대한외과학회지:제 70 권 제 2 호
□ 원 저 □ Vol. 70, No. 2, February, 2006
98
서 론
진행성 위암 중 고유근층까지만 침윤한 위암을 고유근층 위암이라 한다.(1) 고유근층 위암은 전체 위암의 10∼20%
로 보고되고 있는데(2,3) 5년 생존율이 70∼85%로 오히려 조기위암에 가깝다.(4) 따라서 고유근층 위암은 진행성위암 에 속하지만 조기위암과 진행성위암의 중간병기로 여겨진 다. 그리고 그 생물학적 특성이 진행성위암과 다르다고 생 각된다.(2,5) 그럼에도 불구하고 고유근층 위암의 재발의 특 성이나 예후 인자에 대한 연구는 많은 보고가 없는 상태이 다.
이에 저자들은 고유근층 위암의 임상병리학적 인자의 특 성과 재발의 위험인자 및 재발의 양상을 분석하여 향후 고 유근층 위암환자의 보다 적절한 치료 방침을 결정하는데 있어서 도움이 되고자 하였다.
방 법
1992년 2월부터 2000년 12월까지 고려대학교 의과대학 외과학교실에서 위암으로 진단 받고 근치적 절제술을 시행 받은 1,427예의 환자 중 수술 후 조직학적 검사상 고유근층 까지만 침범된 164예 중 수술로 인한 사망환자와 추적 조사 에서 누락된 8예를 제외한 156예를 대상으로 재발한 경우 (31예)와 재발하지 않은 경우(125예)로 나누어 나이, 성별, 종양의 위치, 종양의 크기, 수술의 종류, 림프절 전이 정도, 육안형, 조직학적 분화도 등 임상 병리학적 인자를 비교 분 석하였다. 대상 환자들은 모두 D2 이상의 광범위 림프절 곽 청술을 시행 받았다. 수술 후 평균 추적기간은 48.1개월(범 위: 5∼114개월)이었고, 추적률은 95%였다.
정기적인 추적관리는 이학적 검사, 임상병리학적 검사,
고유근층 위암의 근치적 절제술 후 재발에 관한 위험인자
고려대학교 의과대학 외과학교실
김호일․김종석․김승주․목영재․박성수
Risk Factors of the Recurrence after a Curative Resection of Gastric Carcinoma Invading the Muscularis Propria
Ho-ll Kim, M.D., Chong-Suk Kim, M.D., Seung-Joo Kim,
M.D., Young-Jae Mok, M.D. and Sung-Soo Park, M.D.Purpose: Advanced gastric cancer confined to the mus-
cularis propria is considered to be an intermediate-stage car- cinoma, between early and more advanced cancer from both the pathological and clinical viewpoints of the primary tumor stage. Although many prognostic factors for early gastric cancer and advanced gastric cancer have been identified, there are few reports concerning prognostic factors for gas- tric cancer invading the muscularis propria, and the charac- teristics of recurrence are not completley understood.Methods: One hundred and fifty-six patients who had under-
gone curative resection for gastric cancer invading the muscularis propria from 1992 to 2000 were retrospectively reviewed. The risk factors that determined the recurrence were investigated by univariate and multivariate analysis.Results: Disease recurred in 31 patient (19.9%) after a
median interval of 17.2 months. Based on our univariate analysis, the recurrence was associated with lymph node metastasis, tumor size and histologic type. Multivariate analysis showed that independent risk factor for the recur- rence was only lymph node metastasis. Recurrent disease patterns included hematogenous (38.7%), peritoneal (16.1%) and locoregional (25.8%).Conclusion: Lymph node metastasis is an important risk
factor of the recurrence after curative resection for gastric cancer invading the muscularis propria. Patients with lym- phatic metastasis, particularly with 4 or more nodal imvolve- ments, should undergo postoperative adjuvant therapy. (JKorean Surg Soc 2006;70:98-101)
책임저자:김종석, 서울시 성북구 안암동 5가 126-1 ꂕ 136-705, 고려대학교 안암병원 외과 Tel: 02-920-5866, Fax: 02-928-1631 E-mail: [email protected]
접수일:2005년 2월 24일, 게재승인일:2005년 4월 4일 이 논문의 요지는 2003년 대한외과학회 추계학술대회에서 구연되었음.
