Copyright © 2010 by The Korean Orthopaedic Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clinics in Orthopedic Surgery • pISSN 2005-291X eISSN 2005-4408
Reliability of MRI Findings of Peroneal
Tendinopathy in Patients with Lateral Chronic Ankle Instability
Hee Jin Park, MD, Seung Doh Cha, MD*, Hyung Soo Kim, MD*, Soo Tae Chung, MD*, Noh Hyuck Park, MD, Jeong Hyun Yoo, MD*, Jai Hyung Park, MD*, Joo Hak Kim, MD*,
Tae Woo Lee, MD*, Chang Hyun Lee, MD*, Se Man Oh, MD*
Departments of Radiology and *Orthopedic Surgery, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea
Background: Patients with chronic lateral ankle instability also have peroneal tendinopathy often. However, preoperative MRIs of these patients are vague in many cases. Our study was performed to see the reliability of MRI findings of peroneal tendinopathy in patients with chronic lateral ankle instability.
Methods: MRI images for 82 patients who had chronic lateral ankle instability, and had received surgical treatment between March 2006 and November 2009 were compared with impressions from operating rooms. The mean age of patients was 36.4 years (range, 15 to 64 years), 82 ankles were studied, and patients with rheumatoid diseases were excluded from the study.
Results: Of the 82 cases, 26 were true positives, 38 true negatives, 13 false positives and 5 false negatives. Of 39 cases of peroneal tendinopathy diagnosed from MRI, 14 had peroneal tendon partial tears, 15 tenosynovitis, 3 dislocations, 17 low-lying muscle bellies, and 6 peroneus quartus muscles. Of 31 cases of peroneal tendinopathy observed in surgery 11 had peroneal tendon partial tears, 4 tenosynovitis, 5 dislocations, 12 low-lying muscle belliess, and 1 peroneus quartus muscle. Sensitivity and specificity of peroneal tendinopathy were 83.9% and 74.5%, respectively. Positive predictive value was 66.7%. Negative predictive value was 88.4%. Accuracy rate was 78.0%.
Conclusions: MRI is a useful diagnostic tool for detecting peroneal tendinopathy in patients with chronic lateral ankle instability.
However, MRI is vague in many cases. Therefore, a thorough delicate physical examination and careful observation is needed.
Keywords: Peroneal tendinopathy, Chronic lateral ankle instability, MRI
Received October 26, 2009; Accepted April 13, 2010 Correspondence to: Seung Doh Cha, MD
Department of Orthopaedic Surgery, Myongji Hospital, Kwandong University College of Medicine, Goyang 410-270, Korea
Tel: +82-31-810-6530, Fax: +82-31-810-6537 E-mail: [email protected]
as a useful diagnostic tool prior to surgical intervention.
However, an unambiguous identification of the disease is difficult to obtain because of anatomical characteristics such as the oblique course of the peroneal tendon and confusion with normal variants.1,10) Our study assessed the reliability of MRI by comparing MRI findings and operative findings of peroneal tendinopathy in patients with chronic lateral ankle instability.
METHODS
Of the patients who had visited our hospital due to ankle Peroneal tendinopathy including tenosynovitis and tendon
partial tear are common in patients with chronic ankle discomfort. Instability caused by repetitive ankle sprains and peroneal dislocation following a superior peroneal retinaculum injury can coexist in some cases.1-4) The cause of peroneal tendinopathy is repetitive mechanical stress, not a traumatic injury in most cases.1,5-9) and MRI is regarded
sprains and discomfort lasting more than 6 months between March 2006 and November 2009, 82 who under- went lateral ankle reconstruction under the diag nosis of chronic lateral ankle instability based on the preoperative MRI findings were included in this study. There were 47 males and 35 females with an average age of 36.4 years (range, 15 to 64 years). A total of 82 ankles were examined (50 right and 32 left ankles). Patients with rheumatic diseases were excluded.
