Received: 19 May, 2012 Revised: 28 July, 2012 Accepted: 15 August, 2012 Corresponding author: Won Jae Choi
Department of Physical Therapy, Uijeongbu Healings Hospital, 19 Cheongsa-ro 48beon-gil, Uijeongbu 480-865, Republic of Korea Tel: 82-31-853-9222 Fax: 82-31-853-9221 E-mail: [email protected]
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licens es/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2012 Korean Academy of Physical Therapy Rehabilitation Science
pISSN 2287-7576 Phys Ther Rehabil Sci
eISSN 2287-7584 2012, 1 (1), 1-5
www.jptrs.org
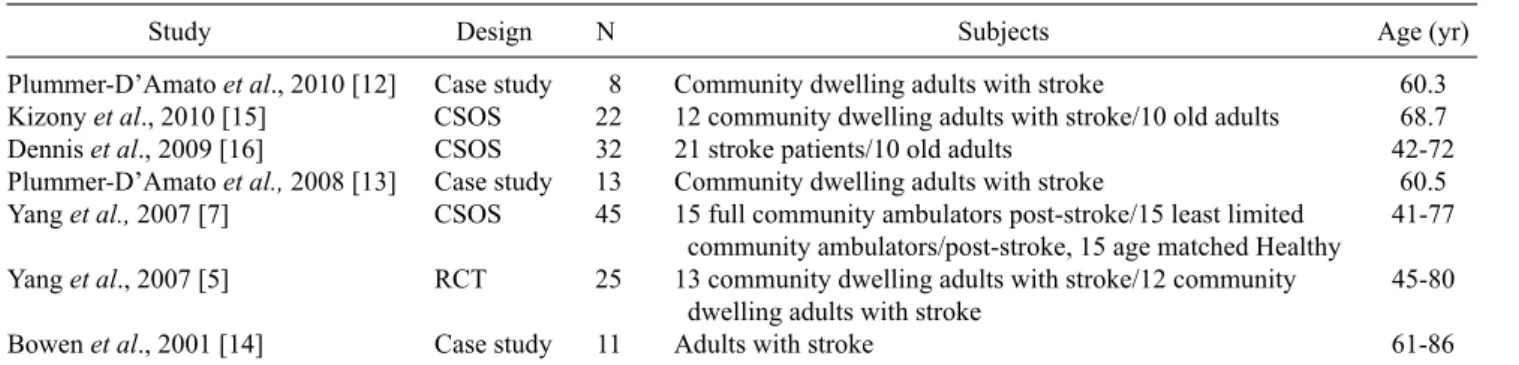
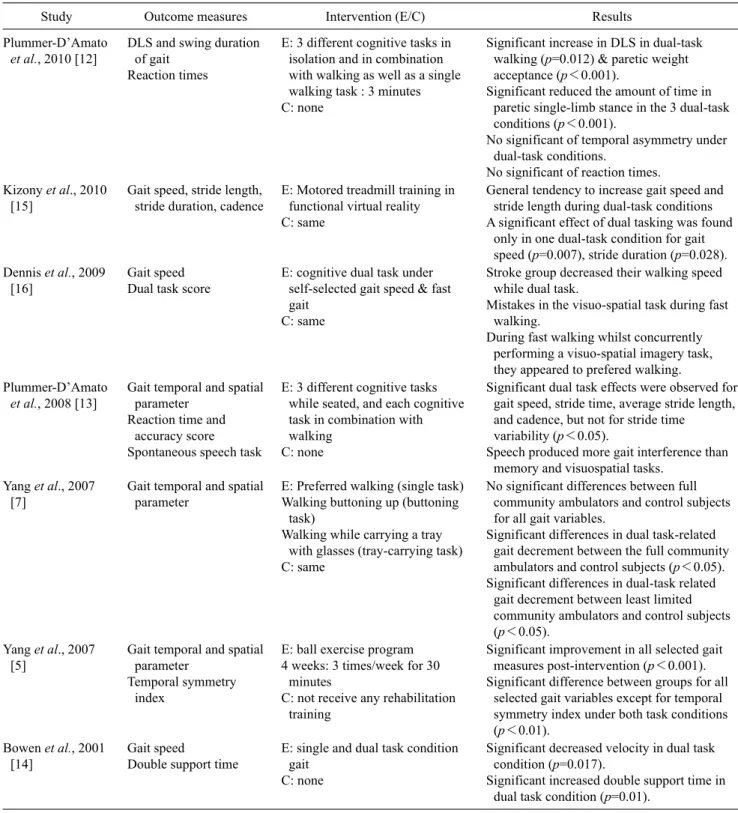
The effects of dual-task training on ambulatory abilities of stroke patients: Review of the latest trend
Gyu Chang Lee a , Won Jae Choi b
a
Department of Physical Therapy, College of Natural Sciences, Kyungnam University, Changwon, Republic of Korea
b