Key Words: Gastric carcinoma, Muscularis propria, Recur-
rence, Lymph node metastasis중심 단어: 위암, 고유근층, 재발, 림프절 전이 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, College of Medicine, Korea University, Seoul, Korea
김호일 외:고유근층 위암의 근치적 절제술 후 재발에 관한 위험인자
99
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 흉부 X-선 검사 및 복부 초음파나 컴퓨터 단층촬영을 이용하여 시행하였다.
재발의 확인 방법은 복부 컴퓨터 단층촬영, 위 내시경 및 시험적 개복술을 근거로 하였다. 재발 양상은 복막 파종, 혈 행성 재발, 국소 및 영역재발로 구분하였고 잔위에 재발한 경우와 복강 내 원격 림프절 전이를 국소 및 영역 재발에 포함하였다.
통계 분석은 SPSS for window 10.0을 이용하였으며 생존
곡선은 Kaplan-Meier method를 이용하여 구하였고 log-rank test로 검정하였다. 임상병리학적 인자들에 대한 비교 분석 은 Chi-Square test를 이용하였고, 재발에 영향을 미치는 위 험인자들에 대한 다변량 분석은 logistic regression analysis 를 사용하였다. P-value가 0.05 미만인 경우에 통계학적으로 유의하다고 판정하였다.
결 과
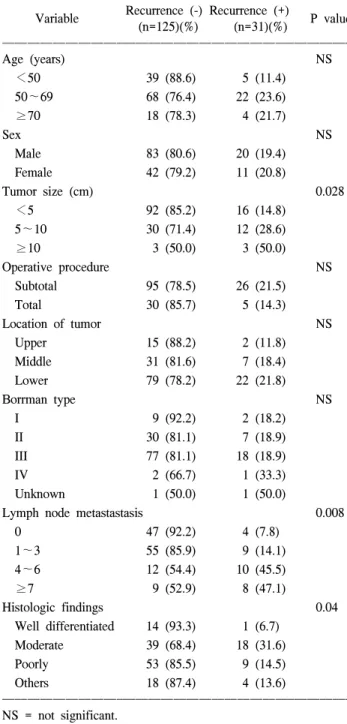
1) 재발과 관련된 임상병리학적 인자들에 분석 전체 대상 환자 중 남자가 103예(66%), 여자가 53예(34%) 로 남녀 성비는 1.94:1이었으며 평균연령은 56.1세(범위:
28∼77세)였다. 림프절 전이는 104예(67.1%)에서 발견되었 고 림프절 전이가 있는 경우의 재발률이 26.0%로 림프절 전이가 없는 경우의 7.8%보다 매우 높게 나타났다.
재발에 영향을 미치는 임상병리학적 인자를 확인하기 위 하여 단변량 분석을 시행한 결과 통계적으로 의미 있는 차 이를 보인 것은 병소의 크기(P=0.028), 림프절 전이(P=0.008), 조직형(P=0.04)이었다(Table 1).
고유근층 위암에 있어 재발에 영향을 미치는 인자들에 대한 다변량 분석을 시행한 결과 림프절 전이 여부만이 위 험도 4.120 (95% confidence interval: 1.356∼12.513)의 독립 적인 위험인자로 나타났다. 림프절 전이 숫자에 따라 림프 절 전이가 1∼3개인 경우, 4∼6개인 경우, 7개 이상인 경우 로 나누었을 때 림프절 전이가 4∼6개인 경우와 7개 이상인 경우가 각각 위험도 9.791 (95% confidence interval: 2.612∼
36.706)과 10.444 (95% confidence interval: 2.585∼42.185)의 독립적인 위험인자로 나타났다(Table 2).
