Comparison of the Changes in the Range of Motion on the Knee Joint According to the Contraction Intensity During Evjenth-Hamberg Stretching in Healthy Subjects: A Cross-Sectional Pilot Study
11
0
0
전체 글
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
수치

관련 문서
The purpose of this study is to evaluate the effects of heat treatment on the load-deflection properties and transitional temperature range(TTR) of
The purpose of this study is to investigate changes in listening, reading achievement, and learning attitudes of Korean elementary students who enrolled in
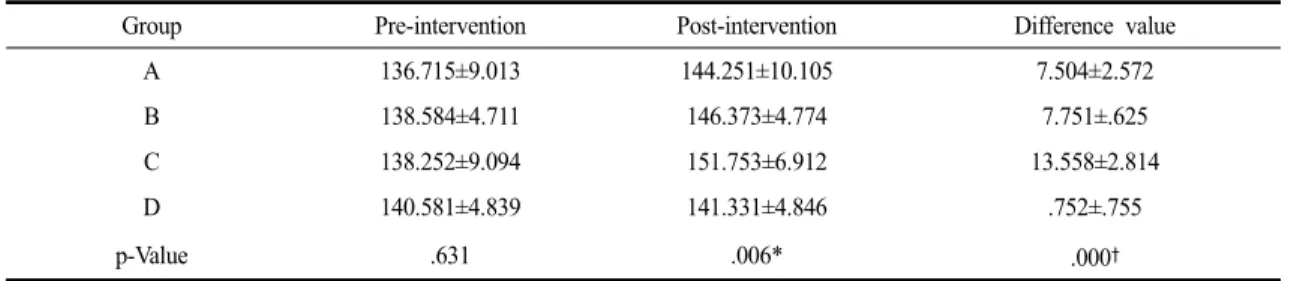
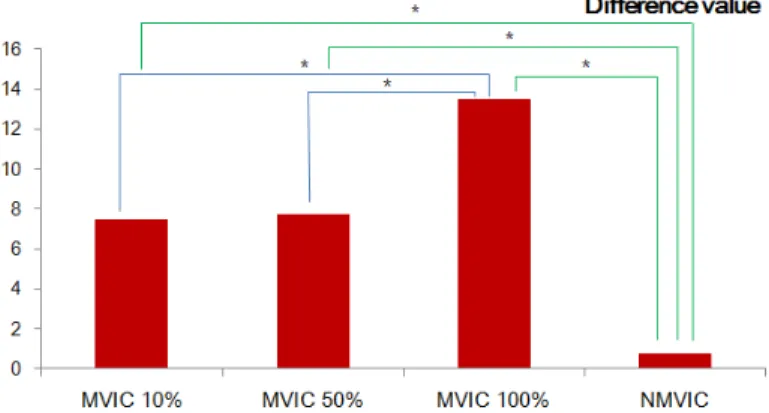
Injury is a burden on athletes, but the rehabilitation exercise of this study suggests that the improvement of knee muscle function and knee function
※ Screw home motion ⇒ 경골이 외측 회전 Open kinetic chain. http://moon.ouhsc.edu/dthompso/namics/screw3.gif.. Test
- quadriceps tendon 이 슬개골 하연에서 tibial tuberocity에 부착.
The index is calculated with the latest 5-year auction data of 400 selected Classic, Modern, and Contemporary Chinese painting artists from major auction houses..
The “Asset Allocation” portfolio assumes the following weights: 25% in the S&P 500, 10% in the Russell 2000, 15% in the MSCI EAFE, 5% in the MSCI EME, 25% in the
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