MRIT1- and T2-weighted sagittal and axial images were obtained using a 1.5 Tesla Phillips MRI scanner. The repetition time and echo time for the T1-weighted and T2- weighted images were 500-600 msec and 11-15 msec, and 2,000 msec and 11-15 msec, respectively. The repetition time and echo time for the T2-weighted fat suppression images were 3,400-3,600 msec and 11-15 msec. The other acquisition parameters were as follows: field of view, 150 × 150 mm; matrix size, 224 × 224; and slice thickness, 4 mm.
MRI Assessment
The MRI images obtained were assessed by two radi-
ologists using PACS (M-view ver. 5.0, Marotech, Korea).
They were unaware of the patients’ clinical symptoms and other test results.
They were asked to assess the MRI images on two occasions in two separate places without consultation or discussion with each other. The assessments were performed with an interval of two weeks and the inter- and intra-observer reliability was calculated. The patients were identified only by randomly assigned numbers.
Definition of Peroneal Tendinopathy
Peroneal tenosynovitis was defined as the appearance of fluid collection within the common peroneal tendon sheath, increased signal intensity within the tendon, or hypertrophy of the tendon on T2-weighted sagittal and axial images11,12) and observation of increased synovial fluid and thickening of the tendon and synovial sheath during surgery. The low lying peroneal muscle belly was defined as extension of the muscle belly distal to the fibular groove (Fig. 1).5,9) Dislocation of the peroneal tendon was defined as displacement of the tendon lateral to the retromalleolar groove. The peroneus quartus was defined as a an accessory muscle originating from
Fig. 1. (A) A T2-weighted axial image of an ankle MRI showing crowding of the muscle tissue of the peroneus brevis tendon within the superior peroneal retinaculum (white arrow). (B) In the same area, extension of the muscle tissue of the peroneus brevis tendon distal to the fibular groove is observed (black arrow).
Fig. 2. (A) The T2-weighted axial image of ankle MRI shows the peroneus quartus muscle at the posteromedial aspect of the peroneus tendons (white arrow). (B) In the same area, the per- oneus quartus tendon is observed (white arrow).
the lateral portion of the distal fibula and descending posteromedially to be inserted into the lateral side of the calcaneus (Fig. 2).5,13)
Surgical Findings
Patients were placed in the supine position under general anesthesia. A curve shaped skin incision extending from 2 cm superior to 2 cm inferior to the distal fibular epiphysis was made. A lateral ankle reconstruction using a modified Brostrom technique was performed to treat the chronic lateral ankle instability and ankle discomfort.
During the procedure, the peroneal tendon at the fibular groove located posterior to the distal fibular epiphysis was examined. Small incisions were made on the tendon sheath and the superior peroneal retinaculum to identify tenosynovitis, partial tears, low lying peroneal muscle belly, and peroneus quartus. Tenosynovitis and tendon tears were treated with debridement and debridement or coronal suture, respectively. For subluxation and disloca- tion of the tendon, fibular groove deepening or superior peroneal retinaculum repair were performed. Low lying peroneal muscle bellies were excised.
Statistical Analysis
All statistical analyses were conducted using SPSS ver. 12.0
(SPSS Inc., Chicago, IL, USA). Inter- and intra-observer reliability were calculated using the intraclass correlation coefficients (ICCs) introduced by Shrout and Fleiss.14) The ICCs can range from 0 (no agreement) to 1 (perfect agreement): a value of 0.00-0.39 was considered poor agreement, 0.40-0.74, moderate agreement, and 0.75-1.00, excellent agreement.
