plus health con- dition, stress, sleep satisfaction, effort for weight, school violence, drinking, smoking, vaping, school performance, depressive symptom.
*P<0.05, **P<0.001.
Soyeon Kang, et al. Having Siblings and Adolescent Depressive Symptoms and Suicidal Attempts
Korean Journal of Family Practice
KJFP
인구 특성 변수로 보정하거나(오즈비, 1.38; 95% 신뢰구간, 1.21–1.57) 신체적, 정신적 건강상태 및 문제행동으로 추가 보정하더라도(오즈 비, 1.19; 95% 신뢰구간, 1.04–1.36) 외동인 경우가 자살 시도와 관련성 이 있음을 알 수 있었다.
고 찰
본 연구 결과 한국 청소년에서 형제 유무와 우울증상 및 자살 시 도 사이에 연관성을 확인하였다. 우울증상, 자살 시도 모두 외동과 관련성이 높았고 자살 시도는 우울증상보다 높은 오즈비로 외동과 연관성이 더 높은 것으로 보아 외동은 자살에 더 큰 영향을 미칠 것 으로 생각된다.
자살은 국가 간 및 한 국가 내에서도 연령대별로 차이를 보인다.
한 사회의 자살 현상은 개인적인 신체적 심리적 기질이나 개인을 둘 러싸고 있는 환경만으로는 설명할 수 없는 사회적 원인, 특히 한국 에서는 연예인 자살, 대통령 자살 등 유명인의 자살에 의한 영향, 낮 은 gross domestic product (GDP) 및 낮은 GDP 성장률, 출생률 등의 영 향에서 비롯된다는 Durkheim (1897)의 주장이 있다. 그러나 국내에 서 시행한 청소년 자살의 위험요인에 관한 통합적인 검토를 시행한 한 연구17)에 의하면 청소년 자살 생각 및 자살 시도의 가장 큰 위험 요인은 우울증이라고 할 수 있다.
기존의 연구들을 살펴보면 한국 514개 고등학생을 대상으로 한 정신건강에 관한 연구에서는 외동에서 스트레스, 우울 경향이 높았 고16) 1980년대 중국의 산아제한 이후 시행된 1988년 난징연구에서도 외동이 우울 경향이 높았다.18) 덴마크 한 추적연구에서는 돈독한 형 제관계로 대변될 수 있는 쌍둥이 군이 일반 인구 군보다 자살 시도 를 적게 한다고 나와16) 이는 본 연구 결과와 일치하였다. 기존 연구들 과는 달리 본 연구에서는 청소년 우울, 자살에 영향을 주는 다양한 인자에 대해서 보정한 후에도 유의미한 결과가 나왔다. 자살 시도는 우울을 포함한 신체적 건강상태, 정신적 건강상태, 문제 행동 요인을 보정하더라도 형제 유무와 연관성이 있음을 확인할 수 있었다. 이는 단순히 형제가 공유하는 신체적 건강상태, 정신적 건강상태, 사회적 상태만으로 우울이나 자살의 경향성이 외동에 비해 낮아지는 것으 로 해석하기 어려움을 보여준다.
본 연구는 형제 유무가 어떻게 자살을 낮출 수 있는지 기전까지 밝힐 수는 없었으나 다음과 같은 요소가 관여할 것으로 추측해볼 수 있다.
생물학적 기전으로 우울증은 뇌의 세로토닌과 노르에피네프린 이 결핍된 상태로 절망감, 무기력감, 자살생각이 증가하게 된다. 세로 토닌 양이 부족하게 되면 충동성을 억제하는 능력이 저하된다.19) 청 소년기 자살은 발달 특성으로 다른 연령대와 달리20) 계획되고 예측
되는 경우가 아닌 충동성에 의한 경우가 많다.21)
인지심리학적 측면에서는 사회적 지지는 삶의 전환기에 적응을 잘 할 수 있게 도움을 주며, 정신적 외로움 및 스트레스 상황에서 스 트레스를 감소시켜7) 자살의 위험을 낮춘다. 청소년기는 여러 환경적 조건에 의해 구체적 조직사고가 발달하는 시기로, 부모로부터 정신 적으로 독립하고 또래 관계를 통해 사회성을 형성해 나가는 삶의 전 환기이다.2) 이때 자기 조절능력이나 외부 사건에 대해 대처전략은 부 족한 상태로 질풍노도의 시기라 일컬어지는 정서적 불안상태에 놓 이게 된다.22) 사회적 지지이론의 완충효과 모델에 의하면, 친밀한 대 인 관계 등의 사회적 지지는 개인이 직면한 스트레스의 영향을 줄일 수 있다.5) 1932년 대상관계이론가 Klein에 의하면 형제관계는 애착이 론에 의하면 형제는 서로에게 사회적 지지를 제공23)하여 스트레스, 우울, 자살을 예방하는 효과를 보인다. 30년간 시행한 한 국외의 전 향적 연구에서는 유아기 형제간 지지 효과가 성인에서 우울증 유병 률을 낮춘다는 연구가 있었고,24) 다른 연구에서는 심지어 부모의 지 지 효과보다도 더 연관성이 높았다고 한다.25) 형제가 있는 것은 가족 수가 많은 것으로 고립감을 감소시키고 사회적 지지를 증가시켜 자 살 예방에 효과가 있는 것으로 해석해 볼 수 있다.
