접수일: 2009년 9월 4일 게재승인일: 2009년 11월 18일
교신저자: 이미숙, 130-702 서울시 동대문구 회기동 1 경희의료원 감염내과
Tel: 02-958-1634, Fax: 02-958-8026, E-mail: [email protected]
내과 중환자실에서 발생한 Carbapenem 내성 Acinetobacter baumannii 유행의 위험 인자 분석 및 감염 관리
문송미1ㆍ손준성1ㆍ이희주2ㆍ천희경3ㆍ김미라3ㆍ이미숙1
경희대학교 의학전문대학원 내과학교실1, 진단검사의학교실2, 경희의료원 감염관리실3
The Analysis of Risk Factor and Infection Control of Carbapenem-Resistant Acinetobacter baumannii in a Medical Intensive Care Unit
Song Mi Moon
1, Jun Seong Son
1, Hee-Joo Lee
2, Hee Kyung Chun
3, Mee La Kim
3, and Mi Suk Lee
1Departments of Internal Medicine
1and Laboratory Medicine
2, Kyung Hee University School of Medicine, Infection Control Office, Kyung Hee University Medical Center
3, Seoul, Korea
Background: An epidemiologic study was performed after the outbreak of carbapenem-resistant Acinetobacter baumannii (CRAB) in the medical intensive care unit (MICU) from December 2006 to May 2007.
Methods: A retrospective case-control study was performed using the medical records of the patients. The case and control patients were compared for age, gender, total length of stay in MICU, prior carbapenem use, Acute Physiology and Chronic Health Evaluation II (APACH II) score, presence of central line, effect of mechanical ventilation, and sputum suction. Environmental and hand-washing studies were performed during the outbreak.
Results: Ten CRAB-affected patients and 29 controls were enrolled in this study. Univariate analysis showed that the age, total length of stay in MICU, presence of central line, and prior carbapenem use were associated with the CRAB outbreak. However, multivariate analysis showed that only prior carbapenem use was associated with the CRAB outbreak (odd ratio: 8.67, P=0.01). The outbreak disappeared after implementing a combined infection control strategy, including the sequential disinfection of MICU and strict compliance with cross-transmission prevention protocols.
Conclusion: The use of carbapenem was associated with an increased risk of CRAB infection. This study suggests that the MICU contamination and infection transmission by health-care workers played a major role in the CRAB outbreak. Novel strategies such as restricted use of broad-spectrum antibiotics, strict hand hygiene, strict isolation of the patients, and MICU disinfection may be required to prevent the CRAB outbreak.
Keywords: Acinetobacter baumannii, Carbapenem resistance, Intensive care unit
서 론
1970년대 Enterobacteriaceae과의 세균들이 병 원 감염의 주요 원인균으로 대두되면서 이들의
치료를 위해 많은 광범위 항균제가 도입되었다.
이후 광범위 항균제의 급격한 사용 증가는 다제 내성을 보이는 Pseudomonas aeruginosa, Stenotro- phomonas maltophilia 및 Acinetobacter spp. 등의 호기성 그람음성간균의 감염 증가를 가져왔다.
다제내성 그람음성간균은 기존의 항균제는 물론
이고 상대적으로 새로운 약제인 cefotaxime, cefta-
zidime, imipenem, meropenem, tobramycin, amika-
cin 및 fluoroquinolone에 대한 내성까지 보고되고
있으며[1-3], 이 중 carbapenem 내성 Acinetobac-
ter spp.는 면역력이 저하된 환자에게서 산발적 감염을 일으키고, 중환자실 등에서 집단 감염을 유발하고 있다. 이러한 집단 감염의 발생과 함께 다제내성 균주의 특성에 의해 치료의 어려움을 겪고 있어 최근 큰 문제로 대두되고 있다[1,2].
Acinetobacter spp.는 자연 환경 및 사람의 피부, 구강, 호흡기, 위장관 등에 존재하는 상재균이나, 그 중 Acinetobacter baumannii는 중환자실과 같은 숙주 저항력이 저하된 고위험군에서 폐렴, 뇌수 막염, 복막염, 심내막염 및 균혈증 등의 병원 감 염을 일으킨다[1,2,4]. 이러한 A. baumannii의 중 환자실내 감염 발생 및 집단 발병이 문제가 되는 이유는 최근 carbapenem-resistant A. baumannii (CRAB)가 급격히 증가하면서 그 치료에 어려움 을 겪고 있기 때문이다[5].
