The Impact of Vascular Access for In-Hospital Major Bleeding in Patients with Acute Coronary Syndrome at Moderate- to Very High-Bleeding Risk
The aim of our study was to determine the impact of vascular access on in-hospital major bleeding (IHMB) in acute coronary syndrome (ACS). We analyzed 995 patients with non-ST elevation myocardial infarction and unstable angina at the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) moderate- to very high-bleeding risk scores in trans-radial intervention (TRI) retrospective registry from 16 centers in Korea. A total of 402 patients received TRI and 593 patients did trans-femoral intervention (TFI). The primary end-point was IHMB as defined in the CRUSADE. There were no significant differences in in-hospital and 1-yr mortality rates between two groups. However, TRI had lower incidences of IHMB and blood transfusion than TFI (6.0% vs 9.4%, P = 0.048; 4.5% vs 9.4%, P = 0.003). The patients suffered from IHMB had higher incidences of in-hospital and 1-yr mortality than those free from IHMB (3.1% vs 15.0%, P < 0.001; 7.2% vs 30.0%, P < 0.001). TRI was an independent negative predictor of IHMB (odds ratio, 0.305; 95% confidence interval, 0.109-0.851; P = 0.003). In conclusions, IHMB is still significantly correlated with in-hospital and 1-yr mortality. Our study suggests that compared to TFI, TRI could reduce IHMB in patients with ACS at moderate- to very high-bleeding risk.
Key Words: Acute Coronary Syndrome; Radial Artery; Hemorrhage Keun-Ho Park,1 Myung Ho Jeong,1
Youngkeun Ahn,1 Sang Sik Jung,2 Moo Hyun Kim,3 Hyoung-Mo Yang,4 Junghan Yoon,5 Seung Woon Rha,6 Keum Soo Park,7 Kyoo Rok Han,8 Byung Ryul Cho,9 Kwang Soo Cha,10 Byung Ok Kim,11 Min Soo Hyon,12 Won-Yong Shin,13 Hyunmin Choe,14 Jang-Whan Bae,15 Hee Yeol Kim,16 and Trans-Radial Intervention Registry Investigators
1Chonnam National University Hospital, Gwangju;
2Gangneung Asan Hospital, Gangneung; 3Dong-A University Hospital, Busan; 4Ajou University Hospital, Suwon; 5Wonju Christian Hospital, Wonju;
6Korea University Guro Hospital, Seoul; 7Inha University Hospital, Incheon; 8Hallym University Kangdong Sacred Heart Hospital, Seoul; 9Kangwon National University Hospital, Chuncheon; 10Pusan National University Hospital, Busan; 11Inje University Sanggye Paik Hospital, Seoul; 12Soonchunhyang University Seoul Hospital, Seoul; 13Soonchunhyang University Cheonan Hospital, Cheonan; 14Inje University Ilsan Paik Hospital, Goyang; 15Chungbuk National University Hospital, Cheongju; 16The Catholic University of Korea Bucheon St. Mary’s Hospital, Bucheon, Korea
Received: 25 November 2012 Accepted: 11 July 2013 Address for Correspondence:
Myung Ho Jeong, MD
Principal Investigator of Korea Acute Myocardial Infarction Registry, Director of Heart Research Center Nominated by Korea Ministry of Health and Welfare, Chonnam National University Hospital, 671 Jaebongro, Dong-gu, Gwangju 501-757, Korea Tel: +82.62-220-6243, Fax: +82.62-228-7174 E-mail: [email protected]
http://dx.doi.org/10.3346/jkms.2013.28.9.1307 • J Korean Med Sci 2013; 28: 1307-1315 Cardiovascular Disorders
INTRODUCTON
Recurrent ischemic events after acute coronary syndrome (ACS) still remain common. Anti-thrombotic therapy with coronary revascularization and high rates of procedural success reduce the frequency of life-threatening ischemic events (1-3). Howev- er, with the greater use of anti-thrombotic medications and ear- ly revascularization, bleeding has become an increasingly im- portant problem. Recently, the European Society of Cardiology
guidelines are recommended to evaluate bleeding risk in non- ST elevation (NSTE)-ACS patients using established risk scores for bleeding such as the Can Rapid risk stratification of Unsta- ble angina patients Suppress ADverse outcomes with Early im- plementation of the ACC/AHA guidelines (CRUSADE) bleed- ing risk score (4, 5). This score is relatively accurate for estimat- ing bleeding risk by combining patient’s clinical variables. It is well known that bleeding complication is a strong independent predictor of early and late adverse clinical outcome in NSTE-
ACS patients. Therefore, all efforts should be made to reduce bleeding whenever possible, especially in patients with high risk of bleeding. However, whether vascular access affect in- hospital major bleeding (IHMB) in patients with ACS, especial- ly at high-bleeding risk, is not well determined. Therefore, the aim of our study is to evaluate the association between vascular access and IHMB in ACS patients with moderate- to very high- CRUSADE bleeding risk.
MATERIALS AND METHODS Study population
The trans-radial intervention (TRI) registry is a retrospective, observational, on-line registry data of all-comers who received the percutaneous coronary intervention (PCI) in 16 institutes of Korea from January through December 2009. The aim of regis- try is to evaluate the safety and efficacy of TRI compared with the trans-femoral intervention (TFI) in Korean patients. The vascular access for patient (trans-radial or trans-femoral) was determined by the clinical decision of interventional cardiolo- gist in each institutes. The data including baseline clinical, labo- ratory, angiographic characteristics, and 1-yr clinical outcomes were collected by a specialized study coordinator at each center using a standardized case report form. TRI or TFI was classified according to final vascular access without regard to operators’
intention before the index procedure.
