https://doi.org/10.14734/PN.2021.32.2.75 pISSN 2508-4887•eISSN 2508-4895
Eun Hui Joo, MD, Ji Eun Ko, MD, Hee lim Lee, MD, Hyeon Chul Kim, MD, Young Ran Kim, MD, PhD Department of Obstetrics and Gynecology, CHA Bundang Medical Center, Seongnam, Korea
Retained placenta accreta is difficult to diagnose in the series of processes involved in parturition.
It is usually discovered after delivery, when massive and uncontrollable postpartum hemorrhage occurs. A histological examination of residual placental tissue is the gold standard for the diagnosis of retained placenta accreta and indicates the degree of placental invasion into the myometrium. If the placenta is forcefully removed, maternal morbidity and mortality is high. Therefore, the management is essential when the placenta cannot be delivered spontaneously or manually. We present a case of a 35-year-old woman (G4P2A1L2) who had a high risk of placenta accreta due to past history of placenta accreta and previous myomectomy. After successful delivery, the placenta was not delivered as expected. Consequently, she experienced massive post-partum hemorrhage of 1,500 mL for up to 2 days post-partum, necessary of an extensive blood transfusion. Following spontaneous vaginal delivery and a failed attempt to manually remove the placenta, a uterine artery embolization was performed, and the patient improved over a few weeks. Thus, this case was successfully managed with conservative treatment, avoiding hysterectomy or other additional surgical treatments. No secondary postpartum complications were observed, and the menstrual cycle returned to normal within 6 months.
Key Words: Placenta accrete, Postpartum hemorrhage, Conservative treatment, Uterine artery em- bolization, Maternal mortality
Introduction
Retained placenta accreta is defined as a firmly morbid adherence of placental tissue to the uterine wall that cannot be separated spontaneously postpartum.1 If left untreated, it may lead to maternal morbidity and mortality due to postpartum hemorrhage (PPH), infection, disse mi nated intravascular coagulopathy, and sepsis. These life-threatening consequences often require a hysterectomy, resulting in infertility.2 A comprehensive and multidisciplinary approach is necessary to reduce the risk of mortality and morbidity associated with retained placenta accreta. The appropriate treatment includes either conservative management of the placenta left in situ with methotrexate, uterine artery embolization (UAE), and hysteroscopic loop resection,3-5 or surgical management that mainly involves hysterectomy. Conservative treatments can be defined as all procedures aimed at avoiding peripartum hysterectomy and its consequences. Based on the consensus guidelines on conservative management des- cribed by the American College of Obstetricians and Gynecologist and the Society for Ma- ternal-Fetal Medicine for placenta accreta spectrum disorders, we suggest the ‘leaving the placenta in situ’ approach. We report the case of a patient with retained placenta accreta, with a considerable amount of residual tissue, who was treated conservatively after delivery following failed removal of a retained placenta accreta.
Received: 3 November 2020 Revised: 24 November 2020 Accepted: 29 November 2020 Correspondence to
Young Ran Kim, MD, PhD Department of Obstetrics and Gynecology, CHA Bundang Medical Center, 59 Yatap-ro, Bundang-gu, Seongnam 13496, Korea Tel: +82-31-780-5290 Fax: +82-31-780-5069
E-mail: [email protected];
Copyright© 2021 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any
Conservative Management of Retained
Placenta Accreta Postpartum
Case
This report was approved by the Institutional Review Boards (IRB) of CHA Bundang Medical Center (IRB No.2018-08-018), and written informed consent was obtained from the patient for the publication of this case report. A 35-year-old pregnant woman, G4P2A1L2, was admitted to our hospital with early intrauterine pregnancy 6+3 weeks. She had a submucosal myoma which was found following her first pregnancy and a history of two spontaneous vaginal deliveries with an emergency UAE after her second delivery. At the time of her second delivery, she experienced severe postpartum bleeding due to complications resulting from placenta accreta, therefore emergency UAE was inevitable. Her prognosis was positive however, after a month, she presented to the emergency unit complaining of recurrent vaginal bleeding. We found that remnant placental tissue was stuck in her cervical os, therefore resectoscopic removal of the placenta was scheduled. The placenta was implanted at the site of the submucosal myoma, therefore we removed the myoma with the retained placenta at the same time. The pathological findings were ‘retained placenta’ and ‘leiomyoma with infarction’
as expected. Owing to her past history, she was considered to have a higher risk of placental abnormalities compared to other normal pregnant women, therefore the physicians examined her carefully during the third trimester using an ultrasound to detect abnormalities which could induce extensive bleeding during de- livery. Classically, two-dimensional (2D) ultrasonographic fea- tures of abnormal placental invasion include 1) the presence of
an irregularly shaped placenta, 2) myometrial thinning adjacent to the placenta, and 3) loss of the retroplacental sonolucent line.
