대한외과학회지:제 67 권 제 6 호
□ 증 례 □ Vol. 67, No. 6, December, 2004
500
서 론
1869년 Balfour와 Stewart가 복수와 비장종대의 증상을 나 타냈던 간문맥 혈전증을 처음 기술한 이후로 증상과 징후 의 비특이성과 최근에 생긴 혈전의 경우 일반 초음파만으 로는 메아리발생(echogenicity)이 매우 낮고 정상 혈액 흐름 과 구별하기 어렵기 때문에 임상 진단에 어려움이 있 다.(1-3) 또한, 진단이 늦어질 경우 심각한 장기간 합병증을 유발하므로 빠른 진단과 적절한 치료를 요한다. 간문맥 혈 전증에 대한 숙지는 이러한 가능성을 생각하게 함으로써 진단율을 높이고 합병증을 줄일 수 있다.
저자들은 담도염을 동반한 담낭 및 담도 결석 수술 후에 생긴 간문맥 및 상장간막 혈전증이 약물 투여로 호전된 경 험이 있어 문헌 고찰과 함께 보고하는 바이다.
증 례
84세 남자 환자는 내원 2일 전부터 있어온 간헐적인 우상 복부 동통 및 오한을 주소로 내원하였다. 특정 질병 및 약물 을 복용한 과거력은 없었다. 내원 당시 활력 징후는 정상이 었으며 신체 검사에서 공막에 황달소견과 우상복부 압통 외 이상 소견은 보이지 않았으며 혈액 검사에서 백혈구수 는 9,900/mm3, 호산구 84.2%, 혈소판수 92,000/mm3, ESR 140 mm/hr 이상, PT 18.9 sec, APTT 57.5 sec, AST 144 IU/dl, ALT 47 IU/dl, 총 빌리루빈 1.95 mg/dl, 소변검사에서 혈액 +++, 빌리루빈 +, 우로빌리노겐 ++, 단백 +소견을 보 였다. 내원 당시 시행한 복부 전산화단층촬영에서 담낭벽 의 미만 성 비후와 1 cm 크기의 담낭 결석 및 경미한 간내 담관의 확장 소견 보였으며 좌측 신장에 3 cm 크기의 낭종 이 보였었다. 수술 소견에서 담낭은 커져 있었으며 담낭벽 의 비후 소견이 있어 담낭절제술을 시행하였다. 담낭내에 는 1 cm 크기의 색소 결석이 있었다. 총담관은 정상범위였 으나 수술 전 황달 소견이 있어 시행한 담관조영술을 위한 담낭관 삽관술시 농의 배출이 있었고 총담관 결석이 의심 되는 방사선 소견 있어 담도절개술(choledochotomy)을 실 시, 0.5 cm의 색소 결석을 제거하였다. 수술 후 10일째 시행 한 T관 담관조영술은 정상소견을 보여 11일째 T관을 제거
Portal Vein and Superior Mesenteric Vein Thrombosis following Cholecystectomy and Choledochostomy
In Kyu Lee, M.D., In Young Seo, M.D., Hae Myung Jeun, M.D., Suk Kyun Chang, M.D. and Sung Eon Yoon, M.D.1 Acute thrombosis of the portal and superior mesenteric vein (SMV) due to inflammation of abdominal organs is a rare condition, but delayed diagnosis causes severe problems and serious long term complications. Therefore the early diagnosis and adequate management of the underlying disease and thrombus is very important. Here a case of an 84-year-old man with portal vein and SMV thrombosis on Doppler ultrasonography and computed tomography (CT) after cholecystectomy and choledochostomy by the 10th day is reported. The patient's condition improved without compli- cation after the treatments with an anticoagulant regimen and antimicrobials. In the follow up, there was no thrombus on the CT or sign of a recurrent disease. (J Korean Surg Soc 2004;67:500-502)
Key Words: Portal vein thrombosis, Superior mesenteric vein thrombosis, Cholangitis, Anticoagulant
중심 단어: 문맥 혈전, 상장간막 정맥 혈전, 담도염, 항 응고제
