Vol.20 No.1. 28-35. June, 2003.
1)
책임저자:김세동, 대구시 남구 대명동 317-1, 영남대학교병원 정형외과 TEL.(053) 620-3642 FAX.(053) 628-4020 E-mail: [email protected]
Running title:대퇴골두 골단분리증 환자의 골단판 재형성
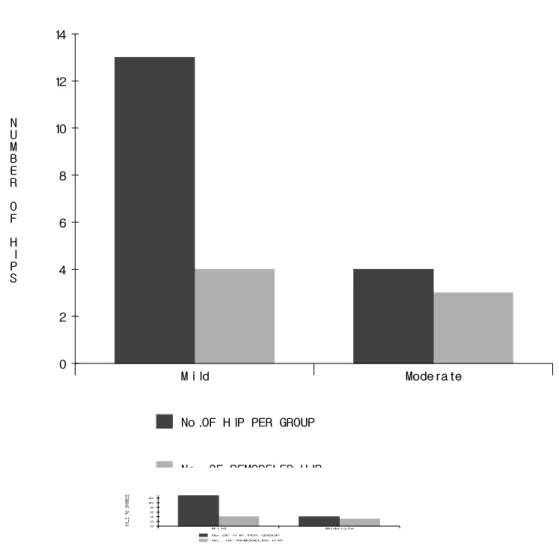
대퇴골두골단분리증 환자 중 금속내고정술을 시행받은 환자에서의 골단판의 재형성
영남대학교 의과대학 정형외과학교실
전체 글
Vol.20 No.1. 28-35. June, 2003.
1)
책임저자:김세동, 대구시 남구 대명동 317-1, 영남대학교병원 정형외과 TEL.(053) 620-3642 FAX.(053) 628-4020 E-mail: [email protected]
Running title:대퇴골두 골단분리증 환자의 골단판 재형성
영남대학교 의과대학 정형외과학교실
수치



관련 문서
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
In this way, the origin of capital gain tax which is to fulfill the security of internal revenue and property holdback functions has a lot of natural
measured in clockwise from the north to the vertical plane containing the given line - Plunge: An acute angle measured in a vertical. plane between the given line and the
The basic goals of the capital system is to maintain the capital of corporations strictly in order to protect creditors of the corporation. Such capital
The switching of gecko toes between attachment and detach- ment, utilization of the nanotape-like functions of the spatula pads, the orienting actions of the seta shaft,
The clinical outcome and complication for treating proximal femoral shaft fracture were compared and analyzed through the group treated with closed
à An element of material near the center of the shaft has a low stress and a small moment arm and thus contributes less to the twisting moment than an
Therefore, in the linear elasticity theory, the shear stress also varies linearly from the axis of a circular shaft.... FIGURE 5.3 Distribution