2) 재발의 양상
재발한 31예(19.8%)의 재발 양상을 분석한 결과 혈행성 전이에 의한 재발이 12예(38.7%)로 가장 높은 것으로 나타 났다. 혈행성 전이의 재발 장기는 간이 10예(83.3%)로 가장 Table 1. Comparison of clinicopathological factors in patie
ns with gastric cancer invading the muscularis propria w ith recurrence (+) and without recurrence (-)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Recurrence (-) Recurrence (+)
Variable P value
(n=125)(%) (n=31)(%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Age (years) NS
<50 39 (88.6) 5 (11.4)
50∼69 68 (76.4) 22 (23.6)
≥70 18 (78.3) 4 (21.7)
Sex NS
Male 83 (80.6) 20 (19.4)
Female 42 (79.2) 11 (20.8)
Tumor size (cm) 0.028
<5 92 (85.2) 16 (14.8)
5∼10 30 (71.4) 12 (28.6)
≥10 3 (50.0) 3 (50.0)
Operative procedure NS
Subtotal 95 (78.5) 26 (21.5)
Total 30 (85.7) 5 (14.3)
Location of tumor NS
Upper 15 (88.2) 2 (11.8)
Middle 31 (81.6) 7 (18.4)
Lower 79 (78.2) 22 (21.8)
Borrman type NS
I 9 (92.2) 2 (18.2)
II 30 (81.1) 7 (18.9)
III 77 (81.1) 18 (18.9)
IV 2 (66.7) 1 (33.3)
Unknown 1 (50.0) 1 (50.0)
Lymph node metastastasis 0.008
0 47 (92.2) 4 (7.8)
1∼3 55 (85.9) 9 (14.1)
4∼6 12 (54.4) 10 (45.5)
≥7 9 (52.9) 8 (47.1)
Histologic findings 0.04
Well differentiated 14 (93.3) 1 (6.7)
Moderate 39 (68.4) 18 (31.6)
Poorly 53 (85.5) 9 (14.5)
Others 18 (87.4) 4 (13.6)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ NS = not significant.
Table 2. Cox regression analysis of data for patients with gast ric cancer invading the muscularis propria
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ 95% confidence Covariate P value Odd ratio
interval ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Lymph node metastasis 0.012 1.923 1.356∼12.513 (negaive, positive)
Lymph node metastasis (number of positive) 0
1∼3 0.302 1.923 0.556∼6.647
4∼6 0.001 9.791 2.612∼36.701
≥7 0.001 10.444 2.585∼42.185
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
100
대한외과학회지:제 70 권 제 2 호 2006ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
많았다(Table 3).
재발까지의 기간은 평균 17.2개월(5∼63개월)로 2년 이내 의 조기재발이 21명으로 74.2%를 차지하였다.
3) 고유근층 위암의 생존율
고유근층 위암으로 수술 받은 환자의 평균 생존기간은 95개월로 전체 5년 생존율은 80.9%이고 5년 병 외 생존율은 77.7%였다(Fig. 1).
재발한 환자의 경우 중앙 생존기간은 24개월로 3년 이내 에 사망한 환자가 74%를 차지하였다. 재발하지 않은 환자 의 5년 생존율은 97%였고 재발한 환자의 5년 생존율은 13.2%였다(Fig. 1).
고 찰
최근 내시경의 발달과 건강에 관한 관심의 증가 등에 의 하여 전체 위암에서 조기 위암의 비율이 높아지고 있고 이 와 더불어 고유근층 위암의 빈도도 증가하고 있다.(6) 본 연 구의 경우에 고유근층 위암은 전체 위암의 11.5%를 차지하 고 전체 5년 생존율은 80.9%로 다른 연구 결과들과 비슷하 게 나타났다.