CRAB의 병원감염은 1991년 미국 뉴욕에서 처 음으로 보고 되었으며, 이후 세계 여러 나라에서 급격히 증가하고 있다. 2003년 우리 나라에서 시 행한 항균제 감수성 실태 조사 결과에 따르면 A.
baumannii의 carbapenem 내성 비율은 13%까지 보 고되었으며[6], CRAB 발생의 위험인자로는 중환 자실 입원, carbapenem계열 항균제나 3세대 ceph- alosporin계열 항균제의 치료력 등이 언급되고 있 다[7,8].
저자들은 2006년 12월 내과 중환자실에서 CRAB 균주의 기준시기 발병률(attack rate)이 1.1 에서 12.1로 증가하고, 관리도(control chart)는 시 그마 수준 II (sigma level II)에서 상한선(upper limit)보다 높게 확인됨을 파악하고, 즉 CRAB의 중환자실내 유행발생을 확인하여 이에 대한 역 학 조사 및 위험 요인 분석을 시행하였다.
대상 및 방법
1. 대상
CRAB 유행 시기로 판단된 2006년 12월부터 2007년 5월까지 내과 중환자실에 입원한 20세 이 상의 환자들 중 발열이 확인된 환자를 대상으로 하였다. 내과 중환자실은 15개 병상으로 대부분 20세 이상의 성인 환자들이 입원하며, 약 50%에 서 호흡기계 질환으로 입원하였다. 혈액, 소변, 객담 등의 배양 검사에서 CRAB가 분리된 환자
를 환자군(N=10)으로, 배양 검사에서 CRAB가 분 리되지 않은 환자를 대조군(N=29)으로 정하여 후 향적 사례-대조군 연구(retrospective case-control study)를 시행하였다.
2. 방법
혈액, 소변, 객담 검체 등에서 분리된 A. bau- mannii를 대상으로 MicroScan system (Dade Beh- ring, West Sacramento, CA, USA)을 이용하여 항 균제 감수성 검사를 시행하였다. Clinical and Laboratory Standards Institute (CLSI)에서 제시한 디스크확산법으로 colistin (Sigma, St. Luois, MO, USA)에 대한 최소억제농도(minimal inhibitory concentration, MIC)를 측정하였다[9]. 감수성 검사 에 이용된 항균제는 ciprofloxacin, moxifloxacin, levofloxacin, amikacin, gentamicin, tobramycin, imi- penem, meropenem, aztreonam, piperacillin-tazo- bactam, ceftazidime, piperacillin, ticarcillin-clav- ulanic acid, cefepime, ceftriaxone, cefotaxime, am- picillin-sulbactam, colistin 및 trimethoprim-sulfame- thoxazole이었다.
CRAB 획득의 위험요인 분석을 위해 CRAB가 분리된 환자군과 동일 기간 내과 중환자실 입원 중 CRAB가 분리 되지 않은 대조군에 대해 의무 기록을 확인하여, 성별, 나이, 진료과, 중환자실 총 재원기간, CRAB 분리 전 중환자실 재원 기 간, 요로카테터 삽입, 중심정맥관 사용, 인공호흡 기 적용, 객담 흡인 간호의 적용, 정맥 고영양제 투여, CRAB 분리 전 carbapenem계열 항균제 사 용 여부 및 Acute Physiology and Chronic Health Evaluation II (APACH II) score를 분석하였다.
전파 경로 확인을 위해 CRAB가 분리된 환자 의 침상, 인공호흡기의 부속품 등에 대한 환경 배양 및 의료진의 손 배양 검사를 시행하였다.