At delivery, placenta accreta can be a cause of massive post- partum bleeding. The ultrasound did not detect any signs of pla- cental invasion into the myometrium, however, the placenta was implanted at the same site as the previous placenta accreta and myomectomy site (Fig. 1) which was reasonable to suggest that there might be a high risk of recurring placenta accreta.
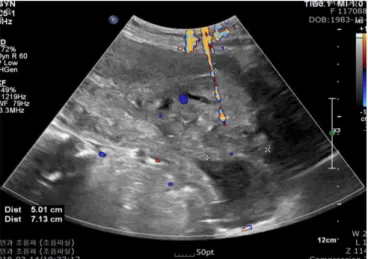
Eventually, she delivered a healthy baby (female; body weight: 2,465 g; Apgar score: 1 min, 7; 5 min, 9). However, the placenta was not spontaneously delivered as expected and the physicians attempted to remove it manually but failed. The retained placenta induced massive postpartum bleeding as the estimated blood loss was about 1,500 mL and vaginal bleeding persisted moderately. An emergency UAE was performed after careful con sideration. The partly removed placenta weighing 340 g was sent for pathological examination, and a massive transfusion (9 pints of packed red blood cells, 5 pints of fresh frozen plasma, and 20 pints of platelet concentrates) was done. The patient seemed to recover without any complications. However, for 2 days postpartum, she continued to experience moderate vaginal bleeding, causing us to assume that there might be re-bleeding from the retained placenta site. Re-embolization was performed and following the procedure, the patient recovered markedly with no other complications related to the massive transfusion and hypovolemia. On ultrasonography, the wound was evident and the remaining 7×5 cm sized placenta remained visible (Fig. 2).
A B
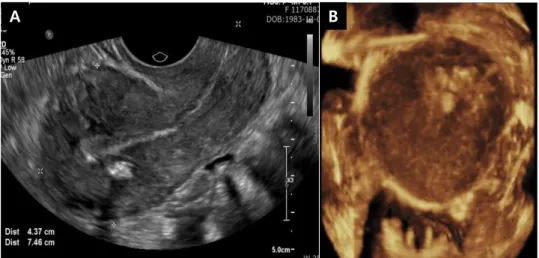
Fig. 1. (A) Ultrasonographic image showing placenta implantation at the site of submucosal myoma at early trimester. (B) Ultrasonographic image showing placenta implantation at the site of previous myomectomy site at IUP 33+6 weeks’ gestation.
very, satisfactory endometrial growth with a clear tri-layer pending normal menstruation (Fig. 4) was observed on two- dimensional and three-dimensional ultrasonography, respec- tively. However, there was still a 2.0×1.1 cm-sized remnant of the placental tissue in her uterus but it did not cause any compli- cations (Fig. 5). Therefore, we decided to observe the natural progress of placenta resorption and planned a 1-year follow-up with no additive invasive procedures.
1. Embolization Procedure
The right common femoral artery was used for arterial access.