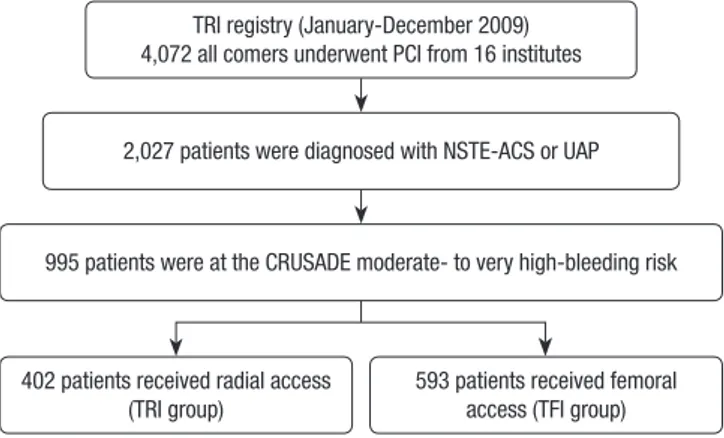
Total 4,072 patients were enrolled in TRI registry and 2,027 patients were diagnosed with non-ST elevation myocardial in- farction (NSTEMI) or unstable angina. The difference between NSTEMI and unstable angina was whether the cardiac markers were elevated or not. Of them, 995 patients with the CRUSADE moderate- to very high-bleeding risk scores (bleeding scores more than 31) were selected. Among them, 402 patients receiv- ed coronary intervention via trans-radial approach (TRI group) and 593 patients via trans-femoral approach (TFI group) (Fig. 1).
Procedure and post-intervention medications
The emergent or early invasive treatments were determined based on the ACS patient status according to the clinical deci- sion of operators in each institutes. The type of stent and use of peri-procedural glycoprotein IIb/IIIa inhibitors and anti-throm- botic medications were also determined based on the decision of operators and current guidelines. Percutaneous closure de- vices were unrestrictedly used to close arterial punctures. Anti- platelet agents were administered to all patients prior to the in- tervention, with aspirin 300 mg and clopidogrel 300-600 mg.
After the intervention, the patients received 100 mg of aspirin per day indefinitely and 75 mg of clopidogrel per day for at least one year. Other medical treatments were also used based on the standard treatment regimen for patients with ACS in a non- restrictive manner.
CRUSADE bleeding scores
For each patient, the CRUSADE risk score was calculated from the corresponding scores for the 8 prognostic variables it in- volves. The CRUSADE bleeding score considers baseline pa- tient characteristics (female sex, history of diabetes, prior vas- cular disease), admission clinical variables (heart rate, systolic blood pressure, signs of congestive heart failure), and admis- sion laboratory values (hematocrit, calculated creatinine clear- ance) (5).
Study outcomes
The primary end-point was the incidence of IHMB as defined in the CRUSADE study, such as intracranial bleeding, docu- mented retroperitoneal bleeding, a fall in hematocrit of ≥ 12%
(baseline to nadir), or any red blood cell transfusion in which baseline hematocrit was ≥ 28% or < 28% with clinically docu- mented bleeding. In patients who underwent revascularization surgery, only major bleeding events that occurred before the intervention were taken into account. Renal clearance of creati- nine was calculated with the Cockcroft-Gaut formula. The defi- nition of prior vascular disease was also that adopted by the CRUSADE registry (prior stroke and/or peripheral artery dis- ease). The secondary end-point was the incidence of the 1-yr major adverse cerebro-cardiovascular events (MACCE) defined as the composite of all-cause mortality, non-fatal MI, target le- sion revascularization (TLR), stent thrombosis, and cerebro- vascular accidents (CVA). TLR was defined as any ischemic driven percutaneous coronary revascularization performed on the treated lesion or vessel. Stent thrombosis was defined ac- cording to the Academic Research Consortium of Circulatory System Devices Panel Meeting, an advisory committee to the US Food and Drug Administration (FDA) in 2006.
Fig. 1. Flow chart of this study. TRI, trans-radial intervention; PCI, percutaneous coro- nary intervention; NSTE-ACS, non ST elevation acute coronary syndrome; UAP, un- stable angina pectoris; CRUSADE, Can Rapid risk stratification of Unstable angina pa- tients Suppress ADverse outcomes with Early implementation of the ACC/AHA guide- lines; TFI, trans-femoral intervention.
TRI registry (January-December 2009) 4,072 all comers underwent PCI from 16 institutes
2,027 patients were diagnosed with NSTE-ACS or UAP
995 patients were at the CRUSADE moderate- to very high-bleeding risk
402 patients received radial access
(TRI group) 593 patients received femoral access (TFI group)
Statistical analysis
Continuous variables were expressed as mean ± SD and cate- gorical ones were expressed as a frequency. An analysis of con- tinuous variables was performed using Student’s t-test and that of categorical ones was performed using chi-square test or Fis- her’s exact test. Multiple logistic regression analysis with the forward LR (likelihood ratio) was used to identify the indepen- dent predictors of IHMB. Only variables with a P value < 0.2 in the univariate analysis were included in the multivariate model.
All the statistical analyses were performed using SPSS 18.0 (Sta- tistical Package for Social Science, SPSS Inc, Chicago, IL, USA) for Windows. All statistical tests were two-tailed, and a value of P < 0.05 was considered statistically significant.
Ethics statement
The institutional review board of all participating centers ap- proved the study protocol. The approval number was 2011-127 of Chonnam National University Hospital. Informed consent was exempted by the board.
RESULTS
Patient baseline characteristics
Baseline demographic and clinical characteristics and labora- tory findings of the 2 groups are shown in Table 1 and Table 2.