3. 통계학적 분석
수집된 자료는 단변량 분석을 통해 통계학적
으로 유의한 CRAB 감염의 위험 요인을 확인하
고자 하였고, 각 분석 결과의 통계적인 유의성은
95% 신뢰 구간 또는 P 값으로 제시하였으며, P
값이 0.05 미만인 경우 유의한 것으로 간주하였
다. 단변량 분석에서 P 값이 0.05 미만으로 유의
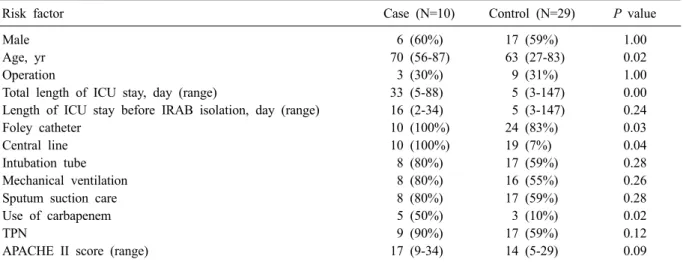
Table 1. Univariate analysis of risk factor for carbapenem-resistant Acinetobacter baumannii
Risk factor Case (N=10) Control (N=29) P value
Male 6 (60%) 17 (59%) 1.00
Age, yr 70 (56-87) 63 (27-83) 0.02
Operation 3 (30%) 9 (31%) 1.00
Total length of ICU stay, day (range) 33 (5-88) 5 (3-147) 0.00
Length of ICU stay before IRAB isolation, day (range) 16 (2-34) 5 (3-147) 0.24
Foley catheter 10 (100%) 24 (83%) 0.03
Central line 10 (100%) 19 (7%) 0.04
Intubation tube 8 (80%) 17 (59%) 0.28
Mechanical ventilation 8 (80%) 16 (55%) 0.26
Sputum suction care 8 (80%) 17 (59%) 0.28
Use of carbapenem 5 (50%) 3 (10%) 0.02
TPN 9 (90%) 17 (59%) 0.12
APACHE II score (range) 17 (9-34) 14 (5-29) 0.09
Abbreviations: ICU, intensive care unit; IRAB, imipenem-resistant A. baumannii; TPN, total parenteral nutrition;
APACHE, acute physiologic and chronic health evaluation.
Table 2. Multivariate analysis of risk factors for carba- penem-resistant Acinetobacter baumannii
Risk factor OR CI95 P value
Age, yr 0.93 0.86-1.01 0.10
Total length of 1.03 0.99-1.07 0.19 ICU stay, day
Central line 1.53 1.17-1.99 0.99 Use of carbapenem 8.67 1.55-48.49 0.01 Abbreviations: OR, odds ratio; CI95, 95% confidence interval.
하게 나온 변수에 대해서는 로지스틱 회귀분석 을 통한 다변량 분석을 시행하였으며, 교차비 (odds ratio) 및 95% 신뢰구간을 측정하여 위험 요인을 분석하였다. 모든 통계적 분석은 SPSS (SPSS 12.0 SPSS inc., Chicago, IL, USA)를 이용 하였다.
결 과
1. 항균제 감수성 결과 및 전파 경로
혈액, 소변, 객담 등에서 분리된 A. baumannii 에 대해 항균제 감수성 결과 colistin에만 감수성 을 갖고, imipenem과 meropenem에 내성을 보이는 A. baumannii가 동정된 10명을 CRAB 환자군으로 분류하였다. CRAB가 분리된 환자의 침상, 인공 호흡기의 부속품과 주변 환경에서 환경 배양을 시행하여, 25개 검체 중 9개에서 CRAB 분리를 확인하였다. 당시 관찰된 의료진의 손씻기 수행 률은 27.4% 였고, 의료진의 손 배양에서 CRAB는 분리 되지 않았다.
2. CRAB 감염의 위험요인 분석
CRAB가 분리된 환자군 10명과 CRAB가 분리 되지 않았던 대조군 29명을 비교하여 위험요인 확인을 위한 단변량 분석을 시행하였다. 환자군 의 경우 6명(60%)이 남자였으며, 대조군에서는 남자가 17명(59%)으로 두 군의 성별에 따른 통계
학적 유의성은 없었다. 그러나 환자군이 평균 연 령 70세(범위 56-87세)로 대조군 63세(범위 27-83 세)보다 높았으며, 이는 단변량 분석결과 P=0.02 로 CRAB 감염과 관련하여 통계적 유의성이 있 었다. 또한 단변량 분석에서 중환자실 총 재원기 간(P=0.00), 중심정맥관 여부(P=0.04), CRAB 분 리 전 carbapenem 항균제 사용(P=0.02)이 CRAB 감염의 위험요인이었다(Table 1).
단변량 분석에서 확인된 CRAB 유행의 위험요 인들에 대해 다변량 분석을 시행하였고, 그 결과 CRAB 분리 전의 carbapenem 항균제 사용(교차비 8.67, P=0.01)이 CRAB 감염 유행 발생의 위험 요 인이었다(Table 2).