RESULTS
MRI Reliability
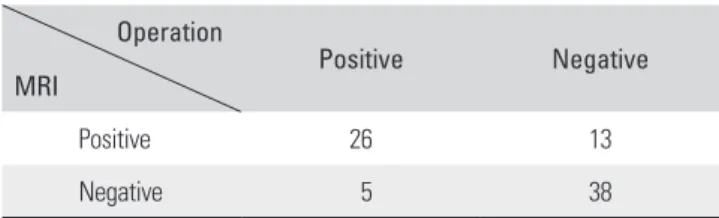
Based on the surgical findings, the MRI findings were true positive (TP), false positive (FP), true negative (TN), and false negative (FN) in 26, 13, 38, and 5, respectively, of the total 82 cases (Table 1). Accordingly, the MRI sensitivity and specificity were 83.9%, and 74.5%, respectively, with the positive predictive value (PPV), the negative pre- dictive value (NPV), and the accuracy rate being 66.7%, 88.4%, and 78.0%, respectively. Of the 39 MRI-identified peroneal lesions, a partial peroneal tendon tear, peroneal tenosynovitis, peroneal tendon dislocation, low-lying muscle belly, and peroneus quartus were observed in 14, 15, 3, 17, and 6 cases, respectively (Table 2). Of the 31 peroneal lesions identified during surgery, a partial peroneal tendon tear, peroneal tenosynovitis, peroneal tendon dislocation, low-lying muscle belly, and peroneus quartus were noted in 11, 4, 5, 12, and 1, respectively (Table 2). The MRI sensitivity, specificity, PPV, NPV, and the accuracy rate for detection of a partial tear were 54.5%, 88.7%, 42.9%, 92.6%, and 84.1%, respectively.Values for peroneal tenosynovitis detection were 25%, 95.5%, 6.7%, 82.1%, and 79.3%, respectively (Table 2).
Inter- and Intra-Observer Reliability of MRI Findings The overall intraobserver reliability was moderate, except Table 1. The Number of Positive and Negative Peroneal Tendinopathy
Patients in the MRI Group and in the Surgery Group Operation
MRI Positive Negative
Positive 26 13
Negative 5 38
Table 2. Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value, and Accuracy Rate from the Result of MRI and Operative Findings on Peroneal Tendinopathies
Sensitivity (%) Specificity (%) Positive predictive
value (%) Negative predictive
value (%) Accuracy rate (%)
Peroneal tendinopathy 83.9 74.5 66.7 88.4 78.0
Peroneal tendon tear 54.5 88.7 42.9 92.6 84.1
Peroneal tenosynovitis 25 95.5 6.7 82.1 79.3
Low-lying muscle belly 91.7 91.4 64.7 98.5 91.5
Peroneus quartus 100 93.8 16.7 100 93.9
Peroneal tendon dislocation 75 98.7 75 98.7 97.6
that it was excellent for peroneal tendinopathy (ICCs, 0.942) and peroneal tendon tear (ICCs, 0.928) for observer 2 (Table 3). The overall interobserver reliability was moderate, although it was poor for the 1st assessment of the peroneal tenosynovitis (ICCs, 0.263) (Table 4).
DISCUSSION
The peroneus longus and peroneus brevis tendons are the stabilizers of the ankle that are responsible for inversion and plantarflexion of the ankle.7) They lie lateral to the ankle and travel along the groove posterior to the distal fibular epiphysis.1,15-18) Acute tears and dislocation of the peroneal tendons are often observed in young athletes, whereas tenosynovitis and partial tears are caused mostly by repetitive mechanical stress rather than traumatic injury.1,3,5-9,19) Indeed, most patients with chronic lateral ankle instability and a partial longitudinal tear of the peroneus brevis tendon have a history of repetitive ankle sprains or an inversion trauma. The etiology of peroneal tendon partial tears is thought to be direct contact between the peroneus brevis tendon and the lateral malleolus coupled with compression from the peroneus longus tendon during contraction.8,4,20) Once a longitudinal
peroneus brevis tendon tear occurs, the peroneus longus tendon contracts and passes into the longitudinally torn peroneus brevis tendon preventing healing and causing tenosynovitis involving chronic pain, edema, and joint motion restriction.20) Low lying peroneal muscle belly causes a crowding effect in the retromalleolar groove located medial to the peroneal retinaculum, predisposing to peroneal tendinopathy or superior peroneal retinaculum injuries.5,9) Peroneus quartus is found in 13-22% of the population and typically inserts onto the retrotrochlear eminence of the lateral side of the calcaneus or onto the peroneal tubercle, although its origins and insertions are various.5,11,13,21) The presence of a peroneus quartus should be identified considering that it can be attributable to constant ankle pain, chronic lateral ankle instability, and subluxation of the peroneal tendons.