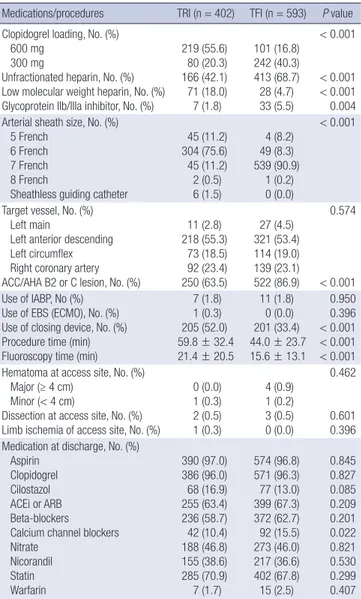
Current smoker, the past history of MI and heart failure were more common in TRI group. However, the past history of by- pass surgery and stable hemodynamic conditions at admission were more common and baseline hematocrit and creatinine clearance were lower in TFI group. The CRUSADE bleeding scores and risk groups were no significantly different between two groups (Table 3). Six hundred mg loading dose of clopido- grel and use of low molecular weight heparin were more com- mon in TRI group, however, use of unfractionated heparin or glycoprotein IIb/IIIa and ACC/AHA B2/C lesions were more common in TFI group. Six-French arterial sheath was common- ly used in TRI group, but seven-French sheath in TFI group. To- tal numbers of treated lesions were higher and procedure times and fluoroscopy times were significantly longer in TRI group, however, the vascular access site complications were similar Table 1. Baseline clinical characteristics in both two groups
Parameters TRI (n = 402) TFI (n = 593) P value
Age (yr) Age ≥ 65 yr (%) Female gender (%) Hypertension (%) Diabetes mellitus (%) History of smoking (%)
Non-smoker Ex-smoker Current smoker Dyslipidemia (%) Family history of CAD (%)
71.9 ± 8.3 337 (83.8) 265 (65.9) 298 (74.1) 200 (49.8) 281 (69.9) 49 (12.2) 72 (17.9) 102 (25.4) 9 (2.2)
70.9 ± 8.9 471 (79.4) 371 (62.6) 423 (71.3) 314 (53.0) 459 (77.4) 73 (12.3) 61 (10.3) 137 (23.1) 7 (1.2)
0.076 0.081 0.279 0.332 0.322 0.002
0.411 0.193 Previous myocardial infarction (%)
Previous PCI (%) Previous CABG (%) Previous heart failure (%) Previous CVA (%) Previous PAD (%)
38 (9.5) 31 (7.7) 1 (0.2) 17 (4.2) 36 (9.0) 6 (1.5)
33 (5.6) 30 (5.1) 14 (2.4) 7 (1.2) 58 (9.8) 14 (2.4)
0.019 0.087 0.007 0.003 0.662 0.338 LVEF (%)
LVEF < 50% (%)
Creatinine clearance (mL/min) Creatinine clearance < 60 mL/min (%)
58.5 ± 12.6 73 (26.6) 51.1 ± 18.1
296 (73.6)
58.2 ± 13.2 141 (25.4) 47.03 ± 21.1
473 (79.8)
0.767 0.702 0.001 0.023 Clinical diasgnosis (%)
Unstable angina
Non-ST elevation myocardial infarction 265 (65.9)
137 (34.1) 375 (63.2)
218 (36.8)
0.386
Cardiogenic shock at admission
Underwent CPR at admission 12 (3.0)
3 (0.7) 18 (3.0)
6 (1.0) 0.964
0.664 Systolic blood pressure at admission (mmHg)
Diastolic blood pressure at admission (mmHg) Heart rate at admission (bpm)
126.7 ± 21.4 75.4 ± 12.8 76.1 ± 15.8
130.8 ± 28.0 80.3 ± 15.8 78.9 ± 16.6
0.029
< 0.001 0.019 CRUSADE bleeding risk groups
Moderate bleeding risk (%) High bleeding risk (%) Very high bleeding risk (%) CRUSADE bleeding risk scores
202 (50.3) 117 (29.1) 83 (20.6) 43.0 ± 9.3
282 (47.5) 192 (32.4) 119 (20.1) 42.8 ± 9.2
0.532
0.675
TRI, trans-radial intervention; TFI, trans-femoral intervention; CAD, coronary artery disease; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; CVA, cerebrovascular accidents; PAD, peripheral artery disease; CPR, cardiopulmonary resuscitation; CRUSADE, the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines.
between two groups (Table 4).
Clinical outcomes
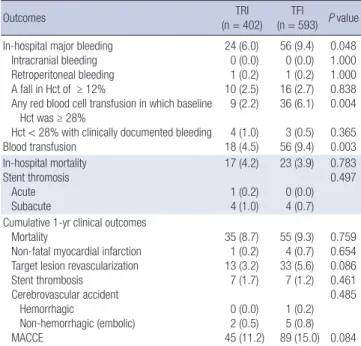
During 1-yr clinical follow-up, the incidence of in-hospital mor- tality and 1-yr MACCE were no significantly different between two groups (4.2% vs 3.9%, P = 0.783; 11.2% vs 14.8%, P = 0.097).
However, the incidence of IHMB and blood transfusion were significantly lower in the TRI group compared with TFI group (6.0% vs 9.4%, P = 0.048; 4.5% vs 9.4%, P = 0.003) (Table 5). The incidence of IHMB showed a consistent gradient of risk across the 3 risk categories, regardless of vascular access. The incidence of IHMB was no significantly different between two groups in patients with the CRUSADE moderate bleeding risk (3.0% vs 2.8%, P = 0.931). However, TRI group tended to have lower inci- dence of IHMB than TFI group in patients with the CRUSADE high- and very high bleeding risk group (4.3% vs 9.9%, P = 0.073;
15.7% vs 24.4%, P = 0.134) (Fig. 2). Accordingly, the significant lower incidence of IHMB in patients with CRUSADE high to very high bleeding risk group (n = 511) was observed in TRI
group than TFI group (9.0% vs 15.4%, P = 0.034). The eighty pa- tients (8.0%) suffered from IHMB. Retroperitoneal bleeding oc- curred in two patients of TFI group, hemoptysis in one patient of TFI group, and gastrointestinal bleeding in three patients of each group. They had higher incidences of in-hospital and 1-yr mortality than those free from IHMB (3.1% vs 15.0%; 7.2% vs 30.0%, P < 0.001 respectively) (Fig. 3, 4).