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, College of Medicine, The Catholic University of Korea, 1Department of Radiology, University of Ulsan College of Medicine, Seoul Asan Medical Center, Seoul, Korea
책임저자:장석균, 서울특별시 영등포구 여의도동 62 ꂕ150-713, 가톨릭대학교 의과대학 외과학교실 Tel: 02-3779-1175, Fax: 02-786-0802
E-mail: [email protected]
접수일:2004년 5월 29일, 게재승인일:2004년 8월 9일
담낭 및 담관 결석 수술 후 생긴 간문맥 및 상장간막 정맥 혈전증
가톨릭대학교 의과대학 외과학교실, 1울산대학교 의과대학 서울아산병원 진단방사선과학교실
이인규․서인영․전해명․장석균․윤성언1
이인규 외:딤낭 및 담관 결석 수술 후 생긴 간문맥 및 상장간막 정맥 혈전증 501 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
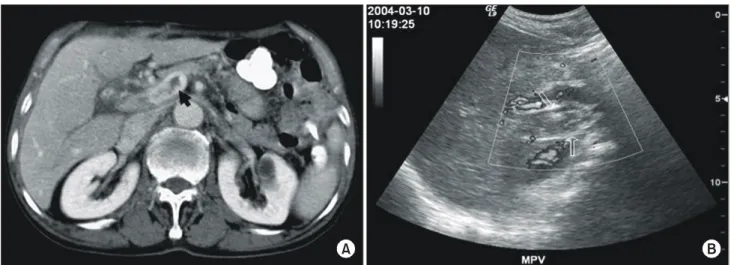
501 하였다. 수술 후 12일째 상복부 불쾌감 및 압통 소견 있으며 38.5oC의 열이 있어 혈액 검사를 시행하였으나 이상 소견은 없었다. 담즙 누출이 의심되어 시행한 초음파에서 우측 간 문맥에 혈전 의심 소견 있어 도플러 초음파 및 복부 전산화 단층촬영을 시행하였다. 검사 소견에서 간문맥, 우측 간문 맥과 근위부 상장간막정맥에 불완전 폐쇄성 혈전증 소견이 보였으며 말단 간내담도 확장소견이 보였다(Fig. 1). 혈액배 양에서 자라는 세균은 없었으며 폐흡충 및 간흡층 피부 검 사는 음성 소견이었다. 환자는 이후 저분자 헤파린을 7일간 투여하였고 씨푸로플록사신을 정맥 주사하였다. 와파린은 헤파린과 3일간 병합투여 후 계속 투여하였다. 열 및 동통 이 없어져 간문맥 혈전 발생 2주 후 퇴원하였다. 발생 5주 후 외래에서 시행한 복부 전산화단층촬영에서 혈전 소견은 없었고(Fig. 2), 2개월 예정으로 항응고제를 복용하며 외래
로 통원치료 중이다.
고 찰
급성 간문맥 혈전증은 임상증상의 비특이성 때문에 진단 에 어려움이 있으나 대부분은 식욕부진, 상복부 및 우상복 부 복통, 구토 등 장 울혈로 인한 다양한 위장 증상으로 나 타난다.(4) 혈전증을 유발하는 병인론을 보면 첫 번째로 과 다응고(hypercoagulability)를 유발하는 골수증식질환(myelo- proliferative disease)이나 antithrombin, protein C, protein S와 같은 coagulation inhibitor의 결핍을 가지는 유전적 질환, 또 한 이러한 물질의 생성을 감소시키는 간부전이나 손실을 증가시키는 콩팥증후군(nephrotic syndrome)에서 이차적으 로 야기되며 Factor V Leiden 돌연변이가 활성화된 Protein C에 대해 저항성을 나타내어 이러한 coagulation cascade의 이상을 일으킬 수 있으며, 피임약도 이러한 문제를 야기할 수 있다. 두 번째로 간문맥의 유량(flow)의 감소를 유발하는 질환으로 간경화나 간담도 악성종양을 포함하는 악성종양 과 Budd-Chiari syndrome, 간의 nodular regenerative hyper- plasia, 간농양, 문맥주위 섬유화에서 간문맥혈전증이 나타 날 수 있으며, 이러한 간문맥 혈전증이 원인이 된 간 질환을 진행시킬 수 있다. 세 번째로 복강내 감염과 염증성 질환에 서 유발되는데 게실염, 췌장염, 염증성 장질환, 담관염, 충 수돌기염, 간 농양 등이 있다. 특히 복강내 수술과 패혈증, 파종혈관내응고(DIC)의 경우 위험도가 높은 것으로 알려져 있다.(5) Plemmons 등(6)은 간문맥에 생긴 패혈 혈전정맥염 (septic thrombophlebitis)인 문맥염(pylephlebitis)의 경우 19명 의 모든 환자에서 열이 있었고 74%는 복부 통증, 21%는 패 혈증으로 증상이 나타났었다. 그중 게실염이 가장 많은 원 인이었고 사망률은 32%로 보고하였다. Cosenza 등(7)은 반 Fig. 1. Abdominal computed tomographic scan (A) and Doppler songraphy (B) on postoperative 10th day showed incomplete obstructive
thrombosis in main portal vein (arrow).
A B
Fig. 2. Follow up computed tomographic scan showed no evidence of the portal vein thrombosis by the 5th week.