MRI is a useful diagnostic tool for detecting per- oneal tendinopathy and dysplastic variations, and pero- neal tendons can be best evaluated on T2-weighted axial images taken with the ankle slightly plantarflexed (Fig. 3).5,8,15,16,18,20,22) A normal peroneus brevis tendon is seen as round or flat shaped near the peroneal groove on axial MRI images and a peroneal tendon tear can be best detected at the tip of the lateral malleolus on axial images.2,23) A longitudinally torn peroneal brevis tendon is seen as chevron-shaped, surrounding the peroneus longus tendon, or rejoining each other at a distal site on axial images (Fig. 4).2,23,24) A normal peroneal brevis tendon can be mistaken for being partially torn when seen as chevron-shaped due to an increase in signal intensity on T1-weighted axial images, the so-called magic angle phenomenon. In such cases, T2-weighted images can be helpful. If abnormal findings are also noted on T2-weighted images, a tendon tear can be suspected.5,11,15,20) MRI is also described as a useful diagnostic modality for per oneal ten- Table 3. Intraobserver Agreement
Observer 1 Observer 2
ICC 95%
Confidence
interval ICC 95%
Confidence interval Peroneal tendinopathy 0.678 0.541-0.780 0.942 0.912-0.963 Peroneal tendon tear 0.611 0.456-0.731 0.928 0.890-0.953 Peroneal tenosynovitis 0.636 0.487-0.749 0.717 0.593-0.808 ICC: Intraclass correlation coefficient.
Table 4. Interobserver Agreement
Test 1 Test 2
ICC 95%
Confidence
interval ICC 95%
Confidence interval Peroneal tendinopathy 0.570 0.404-0.700 0.540 0.366-0.677 Peroneal tendon tear 0.474 0.287-0.626 0.459 0.270-0.614 Peroneal tenosynovitis 0.263 0.049-0.453 0.558 0.389-0.691 ICC: Intraclass correlation coefficient.
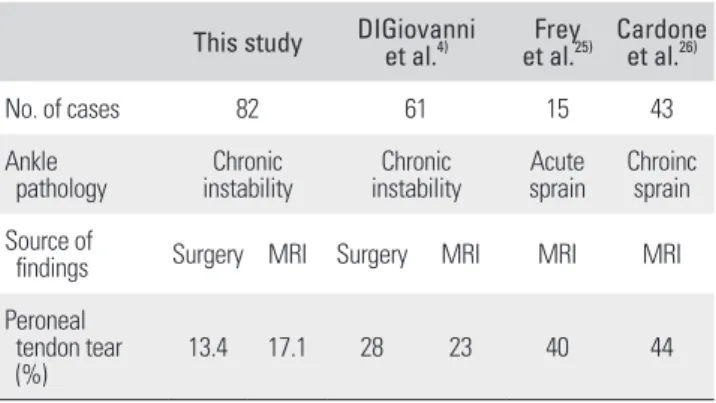
Table 5. Comparison of Lateral Ankle Instability with Associated Peroneal Tendon Tear
This study DIGiovanni
et al.4) Frey
et al.25) Cardone et al.26)
No. of cases 82 61 15 43
Ankle
pathology Chronic
instability Chronic
instability Acute
sprain Chroinc sprain Source of
findings Surgery MRI Surgery MRI MRI MRI
Peroneal tendon tear
(%) 13.4 17.1 28 23 40 44
don partial tears by DIGiovanni et al.4) (Table 5).