Multivariate and subgroup analyses
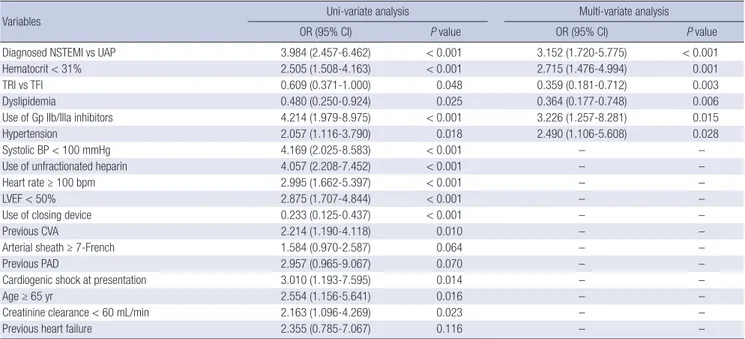
By multivariate logistic regression analysis, the independent predictors of IHMB were the diagnosis of NSTEMI (odds ratio [OR], 3.152; 95% confidence intervals [CI], 1.720-5.775), hema- tocrit < 31% at admission (OR, 2.715; 95% CI, 1.476-4.994), the use of glycoprotein IIb/IIIa inhibitors (OR, 3.226; 95% CI, 1.257 -8.281), and the history of hypertension (OR, 2.490; 95% CI, Table 2. Laboratory findings in both two groups
Items TRI (n = 402) TFI (n = 593) P value
Hematocrit (%) 37.4 ± 5.7 35.4 ± 5.8 < 0.001
Creatinine (mg/dL) 1.4 ± 4.4 1.8 ± 2.3 0.114
Glucose (mg/dL) 153.5 ± 100.1 171.1 ± 90.0 0.012
Total cholesterol (mg/dL) 176.4 ± 47.4 172.2 ± 45.8 0.174 LDL-cholesterol (mg/dL) 106.7 ± 37.5 104.32 ± 39.4 0.367 HDL-cholesterol (mg/dL) 42.5 ± 14.0 41.3 ± 12.0 0.176 Triglyceride (mg/dL) 143.6 ± 95.4 131.7 ± 85.5 0.059
CK-MB (ng/mL) 12.5 ± 63.0 11.5 ± 27.4 0.741
Peak CK-MB (ng/mL) 32.9 ± 107.7 36.2 ± 106.4 0.670
Troponin-I (ng/mL) 2.7 ± 7.9 7.6 ± 39.0 0.020
Peak troponin-I (ng/mL) 8.6 ± 17.8 13.1 ± 44.0 0.086
hs-CRP (mg/dL) 1.5 ± 3.7 1.6 ± 3.2 0.827
TRI, trans-radial intervention; TFI, trans-femoral intervention; LDL, low-density lipo- protein; HDL, high-density lipoprotein; CK-MB, creatine kinase-MB fraction; CRP, C- reactive protein; BP, blood pressure.
Table 3. CRUSADE bleeding scores in both groups
Scores TRI (n = 402) TFI (n = 593) P value
CRUSADE bleeding scores Baseline hematocrit Creatinine clearance Heart rate Sex
Sign of CHF at presentation Prior vascular disease Diabetes mellitus Systolic blood pressure
43.0 ± 9.3 3.1 ± 3.2 26.1 ± 6.3 1.8 ± 2.6 5.3 ± 3.8 3.3 ± 3.5 0.1 ± 0.3 3.0 ± 3.0 3.4 ± 2.7
42.8 ± 9.2 4.3 ± 3.4 27.5 ± 6.9 2.2 ± 2.9 5.0 ± 3.9 4.3 ± 3.4 0.1 ± 0.3 3.2 ± 3.0 3.4 ± 2.7
0.675
< 0.001 0.001 0.054 0.278 0.125 0.395 0.322 0.851 CRUSADE bleeding risk groups, No. (%)
Moderate (score 31-40) High (score 41-50) Very high (score > 50)
202 (50.3) 117 (29.1) 83 (20.6)
282 (47.5) 192 (32.4) 119 (20.1)
0.532
TRI, trans-radial intervention; TFI, trans-femoral intervention; CRUSADE, the Can Ra- pid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines; CHF, congestive heart failure.
Table 4. In-hospital medications and procedural characteristics in both groups Medications/procedures TRI (n = 402) TFI (n = 593) P value Clopidogrel loading, No. (%)
600 mg 300 mg
Unfractionated heparin, No. (%) Low molecular weight heparin, No. (%) Glycoprotein IIb/IIIa inhibitor, No. (%)
219 (55.6) 80 (20.3) 166 (42.1) 71 (18.0) 7 (1.8)
101 (16.8) 242 (40.3) 413 (68.7) 28 (4.7) 33 (5.5)
< 0.001
< 0.001
< 0.001 0.004 Arterial sheath size, No. (%)
5 French 6 French 7 French 8 French
Sheathless guiding catheter
45 (11.2) 304 (75.6) 45 (11.2) 2 (0.5) 6 (1.5)
4 (8.2) 49 (8.3) 539 (90.9)
1 (0.2) 0 (0.0)
< 0.001
Target vessel, No. (%) Left main
Left anterior descending Left circumflex Right coronary artery ACC/AHA B2 or C lesion, No. (%)
11 (2.8) 218 (55.3)
73 (18.5) 92 (23.4) 250 (63.5)
27 (4.5) 321 (53.4) 114 (19.0) 139 (23.1) 522 (86.9)
0.574
< 0.001 Use of IABP, No (%)
Use of EBS (ECMO), No. (%) Use of closing device, No. (%) Procedure time (min) Fluoroscopy time (min)
7 (1.8) 1 (0.3) 205 (52.0) 59.8 ± 32.4 21.4 ± 20.5
11 (1.8) 0 (0.0) 201 (33.4) 44.0 ± 23.7 15.6 ± 13.1
0.950 0.396
< 0.001
< 0.001
< 0.001 Hematoma at access site, No. (%)
Major (≥ 4 cm) Minor (< 4 cm)
Dissection at access site, No. (%) Limb ischemia of access site, No. (%)
0 (0.0) 1 (0.3) 2 (0.5) 1 (0.3)
4 (0.9) 1 (0.2) 3 (0.5) 0 (0.0)
0.462
0.601 0.396 Medication at discharge, No. (%)
Aspirin Clopidogrel Cilostazol ACEi or ARB Beta-blockers Calcium channel blockers Nitrate
Nicorandil Statin Warfarin
390 (97.0) 386 (96.0) 68 (16.9) 255 (63.4) 236 (58.7) 42 (10.4) 188 (46.8) 155 (38.6) 285 (70.9) 7 (1.7)
574 (96.8) 571 (96.3) 77 (13.0) 399 (67.3) 372 (62.7) 92 (15.5) 273 (46.0) 217 (36.6) 402 (67.8) 15 (2.5)
0.845 0.827 0.085 0.209 0.201 0.022 0.821 0.530 0.299 0.407 TRI, trans-radial intervention; TFI, trans-femoral intervention; ACC/AHA, American College of Cardiology/American Heart Association; IAPB, intra-aortic balloon pump;
EBS, emergency bypass system; ECMO, extracorporeal membrane oxygenation; ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
1.106-5.608). However, TRI group (OR, 0.359; 95% CI, 0.181- 0.712), the history of dyslipidemia (OR, 0.364; 95% CI, 0.177- 0.748) were the independent negative predictors of IHMB (Ta- ble 6).