3. 의료진의 손씻기 수행률 및 환경관리
2006년 12월 CRAB 유행 확인 후 전파방지를
위한 환경관리로 의료진의 손씻기 활동을 강조
Fig. 1. Epidemic curve of patients with carbapenem-resistant Acineto- bacter baumannii in medical in- tensive care unit.
하였고, 그 결과 중재 전 의료진 손씻기 수행률 은 27.4%였으나 중재 후 71.4%로 중가하였다. 손 씻기 시행과 함께 의료진에 대해 가운 및 장갑 착용을 격려하는 등 CRAB 분리 환자 접촉 시 격 리 지침 준수를 교육하였으며, 인공호흡기, 호흡 보조기구 소독 관리 및 중환자실 환경 소독을 강 화하였다. CRAB 균주의 유행 발생은 2006년 12 월부터 2007년 5월까지 6개월 동안 지속된 후 2007년 6월에 추가 발생이 없으면서 종결되었다 (Fig. 1).
고 찰
Acinetobacter spp.는 중환자실 입원 환자나 면역 기능이 저하된 환자들에게 패혈증, 요로 감 염, 수막염, 폐렴 등을 유발하는 비교적 병독성이 약한 균이지만[10], 최근 다제내성 Acinetobacter spp.의 분리가 늘고, 이로 인한 유행 발생이 증가 하면서 병원 감염의 심각한 원인균으로 대두되 고 있다[11,12]. 특히 Acinetobacter spp.에 의한 병 원 감염의 문제는 중증 환자에서 발생하며, 항균 제 다제내성을 보여 치료제 선택에 어려움이 있 으며, 환경에서도 오래 살아 남을 수 있는 세균 학적 특성으로 환자간 전파의 병원소가 될 수 있 다는 점이다[13].
1970년대 Acinetobacter spp.에 의한 감염은 am- picillin, minocycline, carbenicillin, gentamicin, 2세 대 cephalosporin으로 치료가 가능했으나 현재 이 들 약제가 더 이상 효과를 보이지 않는다. Acine- tobacter spp.가 다제내성을 획득하는 기전은 매우
다양하다. Ceftazidime에 대해 AmpC β-lactamase 를 포함한 chromosomal cephalosporinases를 형성 함으로써 내성을 획득하며, ticarcillin에 대해서는 plasmid-mediated penicillinase를 통해 내성을 획득 하는데, 이 기전은 fluoroquinolone, aminoglycoside 에 대한 내성 획득과도 관련이 있는 것으로 알려 져 있다. Imipenem에 대해서는 plasmid-mediated carbapenemase 및 세포외막의 투과성을 떨어뜨리 거나 penicillin 결합 단백질을 변화시킴으로써 내 성을 획득한다[14,15]. 과다한 항균제 사용이 병 원 획득성 감염의 발생 증가와 더불어 다제내성 균의 증가를 초래한 것으로 여겨져 왔으며, 이런 현상은 이미 많은 연구 결과를 통해 확인되었다 [16-18]. 기존 연구 결과에서 CRAB 병원감염의 주요 유발 인자로 장기 입원, 저체중, 중증 선행 질환, 입원 환자의 밀집도, 기관내 삽관, 혈관내 도관 삽입 등의 침습적 시술, 수술 및 광범위 항 균제의 장기 투여 등이 알려져 있다[19,20].
2006년 12월부터 2007년 5월까지 내과 중환자 실에서 발생한 CRAB 감염 유행을 조사한 본 연 구의 단변량 분석에서 환자의 연령, 중환자실 재 원기간, 중심정맥관 삽관 여부, CRAB 분리 전 carbapenem 항균제의 사용 여부가 CRAB 감염의 위험인자로 확인되었다. 또한 단변량 분석 결과 위험 요인으로 확인한 항목에 대해 로지스틱 회 귀분석을 통한 다변량 분석을 시행한 결과 CRAB의 유행은 이전의 carbapenem 사용에 대해, P 값 0.01, 교차비 8.67로 연관성을 갖고 있었다.
기존의 연구 결과들에서는 carbapenem계열 항균
제 내성 여부와 관계 없이 A. baumannii 유행의
위험 요인 등을 단순히 확인하는 것에 그쳤으며 [21,22], 이전의 항균제 사용과의 관련성 분석에 서도 carbapenem계열 항균제 사용과의 연관성을 확인한 논문은 아직까지 발표된 바가 없기에 본 논문의 결과는 차별화될 수 있겠다.
