Vol. 18, No. 4, September, 2006
비구 골절의 수술적 치료
김종오∙정덕문
이화여자대학교 의과대학 정형외과학교실
서 론
비구 골절은 교통사고나 추락사고등 고 에너지로 인한 손상에서 발생하는 흔하지 않은 골절이다. 해부학적 특성 상 다른 부위의 손상에 비해 골절 형태의 입체적인 양상의 파악과 수술적 접근의 어려움 등으로 인해 다른 골절에 비 해 정복과 내고정이 쉽지 않아 과거에는 전위의 허용범위 가 넓고, 보존적 치료를 시행하는 경우가 많았었다. 그러 나 최근에는 비구 골절에 대한 수술적 정복 및 내고정이 점차 보편화되고 있는 추세로 중요한 체중 부하 관절로서 장기적인 결과를 위한 정확한 해부학적 정복 및 조기 관절 운동의 중요성이 강조되면서 그 수술의 적용 범위가 확대 되고 있다.
해부학
Acetabulum은 incomplete hemispherical socket으 로 articular surface가 nonarticular cotyloid fossa를 둘러싸고 있는 구조이다. 이 articular socket은 2개의 column으로 둘러싸여 있고 또한 지지되고 있다.
anterior column은 iliac crest, iliac spine, acetabulum의 anterior half로, posterior column은 ischium, ischial spine, acetabulum의 posterior half 와 sciatic notch를 형성하는 dense bone으로 구성되어 있다. 이 Column의 개념은 골절의 분류뿐 아니라 골절의 양상과 수술적 접근법 및 내고정술을 논하는데 있어서 중 요하다. Acetabulum의 Dome은 체중 부하를 받는 부분 으로서 골절의 치료목적상 femroal head의 concentric reduction과 함께 anantomic restoration을 회복하는 것이 매우 중요하다고 할 수 있다. Quadrilateral suface 는 true pelvic cavity의 lateral border를 형성하는
flat plate로 서 비 구 의 내 벽 에 근 접 하 여 있 고 iliopectineal eminence는 anterior column의 prominence로서 이 두 구조물은 얇고 대퇴골에 인접하여 내고정에 제한을 준다.
neurovascular structure로서 sciatic nerve는 piriformis muscle 밑으로 greater sciatic notch를 통 과한다. Superior gluteal atery 와 nerve는 greater sciatic notch 최상부를 통과하는데 greater sciatic notch 상부의 골절이나 extensive approach시 술전 angiography로 patency를 확인하여야 한다. corona mortis는 external artery (또는 inferior epigastric atery) 와 obturator atery와 anastomosis를 이루는 혈 관으로 ilioinguinal approach시 ligation이 필요할 수 있다.
비구 골절의 분류
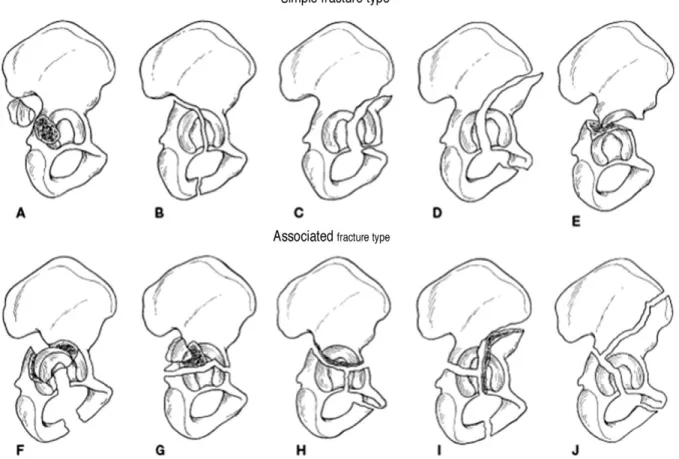
Letournel 과 Judet 분류가 현재 가장 널리 쓰이고 있 고 크게 두 가지 type으로 나눈다. 첫번째는 simple fracture type으로 posterior wall, posterior column, anterior wall, anterior column의 fracture와 transeverse fracture이고, 두번째는 associated fracture type으로 T-shape fracture, posterior column & wall fracture, transeverse & posterior wall fracture, anterior column fracture &
hemitransverse posterior fracture와 both column fracture로 구분된다(Fig.1). 이중 both column fracture란 비구의 어떤 articular fragment도 bony continuity를 유지하지 못하며, 또한 ilium과 sacroiliac joint를 분리하는 axial skeleton fracture line이 어떤 articular surface와 연결되지 못하는 골절을 의미한다.