Subgroup analyses showed that compared to TFI, TRI could significantly reduce the incidence of IHMB in male gender (OR, 0.129; 95% CI, 0.029-0.586; P = 0.008), in patients older than 65 yr (OR, 0.280; 95% CI, 0.133-0.587; P = 0.001), in patients with the history of hypertension (OR, 0.340; 95% CI, 0.158-0.731; P = 0.006), in patients with the history of diabetes (OR, 0.255; 95%
CI, 0.104-0.626; P = 0.003), in patients with creatinine clearance less than 60 mL/min (OR, 0.320; 95% CI, 0.149-0.689; P = 0.004), in patients with left ventricular ejection fraction less than 50%
(OR, 0.217; 95% CI, 0.075-0.626; P = 0.005), in patients with NS-
TEMI (OR, 0.267; 95% CI, 0.108-0.660; P = 0.004), and in patients with the high- to very high-bleeding risk (OR, 0.364; 95% CI, 0.171- 0.777; P = 0.009) (Fig. 5).
DISCUSSION
Our study was conducted to determine the impact of vascular access on IHMB and mortality in NSTE-ACS patients with mo- derate- to very high-bleeding risk. Although numerous studies have reported the association between vascular access and IHMB, previous studies did not focus precisely patients with high bleeding risk. Our study showed that regardless of vascular access, the incidence of bleeding was also higher among the CRUSADE highest risk groups in Korean patients and IHMB was still significantly correlated with in-hospital and 1-yr mor- tality. Our study suggests that compared to TFI, TRI could re- duce IHMB on ACS patients with the CRUSADE moderate- to Table 5. Incidences of in-hospital and 1-yr clinical outcomes in both groups
Outcomes TRI
(n = 402) TFI
(n = 593) P value In-hospital major bleeding
Intracranial bleeding Retroperitoneal bleeding A fall in Hct of ≥ 12%
Any red blood cell transfusion in which baseline Hct was ≥ 28%
Hct < 28% with clinically documented bleeding Blood transfusion
24 (6.0) 0 (0.0) 1 (0.2) 10 (2.5) 9 (2.2) 4 (1.0) 18 (4.5)
56 (9.4) 0 (0.0) 1 (0.2) 16 (2.7) 36 (6.1) 3 (0.5) 56 (9.4)
0.048 1.000 1.000 0.838 0.004 0.365 0.003 In-hospital mortality
Stent thromosis Acute Subacute
17 (4.2) 1 (0.2) 4 (1.0)
23 (3.9) 0 (0.0) 4 (0.7)
0.783 0.497
Cumulative 1-yr clinical outcomes Mortality
Non-fatal myocardial infarction Target lesion revascularization Stent thrombosis
Cerebrovascular accident Hemorrhagic
Non-hemorrhagic (embolic) MACCE
35 (8.7) 1 (0.2) 13 (3.2) 7 (1.7) 0 (0.0) 2 (0.5) 45 (11.2)
55 (9.3) 4 (0.7) 33 (5.6) 7 (1.2) 1 (0.2) 5 (0.8) 89 (15.0)
0.759 0.654 0.086 0.461 0.485
0.084 Hct, hematocrit; MACCE, major adverse cerebro-cardiovascular events.
Fig. 2. Incidences of in-hospital major bleeding according to the CRUSADE risk groups.
MB, major bleeding.
Incidence of in-hospital MB (%)
CRUSADE bleeding risk
Moderate High Very high
P = 0.931
3.0 2.8 4.3
9.9
15.7 24.4
P = 0.073 P = 0.134
TRI TFI
Fig. 3. In-hospital and 1-yr clinical outcomes in patients with and without in-hospital major bleeding. TLR, target lesion revascularization; ST, stent thrombosis; CVA, cere- brovascular accident; MACCE, major adverse cerebro-cardiovascular events.
Incidence (%)
1-yr clinical outcomes
In-hospital mortality
Mortality Non-fatal MI TLR ST CVA MACCE
P = 0.343 P = 0.084 P = 0.096 P = 0.130 P < 0.001 P < 0.001 P < 0.001
3.1 15.0
7.2 30.0
0.4 1.3 4.56.3
1.23.8 0.72.5
11.6 35.0
No IHMB IHMB
Fig. 4. Kaplan-Meier survival curves for 1-yr mortality according to occurrence of in- hospital major bleeding. IHMB, in-hospital major bleeding.
Probability of survival (%)
Survival days
100 200 300 400 Log rank
P < 0.001
IHMB No IHMB 100
90
80
70
60
50
40
very high-bleeding scores.
Patients with ACS are typically managed by initial medical stabilization followed by an early invasive approach, whereby cardiac catheterization is performed, usually within 24-48 hr of admission and the majority of patients subsequently undergo PCI. Use of anticoagulant and antiplatelet agents with early, in- vasive management reduces the risk for recurrent ischemic events, but may increase the risk for bleeding (6).