502 대한외과학회지:제 67 권 제 6 호 2004
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 복적인 화농 담관염을 가진 16명의 환자를 대상으로 한 검
사에서 부분적 간문맥혈전증이 33%에서 관찰되었으며 그 기전으로 간문맥 분지 주변의 담관에 염증으로 인한 광범 위한 관주위염증(periductal inflammation)으로 간문맥에 혈 전성 정맥염이 생긴다고 설명을 하고 있다. 그 외 TIPS (transjugular intrahepatic portosystemic shunt)와 같은 기계적 시술과 간담도수술, 비장절제술, 간이식술등과 같은 수술 후 생기는 것으로 보고하고 있다.(8)
본 증례 환자의 경우는 결석을 동반한 담관염과 담낭염 으로 인한 복강내 감염증과 이로 인한 간 기능 저하가 과다 응고를 유발하였으며, 수술로 인한 위험도 증가가 이러한 급성 간문맥 및 상장간막 혈전증을 유발한 것으로 생각된 다.
간문맥 혈전증에서의 치료는 선택적 문맥 정맥조영술을 통한 혈전용해제의 투여나 수술적 혈전제거술, 정맥내 헤 파린 투여후 경구 항응고제를 투여하여 치료하는 것으로 되어있다.(4) 간문맥의 패혈 혈전증의 경우는 혈액배양검사 에서 Escherichia coli, Bacteroides fragilis, Peptostreptococcus prevotii, Eubacterium lentum이 배양된 것으로 보고하고 있고 항생제는 농양이 없다면 4주 이상 사용하였으며 간내농양 이 발생시에는 6주 이상의 치료가 필요한 것으로 보고하고 있다.(6,9,10) 항응고제 사용에 대해 저자에 따라 불필요하 다는 의견부터 필요하다는 의견까지 다양한 의견이 있으 나, 문맥염 환자의 생존에는 중요한 역할을 하지는 않지만 간내 패혈색전증을 감소시키는데 이점이 있을 것이며 적절 한 시기에 광범위 항생제를 투여하는 것이 가장 중요한 점 이라고 보고하고 있다.(11,12,6) 본 증례 환자의 경우 수술을 통해 패혈 병터를 제거한 상태이며 혈액배양검사에서 배양 되는 세균이 없었으나 갑작스런 고열을 고려하여 2세대 세 팔로스포린에서 씨푸로플록사신으로 변경 정맥투여하였으 며 퇴원 후에는 발생 후 5주까지 경구 투여하였다. 또한 급 성혈전증이며 상장간막정맥부터 우 간문맥까지 증가되는 소견임을 고려하여 저분자 헤파린을 일주일간 투여하였고 와파린을 병합 투약 후 5주간 단독으로 투약하여 혈전이 완전히 제거된 상태로, 총 2달간 투약 예정이다.
REFERENCES
1) Balfour GW, Steward TG. Case of enlarged spleen complicated with ascites. both depending upon varicose dilatation and thrombosis of the portal vein. Edinburgh Med J 1869;14:
589-98.
2) Miller VE, Berland LL. Pulsed doppler duplex sonography and CT of portal vein thrombosis. Am J Roentgenol 1985;145:
73-6.
3) Albertyn LE. Case report: acute portal vein thrombosis. Clin Radiol 1987;38:645-8.
4) Sheen CL, Lamparelli H, Milne A, Green I, Ramage JK.
Clinical features, diagnosis and outcome of acute portal vein thrombosis. Q J Med 2000;93:531-4.
5) Janssen HLA. Changing Perspectives in Portal Vein Throm- bosis. Scand J Gastroenterol 2000;35:69-73.
6) Plemmons RM, Dooley DP, Longfield RN. Septic throm- bophlebitis of the portal vein(pylephlebitis): diagnosis and management in the modern era. Clin Infect Dis. 1995;
21:1114-20.
7) Cosenza CA, Durazo F, Stain SC, Jabbour N, Selby RR.
Current management of recurrent pyogenic cholangitis. Am Surg 1999;65:939-43.
8) Terada T, Nakanuma Y, Yonejima M, Yokoyama H, Koike N. Portal, mesenteric and splenic venous thrombosis after endoscopic injection sclerotherapy. J Clin Gastroenterol 1990;
12:238-9.
9) Takahashi H, Sakata I, Adachi Y. Treatment of portal vein septic thrombosis by infusion of antibiotics and an antifungal agent into portal vein and superior mesenteric artery: a case report. Hepatogastroenterology 2003;50:1133-5.
10) Barnes PF, De Cock KM, Reynolds TN, Ralls PW. A com- parison of amebic and pyogenic abscess of the liver. Medicine (Baltimore) 1987;66:472-83.
11) Maki DG. Septic thrombophlebitis (part 2). Hospital Medicine 1977;january:6-29.
12) Shaw PJ, Saunders AJ, Drake KP. Case report: ultrasono- graphic demonstration of portal vein thrombosis in the acute abdomen. Clin Radiol 1986;37:101-2.