본 연구의 대상기간 동안의 고유근층 위암의 재발률은 19.8%로 Takeuchi 등(7)의 22.2%와 비슷한 결과를 보여주고 있다. 이 결과 역시 조기위암과 진행성 위암의 사이에 있는 것으로 재발하지 않은 경우의 5년 생존율은 97%였다. 재발 의 양상을 보면 본 연구에서는 고유근층 위암의 경우 혈행 성 전이가 복막전이의 두 배 이상을 차지하는 것으로 나타 났다. 고유근층 위암의 경우 장막층에 암세포가 노출되지 않았으므로 복막전이가 혈행성 전이보다 낮게 나타난다.(7) 혈행성 전이 중 간 전이가 가장 높은 것으로 나타났는데 Yoshikawa 등(2)은 간 전이가 고유근층 위암에 있어 가장 흔하고 치명적인 재발 형태라고 하였다. 이러한 결과들은 고유근층 위암의 재발에 있어서는 그 형태가 오히려 조기 위암과 가깝고 따라서 고유근층 위암은 진행성 위암과는 종양의 특성이 다른 조기 위암과 진행성 위암의 중간 단계
에 해당함을 보여주고 있다. 그러므로 고유근층 위암의 술 후 추적관찰에 있어서는 혈행성 전이, 특히 간 전이를 찾아 낼 수 있는 방사선학적 검사들이 보다 중요하다고 할 수 있다. 또한 최근 연구 결과 위암의 간 전이에 대한 간 절제 술과 간 혈관 내 항암제 주입 등의 치료가 환자의 생존율에 영향을 줄 수 있다고(8) 하므로 조기에 간 전이를 발견하여 적극적인 치료를 시행하는 것에 대한 필요성을 고려해보아 야 한다.
본 연구에서 재발까지의 기간은 평균 17.2개월(5∼63개 월)로 2년 이내의 조기재발이 74.2%를 차지하였다. 위암의 재발은 수술 시부터 24개월까지를 조기, 수술 후 24개월에 서 60개월까지의 재발을 중기, 60개월 이후의 재발을 만기 로 혹은 24개월 이후 전체를 만기로 흔히 나누는데 재발의 경우 50% 이상이 24개월 이내의 조기재발을 보인다고 하며 문헌에 따라서는 86%까지도 보고되고 있다.(9) 그러므로 수술 후 첫 2년 동안은 보다 적극적인 추적 관찰이 요구된 다.
고유근층 위암에 대한 여러 연구 결과에서는 종양의 크 기, 종양의 위치, 종양의 육안형, 림프절 전이, 종양의 조직 형, 정맥 침윤 여부 등이 예후에 영향을 주는 것으로 보고하 고 있다.(5-7,10) Takeuchi 등(7)은 고유근층 위암의 재발을 예측하는 데 있어서 림프절 전이 여부와 종양의 위치가 중 요하다고 하였는데 본 연구 결과에서도 재발의 위험인자로 림프절 전이 여부가 가장 중요하였다. 종양의 위치는 관계 가 없었는데 이것은 상부 위암과 하부 위암에서 각각 식도 와 십이지장으로 침윤된 경우가 없었기 때문으로 생각한 다.
본 연구에서 림프절 전이 여부와 더불어 림프절 전이 개 수에 따른 세부 분석을 해본 결과 림프절의 수가 많을수록 재발의 위험성이 높아지는 것으로 나타났다. 특히 림프절 의 전이 개수가 4개 이상인 경우가 림프절 전이가 없거나 Table 3. Site of recurrence after curative resection of gastric
cancer invading the muscularis propria in 31 patients ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Site of recurrence Number of patient (n=31) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Hematogenous 12 (38.7%)
Liver 10
Lung 1
Brain 1
Peritoneal 5 (16.1%)
Local and lymph node 8 (25.8%)
Other, unknown 6 (19.4%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Fig. 1. Survival curves of gastric cancer invading the muscularis propria with or without recurrence after curative surgery.