The positive predictive value of MRI for peroneal tendon lesions was relatively low at 66.7% whereas the
negative predictive value was fairly high at 88.4%. This was because the oblique course of the tendons was difficult to be visualized accurately by MRI. They run from the lateral side of the proximal fibula through the posterior side of the distal fibula, and MRI images of them are often misleading due to the 3-dimensional pathway. Ac- cordingly, surgeons are recommended to factor in such characteristic of the tendons in analyzing MRI images to avoid a misdiagnosis (Fig. 5). In addition, they should guard against excessive reliance on MRI because it can lead to unnecessary surgical interventions. As seen in Table 1, the total number of false positive cases (13) was equivalent to 50% of the true positive cases (26) in this study. Signs of peroneal tenosynovitis include the appearance of fluid collection within the common peroneal tendon sheath and hypertrophy of the tendon on T2-weighted sagittal and axial images.11,12) However, hypertrophy of the tendon was difficult to determine during surgery and thus the positive predictive value of MRI for tenosynovitis was lower than that for other lesions. The prevalence of peroneus quartus is known to be 13 to 22% and it was as low as 10% in a cadaver study by Cheung et al.13) Although the size of our study population limited our ability to provide a rigorous statistical prediction, the positive predictive value of MRI
Fig. 5. (A) A T2-weighted fat suppressed axial image of an ankle MRI shows a split tear of the peroneus brevis tendon (white arrows). The peroneus brevis tendon is split and is observed to have a chevron shape. (B) But, in the operative field, the peroneus brevis tendon was intact and the low-lying muscle belly of peroneus brevis muscle was observed.
Fig. 3. The normal peroneus longus and brevis tendons are observed as a tubular shaped object distal to the lateral malleolus on the T1-weighted axial image taken with the ankle slightly plantarflexed (black arrow).
Fig. 4. (A) This T2-weighted fat suppres- sion axial image of an ankle MRI shows a split tear and enlarged shape of the peroneus brevis tendon (white arrow).
Around peroneus tendons, an increase in synovial fluid is observed. (B) In the same area, a split tear of the peroneus brevis tendon and thickened synovium is observed (black arrow).
for peroneus quartus was 16.7%. Of the 82 patients, 5 had positive findings on MRI and peroneus quartus was confirmed during surgery in 1 of them. It is attributable to the fact that peroneus quartus is often confused with a peroneal tendon tear and comes in various forms.27)
In conclusion, MRI is a useful diagnostic modality for detecting peroneal tendinopathy in patients with chron ic lateral ankle instability. However, the PPV, accura- cy rate, and interobserver reliability of MRI findings were
found to be relatively low in this study. Therefore, thorough physical examinations and careful observation should also be performed in combination with MRI scanning for a definitive diagnosis of peroneal tendinopathy.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Yao L, Tong DJ, Cracchiolo A, Seeger LL. MR findings in peroneal tendonopathy. J Comput Assist Tomogr. 1995;
19(3):460-4.
2. Sobel M, Geppert MJ, Olson EJ, Bohne WH, Arnoczky SP.
The dynamics of peroneus brevis tendon splits: a proposed mechanism, technique of diagnosis, and classification of injury. Foot Ankle. 1992;13(7):413-22.
3. Ferran NA, Maffulli N. Epidemiology of sprains of the lateral ankle ligament complex. Foot Ankle Clin. 2006;11(3):659- 62.
4. DIGiovanni BF, Fraga CJ, Cohen BE, Shereff MJ. Associated injuries found in chronic lateral ankle instability. Foot Ankle Int. 2000;21(10):809-15.
5. Wang XT, Rosenberg ZS, Mechlin MB, Schweitzer ME.
Normal variants and diseases of the peroneal tendons and superior peroneal retinaculum: MR imaging features. Radi- ographics. 2005;25(3):587-602.