The incidence of bleeding complications varied widely among different trials. These discrepancies are primarily due to the dif- ferent definitions of major bleeding used and the different or new anti-thrombotic agent regimens used in the each trial. From analysis of 302,152 patients who performed PCI procedure at the 440 United States centers, bleeding complications occurred in 2.4% of patients (7). In the OASIS-5 study, the rate of MB at nine days was markedly lower with fondaparinux than with enoxaparin (2.2% vs 4.1%; hazard ratio, 0.52; P < 0.001) (8). In addition, a non-CABG-related MB occurred within 30 days of randomization in 520 (3.8%) of the 13,819 ACUITY patients and in 224 (6.2%) of the 3,602 HORIZONS-AMI patients (9, 10). The rate of bleeding complication seemed to be more prevalent in patients with ACS or AMI than those with stable angina. Our study represented that the rate of IHMB was 8.0%. The rate of bleeding was likely to be similar or somewhat higher compared with those of the other studies. It is explained that our study was not a well-controlled randomized trial but a real-world clinical practice and enrolled the NSTEMI or unstable angina patients with moderate to very high bleeding risk. The incidence of MB also showed a consistent gradient of risk across the 3 risk cate- gories in our study. Regardless of vascular access, bleeding inci- dence was higher among the CRUSADE highest risk groups.
The CRUSADE bleeding risk score groups were also well corre- lated with the incidence of IHMB in Korean NSTE-ACS patients.
It has been well known that MB was strongly associated with increased mortality. In addition, the severity of the bleeding complications was directly correlated with worse outcomes (11-14). A recent study from the CRUSADE registry reported that IHMB was a significant association with short and long- Table 6. Independent predictors of in-hospital major bleeding
Variables Uni-variate analysis Multi-variate analysis
OR (95% CI) P value OR (95% CI) P value
Diagnosed NSTEMI vs UAP 3.984 (2.457-6.462) < 0.001 3.152 (1.720-5.775) < 0.001
Hematocrit < 31% 2.505 (1.508-4.163) < 0.001 2.715 (1.476-4.994) 0.001
TRI vs TFI 0.609 (0.371-1.000) 0.048 0.359 (0.181-0.712) 0.003
Dyslipidemia 0.480 (0.250-0.924) 0.025 0.364 (0.177-0.748) 0.006
Use of Gp IIb/IIIa inhibitors 4.214 (1.979-8.975) < 0.001 3.226 (1.257-8.281) 0.015
Hypertension 2.057 (1.116-3.790) 0.018 2.490 (1.106-5.608) 0.028
Systolic BP < 100 mmHg 4.169 (2.025-8.583) < 0.001 – –
Use of unfractionated heparin 4.057 (2.208-7.452) < 0.001 – –
Heart rate ≥ 100 bpm 2.995 (1.662-5.397) < 0.001 – –
LVEF < 50% 2.875 (1.707-4.844) < 0.001 – –
Use of closing device 0.233 (0.125-0.437) < 0.001 – –
Previous CVA 2.214 (1.190-4.118) 0.010 – –
Arterial sheath ≥ 7-French 1.584 (0.970-2.587) 0.064 – –
Previous PAD 2.957 (0.965-9.067) 0.070 – –
Cardiogenic shock at presentation 3.010 (1.193-7.595) 0.014 – –
Age ≥ 65 yr 2.554 (1.156-5.641) 0.016 – –
Creatinine clearance < 60 mL/min 2.163 (1.096-4.269) 0.023 – –
Previous heart failure 2.355 (0.785-7.067) 0.116 – –
OR, odds ratio; CI, confidence interval; NSTEMI, non-ST elevation myocardial infarction; UAP, unstable angina pectoris; TRI, trans-radial intervention; TFI, trans-femoral interven- tion; Gp, glycoprotein; LV, left ventricular; CVA, cerebrovascular accidents; PAD, peripheral artery disease.
Fig. 5. Subgroup analyses for in-hospital major bleeding according to vascular ac- cess. OR, odds ratio; CI, confidence interval.
Male 0.129 0.029-0.586
Female 0.551 0.174-1.742
< 65 yr 0.010 0.000-51.927
≥ 65 yr 0.280 0.133-0.587
Hypertension (-) 0.655 0.043-9.906
Hypertension (+) 0.340 0.158-0.731
Diabetes mellitus (-) 1.028 0.211-5.019
Diabetes mellitus (+) 0.255 0.104-0.626
Left ventricular ejection fraction ≥ 50% 0.785 0.239-2.581 Left ventricular ejection fraction < 50% 0.217 0.075-0.626
Creatinine clearance ≥ 60 mL/min 0.622 0.027-14.088
Creatinine clearance < 60 mL/min 0.320 0.149-0.689
Unstable angina 0.987 0.210-4.626
Non-ST elevation myocardial infarction 0.267 0.108-0.660
Moderate-bleeding risk group 0.129 0.008-3.325
High- to very high-bleeding risk group 0.364 0.171-0.777
Overall 0.359 0.181-0.712
0 Favors TRI 1 Favors TFI
OR 95% CI
term mortality, particularly among PCI-treated patients with NSTEMI (15). In long-term data from HORIZON-AMI (Harmo- nizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction), the patients with IHMB after primary PCI have significantly increased 3-yr rates of morbidity and mortality (16). Many mechanisms that MB affects worse out- comes might involve greater comorbidities (advanced age, im- paired glomerular filtration rate, diabetes, etc.) in bleeding pa- tients, anemia results in an impairment of the oxygen delivery, hypotension, transfusion, inflammatory response and early cessation of antithrombotic therapies because of bleeding (17- 19). Our study showed that IHMB was also significantly associ- ated with in-hospital and 1-yr mortality.
A large number of trials have reported the predictors of MB including advanced age, female gender, baseline anemia, im- paired renal function, previous history of bleeding, STEMI, ad- vanced Killip class (III or IV) the degree of excess dose and the number of antithrombotic agents such as heparin plus glyco- protein IIb/IIIa inhibitor (17, 18, 20-24). In our study, initial di- agnosed as NSTEMI, hematocrit < 31%, use of glycoprotein IIb/IIIa inhibitor, and history of hypertension were also signifi- cant predictors of IHMB, however, TRI was a negative predictor.
Probably, it was associated that trans-radial access could re- duce the access site-related bleeding complications.