결론적으로 2006년 12월부터 2007년 5월까지 의 CRAB 유행 발생은 carbapenem 사용이 유의한 위험인자였다. 본 연구와 별도로 유행기간 동안 중환자실에서 분리된 모든 CRAB 임상균주와 의 료 기구를 포함한 환경 검체 배양에서 자란 균주 에 대해 PFGE 분석을 실시한 양 등[23]의 연구결 과에서 그 전파 경로는 분리 환자의 호흡기구와 주변 환경의 오염으로 밝혀졌었다. 이에 대한 감 염 관리 활동으로 의료진의 손씻기 활동을 증진 시키고, 가운 및 장갑 등의 보호장비 착용을 통 한 CRAB 분리환자의 접촉 격리 지침 준수를 교 육하였으며, 인공호흡기 및 호흡 보조기구의 적 절한 관리와 환경 소독을 강화하였다. 이후 2007 년 7월에 새로운 CRAB 분리 환자의 발생이 없 었으며, 이에 CRAB의 내과 중환자실내 유행은 종결되었다. CRAB의 반복적 유행 방지를 위해 서는 의료진의 손씻기를 강조하고 환경 오염에 대한 관리와 더불어 carbapenem 등의 광범위 항 생제 투여에 대한 적절한 감시와 조절이 반드시 필요함을 다시 한번 강조하고자 한다.
요 약
배경: Acinetobacter baumannii는 자연 환경 및 사람의 피부, 구강, 호흡기, 위장관내에 존재하는 상재균이다. 하지만 중환자실 입원 환자처럼 숙 주 저항력이 저하된 고위험군에서는 병원 획득 감염의 주요 원인균으로 작용하며, carbape- nem-resistant A. baumannii (CRAB) 등 다제내성균 의 증가로 치료에 많은 어려움을 겪고 있다. 저 자들은 내과 중환자실에서 2006년 12월부터 2007 년 5월까지 CRAB의 유행을 확인하고, 이에 대한 역학조사 및 위험 요인 분석을 시행하였다.
방법: CRAB 유행 시기로 판단된 2006년 12월 부터 2007년 5월까지 중환자실에 입원한 20세 이 상의 환자들을 대상으로, 발열이 확인된 환자에 대한 혈액, 소변, 객담 등의 배양 검사를 시행하
였다. 그 결과 CRAB가 분리된 환자를 환자군 (N=10)으로, CRAB가 분리되지 않은 환자를 대조 군(N=29)으로 정하여 후향적 사례-대조군 연구를 시행하였다. 전파 경로 확인을 위해 CRAB가 분 리된 환자의 침상, 인공호흡기의 부속품 등에 대 한 환경 배양 및 의료진의 손배양 검사를 시행하 였다.
결과: 임상 검체 및 환경 배양에서 분리한 CRAB 균주는 carbapenem계열 항균제인 imipe- nem, meropenem에 대한 내성뿐만 아니라 colistin 을 제외한 다른 항균제들에도 내성을 갖고 있는 다제내성 균주였다. CRAB가 분리된 환자의 침 상, 인공호흡기의 부속품과 주변 환경에서 시행 한 25개 검체 중 9개에서 CRAB이 배양되었다.
환자군과 대조군의 CRAB 획득 위험 요인 분석 에서 나이(P=0.02), 중환자실 재원 기간(P=0.00), 중심정맥관 삽입(P=0.04), CRAB 분리 전 carba- penem계열 항균제의 사용(P=0.02)이 통계적으로 유의한 위험요인이었고, 다변량 분석 결과 CRAB 분리 전 carbapenem계열 항균제 사용이 중환자실 내 CRAB 유행 발생의 유의한 위험인자임을 확 인하였다(교차비: 8.67).
결론: 내과 중환자실 내 CRAB 감염은 carba- penem계열 항균제의 광범위한 사용과 밀접한 연 관성이 있으며, 그 유행은 CRAB 분리 환자의 호 흡 기구와 주변 환경을 통한 전파로 발생하였다.
이에 CRAB의 병원 감염 발생 및 전파 방지를 위 해 의료진의 손씻기 등이 강조되어야 하며, 철저 한 환경 소독 및 격리 시행 등 환경 감염 관리에 힘써야겠다. 더불어 CRAB 유행 발생의 주된 위 험 요인으로 확인된 carbapenem계열 항균제 사용 에 있어 이의 적절한 투여 여부를 감시, 관리하 는 정책 역시 반드시 필요하겠다.
참 고 문 헌