6. Hubbard TJ, Kramer LC, Denegar CR, Hertel J. Contrib- uting factors to chronic ankle instability. Foot Ankle Int.
2007;28(3):343-54.
7. Lee MS, Hofbauer MH. Evaluation and management of lateral ankle injuries. Clin Podiatr Med Surg. 1999;16(4):
659-78.
8. Saxena A, Pham B. Longitudinal peroneal tendon tears. J Foot Ankle Surg. 1997;36(3):173-9.
9. Tjin A Ton ER, Schweitzer ME, Karasick D. MR imaging of peroneal tendon disorders. AJR Am J Roentgenol.
1997;168(1):135-40.
10. Lamm BM, Myers DT, Dombek M, Mendicino RW, Catanzariti AR, Saltrick K. Magnetic resonance imaging and surgical correlation of peroneus brevis tears. J Foot Ankle Surg. 2004;43(1):30-6.
11. Kijowski R, De Smet A, Mukharjee R. Magnetic resonance imaging findings in patients with peroneal tendinopathy and peroneal tenosynovitis. Skeletal Radiol. 2007;36(2):105-
REFERENCES
14.
12. Gray JM, Alpar EK. Peroneal tenosynovitis following ankle sprains. Injury. 2001;32(6):487-9.
13. Cheung YY, Rosenberg ZS, Ramsinghani R, Beltran J, Jahss MH. Peroneus quartus muscle: MR imaging features.
Radiology. 1997;202(3):745-50.
14. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86(2):420-8.
15. Dombek MF, Orsini R, Mendicino RW, Saltrick K. Peroneus brevis tendon tears. Clin Podiatr Med Surg. 2001;18(3):409- 27.
16. Bencardino JT, Rosenberg ZS, Serrano LF. MR imaging features of diseases of the peroneal tendons. Magn Reson Imaging Clin N Am. 2001;9(3):493-505.
17. Slater HK. Acute peroneal tendon tears. Foot Ankle Clin.
2007;12(4):659-74.
18. Heckman DS, Reddy S, Pedowitz D, Wapner KL, Parekh SG.
Operative treatment for peroneal tendon disorders. J Bone Joint Surg Am. 2008;90(2):404-18.
19. Karlsson J, Wiger P. Longitudinal split of the peroneus brevis tendon and lateral ankle instability: treatment of concomitant lesions. J Athl Train. 2002;37(4):463-6.
20. Major NM, Helms CA, Fritz RC, Speer KP. The MR imaging appearance of longitudinal split tears of the peroneus brevis tendon. Foot Ankle Int. 2000;21(6):514-9.
21. Alanen J, Orava S, Heinonen OJ, Ikonen J, Kvist M. Peroneal tendon injuries: report of thirty-eight operated cases. Ann Chir Gynaecol. 2001;90(1):43-6.
22. Sobel M, Bohne WH, Markisz JA. Cadaver correlation of peroneal tendon changes with magnetic resonance imaging.
Foot Ankle. 1991;11(6):384-8.
23. Sobel M, DiCarlo EF, Bohne WH, Collins L. Longitudinal splitting of the peroneus brevis tendon: an anatomic and histologic study of cadaveric material. Foot Ankle.
1991;12(3):165-70.
24. Bonnin M, Tavernier T, Bouysset M. Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med. 1997;25(5):699-703.
25. Frey C, Bell J, Teresi L, Kerr R, Feder K. A comparison of MRI and clinical examination of acute lateral ankle sprains.
Foot Ankle Int. 1996;17(9):533-7.
26. Cardone BW, Erickson SJ, Den Hartog BD, Carrera GF. MRI of injury to the lateral collateral ligamentous complex of the ankle. J Comput Assist Tomogr. 1993;17(1):102-7.
27. Donley BG, Leyes M. Peroneus quartus muscle: a rare cause of chronic lateral ankle pain. Am J Sports Med.
2001;29(3):373-5.