Bleeding complications after PCI are most commonly related to vascular access site and are associated with an increased risk of post-PCI morbidity and mortality (25-27). Pooled analysis of 23 randomized trials (n = 7,020) comparing the association be- tween radial versus femoral approaches for PCI presented that radial access reduced major bleeding and there was a tendency for reduction in ischemic events compared to femoral access (28). A recent study presents that TRI is associated with decreas- ed 2-yr mortality rates and a reduction in the need for vascular surgery and/or blood transfusion compared with TFI in patients undergoing angioplasty for AMI (29). Our study showed that TRI was also significantly related with reduction of IHMB and blood transfusion, however, resulted in similar rates of in-hos- pital mortality and 1-yr MACCE compared with TFI. Probably, our study showed relatively low incidences of major bleeding related to vascular access, and in addition, more than half of IHMB in TFI were any red blood cell transfusion in which base- line Hct ≥ 28%, which could be possible a clinically insignifi- cant state. Therefore, vascular access could have less influence on the mortality in our study. However, it was still uncertain that TRI could reduce short- and long-term mortality and large trials were necessary to discuss about this issue.
Our study showed that TRI was associated with a significant reduction in IHMB that was more prominent in patients with high-risk subgroups, such as more than 65 yr, history of hyper- tension and diabetes, low left ventricular ejection fraction, im- paired renal function, NSTEMI and high- to very high-bleeding
risk. Therefore, TRI was more safe and efficacious than TFI in patients with ischemic risk as well as those with bleeding risk.
Our study has some limitations. First, our study was a multi- center retrospective observational registry study that was many missing values. Therefore, the CRUSADE bleeding risk scores were relatively underestimated and the portion of moderate- to very high-bleeding risk group in our registry was relatively small- er than that in real-world clinical practice. We thought that our study was underpowered to assess the 1-yr clinical outcome.
However, in our study, it is clear that TRI had lower incidences of blood transfusion and IHMB than TFI in ACS patient with moderate- to very high bleeding risk. Second, our study was a retrospective post-hoc subgroup analysis of a TRI registry where the selection of vascular access was determined by the attend- ing interventional cardiologists and we did not apply the pro- pensity score matching analysis for elimination of the observed differences. Therefore, this might have introduced a significant bias in patient selection, even though it was partially compen- sated by multivariate analysis to control the baseline biases.
Third, in spite of no interaction between vascular access and use of glycoprotein IIb/IIIa inhibitors in logistic regression anal- ysis, TRI group was less frequent use of glycoprotein IIb/IIIa in- hibitors than TFI group.
In conclusions, our study represents that IHMB is still signifi- cantly correlated with in-hospital and 1-yr mortality and the CRUSADE bleeding risk score groups are also well correlated with the incidence of IHMB in Korean NSTE-ACS patients. Fur- thermore, we conclude that compared to TFI, TRI could reduce IHMB in ACS patients with the CRUSADE moderate- to very high-bleeding scores. However, much more trial remains to be done on the beneficial effect of TRI for clinical outcomes.
DISCLOSURE
The authors have no conflicts of interest to disclose.
REFERENCES
1. Ferguson JJ, Califf RM, Antman EM, Cohen M, Grines CL, Goodman S, Kereiakes DJ, Langer A, Mahaffey KW, Nessel CC, et al. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment eleva- tion acute coronary syndromes managed with an intended early inva- sive strategy: primary results of the SYNERGY randomized trial. JAMA 2004; 292: 45-54.
2. Stone GW, McLaurin BT, Cox DA, Bertrand ME, Lincoff AM, Moses JW, White HD, Pocock SJ, Ware JH, Feit F, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med 2006; 355: 2203-16.
3. Singh M, Rihal CS, Gersh BJ, Lennon RJ, Prasad A, Sorajja P, Gullerud RE, Holmes DR Jr. Twenty-five-year trends in in-hospital and long-term outcome after percutaneous coronary intervention: a single-institution experience. Circulation 2007; 115: 2835-41.
4. Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, Caso P,
Dudek D, Gielen S, Huber K, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coro- nary syndromes (ACS) in patients presenting without persistent ST-seg- ment elevation of the European Society of Cardiology (ESC). Eur Heart J 2011; 32: 2999-3054.
5. Subherwal S, Bach RG, Chen AY, Gage BF, Rao SV, Newby LK, Wang TY, Gibler WB, Ohman EM, Roe MT, et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleed- ing Score. Circulation 2009; 119: 1873-82.
6. Kim JS, Park SM, Kim BK, Ko YG, Choi D, Hong MK, Seong IW, Kim BO, Gwon HC, Hong BK, et al. Efficacy of clotinab in acute myocardial in- farction trial-ST elevation myocardial infarction (ECLAT-STEMI). Circ J 2012; 76: 405-13.
7. Mehta SK, Frutkin AD, Lindsey JB, House JA, Spertus JA, Rao SV, Ou FS, Roe MT, Peterson ED, Marso SP. Bleeding in patients undergoing percu- taneous coronary intervention: the development of a clinical risk algo- rithm from the National Cardiovascular Data Registry. Circ Cardiovasc Interv 2009; 2: 222-9.
8. Yusuf S, Mehta SR, Chrolavicius S, Afzal R, Pogue J, Granger CB, Budaj A, Peters RJ, Bassand JP, Wallentin L, et al. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med 2006; 354:
1464-76.
9. Stone GW, White HD, Ohman EM, Bertrand ME, Lincoff AM, McLau- rin BT, Cox DA, Pocock SJ, Ware JH, Feit F, et al. Bivalirudin in patients with acute coronary syndromes undergoing percutaneous coronary in- tervention: a subgroup analysis from the Acute Catheterization and Ur- gent Intervention Triage strategy (ACUITY) trial. Lancet 2007; 369: 907- 19.
10. Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, Kornowski R, Hartmann F, Gersh BJ, Pocock SJ, et al. Bivalirudin dur- ing primary PCI in acute myocardial infarction. N Engl J Med 2008; 358:
2218-30.