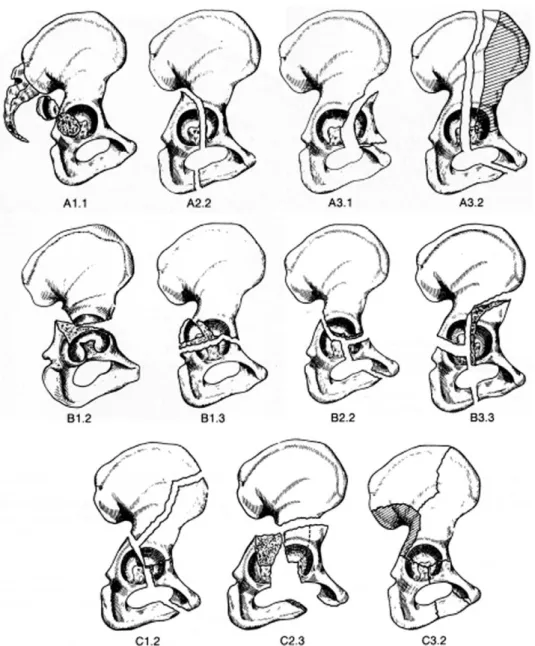
AO group 분류는 fracture의 severity에 따라 알파벳 순으로 나누었다. type A는 single wall 또는 column fracture이고, type B는 anterior & posterior column fracture(transverse, or T-type fracture)이며, type C 는 Letournel과 Judet 분류상의 Both column fracture로서 roof를 포함한 모든 articular segment가
※ 통신저자 : 김 종 오
서울특별시 양천구 목동 911-1번지 이화여자대학교 의과대학 정형외과학교실 Tel: 82-2-650-5276
Fax: 82-2-642-0349
E-mail: [email protected]
남아있는 ilium과 분리되어 있는 것을 말한다(Fig. 2).
그러나 통상적인 분류에 의해 같은 type의 골절에 대해 anatomic reduction을 한 경우에도 각각 다른 치료결과 를 보이는 경우가 있다. 이에 Tile은 Letournel과 AO group분류에는 포함되지 않지만 예후에 영향을 미치는 요 소가 있으므로, AO group분류에 qualifier(femoral head subluxation/dislocation, acetbular or femoral articular surface damage, intraarticular fragment, and nondisplaced fractures)를 포함시키자 고 제안했다.
비구 골절의 수술적 적응증
문헌마다 여러 가지 적응증을 제시하고 있지만 중요한 것은 치료 목적이 acetabulum의 weight bearing dome 의 articular congruity의 회복과 acetabulum 내의 femoral head의 stability를 얻는 것이다.
첫째, acetabulum dome에서 2 mm이상의 전위된 골 절이 있으면 수술의 적응증이 되는데, dome을 지나는 골 절이란 Matta에 의하면 3개의 방사선 사진에서 roof arc 가 45도 미만일 때, 최근의 연구에서는 AP roof arc는 25도 미만, medial roof arc는 45도 미만, posterior
roof arc가 75도 미만일 때로 보고있다. 이는 CT 상에서 acetabulum의 최상부에서 10mm이내를 지나는 골절선 이 있을 때도 알 수 있다.
둘째, femoral head의 instability가 있을 때 적응증 이 된다. 이는 전위된 acetabular fracture에서 femoral head의 subluxation이 있을 때, posterior wall의 artcular surface를 50% 이상 침범했을 때, 50% 미만이지만 임상적으로 90도 hip flexion시에 instability가 발생하는 경우이다.