Nonselective pelvic arteriography was performed followed by additional internal iliac arteriography. Co-axial 3 French cathe- ters (Tracker-18 Infusion Catheter; Boston Scientific, Natick, MA, USA) were advanced into the uterine artery, and emboliza- tion was performed until complete cessation of blood flow was achieved. A small amount of polyvinyl alcohol (PVA) (Contour;
Boston Scientific, Natick, MA, USA) was mixed with 40 mL of 1:1 saline-contrast mixture at the beginning of embolization (0.33 mL of dry volume in each uterine artery) and at the end point, was switched to gelfoam pledgets. The PVA particles (Contour, Boston Scientific) were 355-500 μm diameter.
Discussion
Although retained placenta ccrete is a challenging obstetric emergency, it can be sufficiently treated with conservative ma- nagement. Many articles have reported that hysterectomy cannot be avoided owing to unstable biometric signals and massive blood loss in patients which cannot be controlled with sutures or other non-invasive care.6-8 We report a case of successful treat ment of retained placenta accreta postpartum with natural progress during follow-up.
To the best of our knowledge, no other case of conservative treatment of retained placenta accreta complicated by placental adhesion to the previous myomectomy site has been reported.
Most of the reported cases were treated by caesarean hysterec- tomy or other surgical approaches. This case demonstrates a successful incident of conservative management of retained pla- centa accreta, complicated by previous myomectomy, without any invasive methods. At the time of her second pregnancy, the The final pathological examination revealed partial or com-
plete absence of the decidua basalis with adherence of the placenta directly to the superficial myometrium. This confirmed the diagnosis of retained placenta accreta (Fig. 3). No further PPH was observed, and menstrual periodicity resumed after 6 months. Beta-human chorionic gonadotropin (β-hCG) serum levels also normalized within 10 weeks. After 9 months of deli-
Fig. 2. Ultrasonographic image showing 7.13×5.01 cm sized mixed echogenic area in the anterior wall of uterus at postpartum.
Fig. 3. Magnification haematoxylin/eosin slide (×10). Partial or com- plete absence of decidua basalis with adherence of the placenta di- rectly to the superficial myometrium, which is distinctive of retained placenta accrete.
reports state that UAE could also increase the risks for malpre- sentation, preterm birth, caesarean delivery and postpartum haemorrhage.10 Our patient had experienced both UAE and re- sectoscopic myomectomy followed by the removal of the rem- nant placenta postpartum, therefore it is worth regarding as a rare but clinically important case.
The International Federation of Gynecology and Obstetrics consensus guidelines on placenta accreta spectrum disorders proposes four primary methods of conservative management.
We applied the ‘leaving the placenta in situ’ or the ‘expectant approach’ to our patient, waiting for complete spontaneous re- sorption of the retained placenta.11 Usually, UAE allows for the conservative treatment of retained placenta accreta, which helps improve the patient’s condition more rapidly.12 Assumingly, a progressive decrease in blood supply within the uterus and the placenta results in secondary necrosis of the villous tissue.
Therefore, the placenta naturally separates from the uterus, and the villi attached to adjacent pelvic organs are equally spontane- ously removed.13 An empty uterus has been observed sponta- ne ously with medical treatment in 75% of cases after a median of 13.5 weeks (range 4-60 weeks), and the residual villous tissue in the uterine wall may require up to 6 months to be completely absorbed.14,15 In rare cases, a coagulopathy or septicaemia re- quiring an emergency secondary hysterectomy may develop.12,16 Weekly measurement of serum β-hCG to check for a continuous fall can be an indicator for the remnant placenta; however, low levels do not guarantee complete placental resorption. Therefore, this should be confirmed by other examinations, such as ultra- retained placenta accreta had been treated conservatively, but
the placental attachment disorder recurred at the same site of the previous myomectomy in the subsequent pregnancy. It has been widely known that previous surgery damaging the uterus or endometrium itself is considered as a risk factor for inducing placenta accreta, although the risk is not that high.9 A previous case-report also indicated that UAE for treating myoma could be a cause of abnormal placental adherence. They explained that the mechanism of inducing placenta accreta in this case is the result of infarction of the uterine endometrium following UAE, leading to deficiency of the decidua basalis and resulting in abnormal trophoblast invasion into the myometrium. Some Fig. 5. Ultrasonographic image showing 2.02×1.08 cm sized mixed echogenic area in the posterior wall of uterus at about 9 months later.