또한, Alder가 출생 순위 중심으로 설명한 성격 특성에 의하면 외 동은 과잉 보호되어 응석받이인 경우가 많아 청소년기 사회적 관계 형성에 이러한 특성이 영향을 줄 수 있다고 한다. 한국에서 4개의 중, 고등학교 학생을 대상으로 시행한 설문지 형식의 청소년의 자아분 화 수준 및 가족 기능이 정신 건강에 미치는 영향을 조사한 논문에 서는 외동이 우울, 스트레스 경향이 높아 교우관계, 학교생활 만족 도, 가족생활 만족도 등 정신 건강이 가장 나쁜 것으로 밝혀졌다.26)
이 연구의 제한점은 다음과 같다. 첫째, 한 가지 질문으로 우울증 상을 물어본 것이라 정확히 청소년 우울증을 반영한다고 볼 수 없 다. 둘째로는 사용한 자료에서 자살의 중요한 위험 요인 중 하나인 정신과적 과거력이나 가족력에 대한 변수가 부족했다. 하지만 정신 과적 과거력이나 가족력은 유병률이 매우 낮기 때문에 변수가 있었 다고 하더라도 보정에 큰 영향을 주지 않았을 것으로 생각된다. 셋 째, 자가 기입식 연구로 사회적 바람직성 편견, 회상 편견 등이 작용 했을 수 있고, 인터넷을 통한 조사로 컴퓨터 사용 능력에 따라 다른 답이 기술될 수 있었다. 마지막으로 연관된 기전은 밝힐 수 없어 추 후 심층적 연구가 필요할 것으로 생각된다. 이러한 제한성에도 불구 하고 한국 청소년을 대표할 만한 대규모 인구가 포함된 자료로 연구 를 진행했으며 외동으로 태어난 것과 자살 시도 및 우울증상에 시간 적 선후관계가 분명하다는 장점이 있다.
자살을 시도하는 80% 정도에서 겪게 되는 우울증은 완치가 되지 않더라도 증상을 완화하였을 때 자살을 예방할 수 있는 것으로 보
강소연 외. 형제 유무와 청소년 우울증상 및 자살 시도와의 관련성
Korean Journal of Family PracticeKJFP
고 있고3) 이전의 자살 시도 과거력27) 및 주요 우울 장애는 청소년 자 살을 완수하는 주요 예측인자로 알려져 있다.28) 이에 본 연구는 이전 에 밝혀지지 않았던 우울증상과 자살 시도에 대한 형제 유무의 연 관성을 분석함으로써 자살 예방에 기여하고자 하였다. 향후 다양한 추가 연구를 통해 이 관련성을 매개하는 경로를 파악하여 높은 청 소년 자살 예방을 위한 보건의료 정책적인 접근이 필요하겠다.
감사의 글
We would like to thank the Korea Centers for Disease Control and Prevention for the data obtained from the Korean Youth’s Risk Behavior Survey (KYRBS) 2015.