그 외에도, 비구내에 osteochondral fragment로 인해 서 concentric reduction되지 않는 경우, polytrauma, open reduction을 요하는 ipsilateral displaced femoral neck fracture에서도 수술의 적응증이 될 수 있다.
수술적 접근 방법
1. Indication for the anterior approach
Ilioinguinal approach는 entire anterior acetabulum을 볼 수 있는 접근 방법으로서 anterior wall of acetabulum, anterior column, inner table of innomiate bone, quadrilateral surface에 도달할
Fig. 1. Letournel & Judet classification of acetabular fractures.
수 있다. 그렇지만 intraarticular visualization이 불가 능하다는 단점이 있다. Bilateral ilioinguinal approach 시에는 entire anterior half of pelvic ring, symphysis pubis, iliac fossa, anterior aspect of both SI joint까지 도달할 수 있다.
Iliofemoral approach는 hip joint 상방에 main displacement가 있는 anterior column fracture에 사 용한다. 그러나 iliopectineal eminence의 distal로는 access가 힘들다는 단점이 있다. adduction 과 internal rotation하면 exposure가 좋아진다. 주로 iliopectineal eminence의 distal로 extension이 없는 anterior column과 anterior wall fracture가 적응증이다.
2. Indication for the posterior approach
Kocher-Langenbeck approach는 acetabulum의 posterior wall과 post column에 도달할 수 있다.
quadratus femoris(ascending branch of MCFA), sciatic nerve, branch of inferior gluteal nerve, superior gluteal nerve & artery(greater sciatic notch)를 주의해야 한다. Sciatic nerve의 protection을 위해서는 수술 중 knee를 반드시 flexion시켜야 되며, short external rotator의 muscle belly의 retraction 시 주의하여야 한다. Superior gluteal artery와 nerve 는 greater sciatic notch에서 빠져나오며 만일 혈관의 손상이 발생하면 20분동안 packing을 해야한다.
Fig. 2. AO group classification of acetabular fractures.
3. Extensile acetabular approaches
Extended iliofemoral approach는 inner & outer table of ilium, acetabulum, both ant. & post.
column의 complete exposure를 할 수 있다. 그러나 acetabulum segments의 devascularizing risk가 있는 것이 단점이다.
Triradiate extensile approach는 anterior &
posterior column, inner iliac wall, anterior aspect of SI joint, outer aspect of innomiate bone, complex acetabular fracture의 접근시 사용될 수 있으 며 hip abductor의 ischemic necrosis를 예방할 수 있는 장점이 있다.
4. Combined anterior and posterior approach
Both column fracture 때 이용할 수 있다. Lateral position으로 동시에 접근할 수 있고 Complication은 다 른 단독 extensile approach와 큰 차이가 없다고 보고하 고 있다.
합병증
1. 사망률
0~2.5%로 보고하고 있다. 60세 이상에서는 overall mortality rate는 5.7%라 보고하고 있다.
2. posttraumatic arthritis
Letournel에 의하면 940예의 acetabular fracture의 개방적 정복 및 내고정술을 시행한 결과 posttraumatic arthritis는 년당 17%라 하였다. 418개의 perfect reduction에서는 10.8%, 151개의 imperfect reduction 에서는 35.7%의 posttraumatic arthritis를 보였다.
Both colum fracture와 transeverse fracture에서 더 안 좋은 결과를 보이는데 이는 imperfect reduction에서 기인한다고 본다.
3. 무혈성 괴사
2년 이내의 AVN(<2yrs)의 비율은 posterior dislocation 이 동반된 경우 7.5%, 다른 fracture가 동 반된 경우는 1.6%로 나타난다. 특히 posterior wall fracture에서의 AVN은 과도한 fracture site의 expsure나 손상된 posterior capsule로 인해 fracture
fragment로의 blood supply가 차단되기 때문으로 여겨 진다.
4. 감염
1~5%로 보고된다. 감염을 증가시키는 요소로는 suprapubic catherization이나 Morel-Lavallee lesion 등이 있다.