0 1.0
.8 .6 .4 .2
60 40
20
Cum survival
Time (months)
Recurrent (n=31) All (n=156) Non-recurrent (n=125)
0.0
김호일 외:고유근층 위암의 근치적 절제술 후 재발에 관한 위험인자
101
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 1∼3개의 전이 림프절이 있는 경우 보다 재발의 위험도가의미 있게 증가하는 것으로 나타났다. 본 연구의 경우 전이 된 림프절 수에 따라 분류하면 림프절 전이가 있는 경우의 83.4%가 N1군에 속하여 다양한 예후를 보이는 환자들을 동 일한 병기로 분류하게 된다. 따라서 고유근층 위암에 있어 서 현재의 UICC/AJCC 기준의 림프절 군의 분류를 일률적 으로 적용하는 것보다 더 광범위한 연구를 통하여 림프절 전이 개수에 따라 재발 위험군을 분류하는 것도 고유근층 위암의 치료 계획을 세우는 데 도움이 될 수 있을 것으로 생각한다.
결 론
고유근층을 침윤한 위암의 근치적 절제술 후 림프절 전 이 여부가 재발의 가장 중요한 위험인자로 특히 전이 림프 절의 수가 4개 이상인 경우에는 재발의 위험률이 보다 높아 지므로 적절한 술 후 보조적 항암 화학 요법 및 철저한 추 적 관찰이 필요하며, 앞으로 보다 더 정확한 재발 위험군의 예측을 위해서 림프절 전이 개수에 따른 세부 분석에 대한 광범위한 연구가 필요하리라 본다.
REFERENCES
1) Japanese Research Society for Gastric Cancer. The general rules for the gastric cancer study in surgery and pathology. Jpn J Surg 1981;11:127.
2) Yoshikawa K, Maruyama K. Characterisitcs of gastric cancer
invading to the proper muscle layer-wih special reference to mortality and cause of death. Jpn J Clin Oncol 1985;15:
499-503.
3) Noguchi Y, Imada T, Matsmoto A, Coit DG, Brennan MF.
Radical surgery for gastric cancer. A review of the Japanese experience. Cancer 1989;64:2053-62.
4) Kaibara N, Nishidoi H, Kimura O, Makino M, Sumi K, Koga S. Analysis of results of surgical treatment for gastric cancer.
Retrospective survey of 1215 curatively resected cases. Dig Surg 1988;5:124-7.
5) Maehara Y, Anai H, Moriguchi S, Watanabe A, Tsujitani S, Suimachi K. Gastric carcinoma invading muscularis propria and macroscopic appearance. Eu J Surg Oncol 1992;18:131-4.
6) Kenjiro N, Takfumi K, Naoki O, Naoko K, Masao T. How can we detect, evaluate, and cure intermediate-stage carcinoma of the stomach. Am J Gastroenterol 1999;94:2251-5.
7) Takeuchi H, Kakeji Y, Tokunaga E, Koga T, Maehara Y, Sugimachi K. Prediction of recurrence after curative resection of gastric carcinoma invading the muscularis propria: a multiple analysis. Gastric Cancer 2000;3:28-32.
8) Katsuyuki K, Shigetoyo S, Yasuyuki S, Shinji O, Jun S, Narutoshi N, et al. Evaluation of treatment for synchronous hepatic metastases from gastric cancer with special reference to long-term survivors. Surg Today 2002;32:587-93.
9) Park CH, Park JG, Kim JP. Clinical analysis on recurrence pattern of gastric cancer. J Korean Cancer Assoc 1990;22:
556-66.
10) Yokota T, Kunii Y, Teshima S, Yamada Y, Saito T, Kikuchi S, et al. Gastric cancer with invasion limited to the muscularis propria. Int Surg 1999;84:7-12.