요 약
연구배경:
최근 한국 청소년의 자살 및 우울은 심각한 문제이다. 이 전의 문헌을 고찰하였을 때 가족의 수 및 부모의 지지가 청소년 자 살 및 우울을 낮추는 것은 알려져 있으나 구체적으로 한국 청소년에 서 형제 유무와 우울 증상, 자살 시도의 관련성에 대한 연구가 없어 본 연구는 이를 분석하였다.방법:
2015년 제11차 청소년 건강행태 온라인조사에 참여한 68,043 명의 청소년을 대상으로 형제 유무와 자가 기입한 우울증상 및 자살 시도에 관해 다변량 로지스틱 회귀분석을 이용하여 관련성 분석을 시행하였다. 교란변수로는 인구학적 요소(연령, 성별, 가정의 경제적 상태, 가족 동거 여부), 신체적 건강상태 요소(주관적 건강상태 인지, 체중조절을 위한 노력 여부), 정신적 건강상태 요소(수면에 대한 만 족도, 스트레스 인지 정도), 문제 행동 요소(학교 폭력, 음주, 흡연, 전 자담배 사용, 학업성적)로 삼았다.결과:
총 대상자의 평균 나이는 15.1±0.2세였고 52.1%가 남자였다. 총 15,894명(23.6%)이 지난 12개월 동안 2주 내내 일상생활을 중단할 정 도의 슬프거나 절망감을 느낀 우울증상이 있었다고 기록했고, 1,662 명(2.4%)이 지난 12개월 동안 자살을 시도한 적이 있다고 대답하였 다. 교란변수들로 보정 후 외동인 경우 형제를 가진 군에 비해 우울 증상을 갖는 관련성이 유의하게 높았고(오즈비, 1.11; 95% 신뢰구간, 1.05–1.19) 외동인 경우 형제를 가진 군에 비해 자살 시도와 관련성이 유의하게 높음을 알 수 있었다(오즈비, 1.19; 95% 신뢰구간, 1.04–1.36).결론:
한국의 청소년에서 형제 유무는 우울증상, 자살 시도와 통계 적으로 유의한 관련성이 있음을 확인하였다. 향후 이를 매개하는 경 로를 파악하여 청소년 자살 예방을 위한 보건의료 정책적인 접근이 필요하다.중심단어:
한국; 청소년; 형제; 외동; 우울증상; 자살 시도REFERENCES
1. Statics Korea. Cause of death statics in 2015 [Internet]. Daejeon: Statistics Korea. [cited 2016 Jan 1]. Available from: http://www.kosis.kr.
2. Kim HS, Kim HS. Youth adolescence behavioral science. Ulsan: UUP; 2000.
3. O’Connor E, Gaynes BN, Burda BU, Soh C, Whitlock EP. Screening for and treatment of suicide risk relevant to primary care: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2013; 158: 741-54.
4. Agerbo E, Nordentoft M, Mortensen PB. Suicide among young people--fa- milial, psychiatric and socioeconomic risk factors. A nested case-control study. Ugeskr Laeger 2002; 164: 5786-90.
5. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psy- chol Bull 1985; 98: 310-57.
6. Lee EH, Cho YJ. Psychological process of adolescents’ suicide: the protecting effects of social support and problem-solving ability. Korean J Soc Issues 2008; 16: 105-43.
7. Kim MY. The theory of a conceptual definition and the effect of social sup- port, and the methodological issues of the effect of social support. Korean J Clin Soc Work 2005; 2: 99-121.
8. Malecki CK, Demary MK. Measuring perceived social support: develop- ment of the child and adolescent social support scale (CASSS). Psychol Sch 2002; 39: 1-18.
9. Dubow EF, Kausch DF, Blum MC, Reed J, Bush E. Correlates of suicidal ide- ation and attempts in a community sample of junior high and high school students. J Clin Child Psychol 1989; 18: 158-66.
10. Andrews JA, Lewinsohn PM. Suicidal attempts among older adolescents:
prevalence and co-occurrence with psychiatric disorders. J Am Acad Child Adolesc Psychiatry 1992; 31: 655-62.
11. Juon HS, Nam JJ, Ensminger ME. Epidemiology of suicidal behavior among Korean adolescents. J Child Psychol Psychiatry 1994; 35: 663-76.
12. Eskin M. Suicidal behavior as related to social support and assertiveness among Swedish and Turkish high school students: a cross-cultural investi- gation. J Clin Psychol 1995; 51: 158-72.
13. Kienhorst CW, de Wilde EJ, Van den Bout J, Diekstra RF, Wolters WH. Char- acteristics of suicide attempters in a population-based sample of Dutch ado- lescents. Br J Psychiatry 1990; 156: 243-8.
14. Reinherz HZ, Giaconia RM, Silverman AB, Friedman A, Pakiz B, Frost AK, et al. Early psychosocial risks for adolescent suicidal ideation and attempts. J Am Acad Child Adolesc Psychiatry 1995; 34: 599-611.
15. Tomassini C, Juel K, Holm NV, Skytthe A, Christensen K. Risk of suicide in twins: 51 year follow up study. BMJ 2003; 327: 373-4.
16. Lee YS, Kim KH, Cho YC. Relationships between mental health and psy- chosocial factors with single-child high school students in an urban city of Korea. J Prev Med Public Health 2006; 39: 419-26.
17. Jeon HJ, Bae J, Woo JM. Recent statistics and risk factors of suicide in chil- dren and adolescents. J Korean Med Assoc 2013; 56: 93-9.
18. Tseng WS, Kuotai T, Hsu J, Chiu JH, Yu L, Kameoka V. Family planning and child mental health in China: the Nanjing survey. Am J Psychiatry 1988;
145: 1396-403.
19. Mann JJ. Neurobiology of suicidal behaviour. Nat Rev Neurosci 2003; 4:
Soyeon Kang, et al. Having Siblings and Adolescent Depressive Symptoms and Suicidal Attempts
Korean Journal of Family Practice