5. 신경마비
Sciatic nerve palsy의 경우는 initial injury시 10~15%, 수술 후 2~6%로 나타난다. 특히 Kocher- Langenbeck이나 Extensile approach시 더 흔하다.
6. 이소성 골 형성
대부분 extensile approach에서 prophylaxis를 하지 않을 경우 14~50%에서 발생한다. Kocher-Langenbeck approach시 prophylaxis를 하지 않을 경우 25%정도에 서 보이나, Ilioinguinal approach 시에는 드물다. 예방 으로는 indomethacin 25 mg을 하루 세번씩 4~6주간 쓰거나 radiation therapy를 할 수 있다.
7. Thromboembolic Complication
Thromboembolic Complication으로는 DVT가 8~61%까 지 보 일 수 있 으 며 , MRV(magnetic resonance venography)가 venogram보다 더 나으며, MRV는 34%의 asymtomatic DVT 환자를 detection 할 수 있다. Pulmonary embolism은 2~6%에서 나타날 수 있다. Preopertive Screening으로서 Duplex Doppler scan이 유용하다. 고위험군으로는 old(>60), anticoagulation에 contraindication인 환자, obesity, malignancy, prior DVT 환자 등이다. Contraindication 이 아니면 술 후 warfarin 사용 후 enoxaparin을 6 주 동안 계속하는 것이 좋다.
비구골절 치료로서 THR
적응증으로는 femoral head superior portion의 severe osteochondral injury가 있는 acetabular fracture, injury후 3주가 지난 comminuted, incongruous, both-column fracture, injury후 4주가 지난 severe marginal impaction이 있는 posterior fracture-dislocation등이다. 그러나 primary THR시 poor prognosis를 보이고 acetabular component가 단
기간에 이완이 오는 단점이 있다. 또한 cemented socket 을 사용할 경우 단기간의 loosening 및 revision rate가 4~5배나 된다.
REFERENCES
11) Johnson EE, Kay RM and Dorey FJ: Heterotropic ossifiacation prophylaxis following operative treatment of acetabular fractures. Clin Orthop, 305:88-95, 1994.
12) Judet R, Judet J and Letournel E: Fractures of the acetabulum: classification and surgical approaches for open reduction J . Bone and Joint Surg , 46-A:1615-1647, 1964.
13) Letournel E: Acetabulum fractures, classification and management. Clin Orthop, 151:81-106,1980.
14) Letournel E: The treatment of acetabular fractures through the Iloinguinal approach, Clin Orthop, 292:62- 76,1993.
15) Matta JM, Anderson LM, Epstein HC and Hendricks P: Fractures of the acetabulum. Clin Orthop, 205:230- 240, 1986.
16) Matta JM: Operative treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop, 305:10-
19, 1994.
17) Matta JM: Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after injury. J Bone Joint Surg, 78A(11):1632-1645,1996.
18) Mayo KA: Open reduction and Internal Fixation of Fractures of the Acetabulum. Clin Orthop, 305:31-37, 1994.
19) Mears DC and Rubash HE: Extensile exposure of the pelvis. Contemp Orthop, 6:21-31, 1983.
10) Johnson EE, Matta JM, Mast JW and Letournel E:
Delayed reconstruction of acetabular fractures 21-120 Days following injury. Clin Orthop, 305;20-30, 1994.
11) Olson SA and Matta JM: The computerized tomography subchondral arc: a new method of assessing acetabular articular continuity after fracture. J Orthop Trauma, 7(5):402-413,1993.
12) Rowe CR and Lowell JD: Prognosis of fractures of the acetabulum. J Bone Joint Surg, 43A:30-59, 1961.
13) Tile M.: Fractures of the pelvis and acetabulum, 2nd ED.
Philadelphia, Williams & Wilkins, 259-304, 1995.
14) Weber M, Berry DJ and Harmsen WS: Total hip arthroplasty after operative treatment of an acetabular fracture. J Bone Joint Surg, 80A(9):1295-1305, 1998.