A B
Fig. 4. (A) Two-dimensional (2D) ultrasonography after the return of menstruation. (B) Three- dimensional (3D) ultrasonography after the return of menstruation.
sound imaging.
In conclusion, while the optimal standard therapy of retained placenta accreta has not been well-established, this case sug- gests that conservative treatment without other additional treat - ment of placenta accreta should be considered alternatively prior to resorting to surgical methods. Further evaluation and analysis of the conservative treatment should be performed to clarify its effectiveness and safety.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
References
1) Zhong L, Chen D, Zhong M, He Y, Su C. Management of patients with placenta accreta in association with fever following vaginal delivery.
Medicine (Baltimore) 2017;96:e6279.
2) Wortman AC, Alexander JM. Placenta accreta, increta, and percreta.
Obstet Gynecol Clin North Am 2013;40:137-54.
3) Kreinin A, Saphier O, Silberstein T. Methotrexate treatment for retained placental tissue after second trimester termination of pregnancy. Isr Med Assoc J 2018;20:388-90.
4) Peng ZH, Xiong Z, Zhao BS, Zhang GB, Song W, Tao LX, et al. Prophylactic abdominal aortic balloon occlusion: an effective method of controlling hemorrhage in patients with placenta previa or accreta. Exp Ther Med 2019;17:1492-6.
5) Alonso L, Nieto L, Carugno J. Hysteroscopic removal of retained products of conception implanted over a focal area of adenomyosis: a case report.
J Minim Invasive Gynecol 2018;25:382-3.
6) Sheldon W, Blum J, Vogel JP, Souza JP, Gulmezoglu AM, Winikoff B, et al.
Postpartum haemorrhage management, risks, and maternal outcomes:
findings from the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG 2014;121 Suppl 1:5-13.
7) Eller AG, Porter TF, Soisson P, Silver RM. Optimal management strategies for placenta accreta. BJOG 2009;116:648-54.
8) Sichitiu J, El-Tani Z, Mathevet P, Desseauve D. Conservative surgical management of placenta accreta spectrum: a pragmatic approach. J Invest Surg 2021;34:172-80.
9) Mathiesen E, Hohenwalter M, Basir Z, Peterson E. Placenta increta after hysteroscopic myomectomy. Obstet Gynecol 2013;122(2 Pt 2):478-81.
10) Takahashi H, Hayashi S, Matsuoka K, Kitagawa M. Placenta accreta follo- wing uterine artery embolization. Taiwan J Obstet Gynecol 2010;49:197- 8.
11) Sentilhes L, Kayem G, Chandraharan E, Palacios-Jaraquemada J, Jauniaux E; FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum dis- orders: conservative management. Int J Gynaecol Obstet 2018;140:291- 8.
12) Lee HJ, Cho HY, Peck MJ, Ki HJ, Moon MJ, Kim HC, et al. Uterine artery embolization versus cesarean hysterectomy in the management of postpartum hemorrhage. Minim Invasive Ther Allied Technol 2019;28:
351-8.
13) Allen L, Jauniaux E, Hobson S, Papillon-Smith J, Belfort MA; FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO con sensus guidelines on placenta accreta spectrum disorders: noncon- servative surgical management. Int J Gynaecol Obstet 2018;140:281-90.
14) Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol 1991;77:69-76.
15) Abdel-Aleem H, Abdel-Aleem MA, Shaaban OM. Nitroglycerin for ma- nagement of retained placenta. Cochrane Database Syst Rev 2015;(11):
CD007708.
16) Tong A, Zhao F, Liu P, Zhao X, Qi X. Management of postpartum pulmo- nary embolism combined with retained placenta accreta: a case report.
Medicine (Baltimore) 2019;98:e17219.