11. Mehran R, Pocock SJ, Nikolsky E, Clayton T, Dangas GD, Kirtane AJ, Parise H, Fahy M, Manoukian SV, Feit F, et al. A risk score to predict bleeding in patients with acute coronary syndromes. J Am Coll Cardiol 2010; 55:
2556-66.
12. Eikelboom JW, Mehta SR, Anand SS, Xie C, Fox KA, Yusuf S. Adverse impact of bleeding on prognosis in patients with acute coronary syn- dromes. Circulation 2006; 114: 774-82.
13. Rao SV, O’Grady K, Pieper KS, Granger CB, Newby LK, Van de Werf F, Mahaffey KW, Califf RM, Harrington RA. Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes. Am J Cardiol 2005; 96: 1200-6.
14. Ndrepepa G, Berger PB, Mehilli J, Seyfarth M, Neumann FJ, Schömig A, Kastrati A. Periprocedural bleeding and 1-year outcome after percutane- ous coronary interventions: appropriateness of including bleeding as a component of a quadruple end point. J Am Coll Cardiol 2008; 51: 690-7.
15. Lopes RD, Subherwal S, Holmes DN, Thomas L, Wang TY, Rao SV, Mag- nus Ohman E, Roe MT, Peterson ED, Alexander KP. The association of in-hospital major bleeding with short-, intermediate-, and long-term mortality among older patients with non-ST-segment elevation myocar- dial infarction. Eur Heart J 2012; 33: 2044-53.
16. Suh JW, Mehran R, Claessen BE, Xu K, Baber U, Dangas G, Parise H, Lansky AJ, Witzenbichler B, Grines CL, et al. Impact of in-hospital ma- jor bleeding on late clinical outcomes after primary percutaneous coro- nary intervention in acute myocardial infarction the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) trial. J Am Coll Cardiol 2011; 58: 1750-6.
17. Spencer FA, Moscucci M, Granger CB, Gore JM, Goldberg RJ, Steg PG, Goodman SG, Budaj A, FitzGerald G, Fox KA. Does comorbidity ac- count for the excess mortality in patients with major bleeding in acute myocardial infarction? Circulation 2007; 116: 2793-801.
18. Manoukian SV, Feit F, Mehran R, Voeltz MD, Ebrahimi R, Hamon M, Dangas GD, Lincoff AM, White HD, Moses JW, et al. Impact of major bleeding on 30-day mortality and clinical outcomes in patients with acute coronary syndromes: an analysis from the ACUITY trial. J Am Coll Car- diol 2007; 49: 1362-8.
19. Sabatine MS, Morrow DA, Giugliano RP, Burton PB, Murphy SA, Mc- Cabe CH, Gibson CM, Braunwald E. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation 2005;
111: 2042-9.
20. Moscucci M, Fox KA, Cannon CP, Klein W, López-Sendón J, Montale- scot G, White K, Goldberg RJ. Predictors of major bleeding in acute coro- nary syndromes: the Global Registry of Acute Coronary Events (GRACE).
Eur Heart J 2003; 24: 1815-23.
21. Yan AT, Yan RT, Huynh T, DeYoung P, Weeks A, Fitchett DH, Langer A, Goodman SG; INTERACT Investigators. Bleeding and outcome in acute coronary syndrome: insights from continuous electrocardiogram moni- toring in the Integrilin and Enoxaparin Randomized Assessment of Acute Coronary Syndrome Treatment (INTERACT) trial. Am Heart J 2008; 156:
769-75.
22. Lincoff AM, Bittl JA, Harrington RA, Feit F, Kleiman NS, Jackman JD, Sarembock IJ, Cohen DJ, Spriggs D, Ebrahimi R, et al. Bivalirudin and provisional glycoprotein IIb/IIIa blockade compared with heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary intervention: REPLACE-2 randomized trial. JAMA 2003; 289: 853-63.
23. Alexander KP, Chen AY, Roe MT, Newby LK, Gibson CM, Allen-LaPointe NM, Pollack C, Gibler WB, Ohman EM, Peterson ED. Excess dosing of antiplatelet and antithrombin agents in the treatment of non-ST-seg- ment elevation acute coronary syndromes. JAMA 2005; 294: 3108-16.
24. Pocock SJ, Mehran R, Clayton TC, Nikolsky E, Parise H, Fahy M, Lansky AJ, Bertrand ME, Lincoff AM, Moses JW, et al. Prognostic modeling of individual patient risk and mortality impact of ischemic and hemor- rhagic complications: assessment from the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circulation 2010; 121: 43-51.
25. Doyle BJ, Rihal CS, Gastineau DA, Holmes DR Jr. Bleeding, blood trans- fusion, and increased mortality after percutaneous coronary interven- tion: implications for contemporary practice. J Am Coll Cardiol 2009; 53:
2019-27.
26. Rao SV, Eikelboom JA, Granger CB, Harrington RA, Califf RM, Bassand JP. Bleeding and blood transfusion issues in patients with non-ST-seg- ment elevation acute coronary syndromes. Eur Heart J 2007; 28: 1193- 204.
27. Sciahbasi A, Pristipino C, Ambrosio G, Sperduti I, Scabbia EV, Greco C, Ricci R, Ferraiolo G, Di Clemente D, Giombolini C, et al. Arterial access- site-related outcomes of patients undergoing invasive coronary proce- dures for acute coronary syndromes (from the ComPaRison of Early In-
vasive and Conservative Treatment in Patients With Non-ST-ElevatiOn Acute Coronary Syndromes [PRESTO-ACS] Vascular Substudy). Am J Cardiol 2009; 103: 796-800.
28. Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on ma- jor bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J 2009; 157: 132-40.
29. Valgimigli M, Saia F, Guastaroba P, Menozzi A, Magnavacchi P, Santar- elli A, Passerini F, Sangiorgio P, Manari A, Tarantino F, et al. Transradial versus transfemoral intervention for acute myocardial infarction: a pro- pensity score-adjusted and -matched analysis from the REAL (REgistro regionale AngiopLastiche dell’Emilia-Romagna) multicenter registry.
JACC Cardiovasc Interv 2012; 5: 23-35.