https://doi.org/10.14734/PN.2020.31.1.14 pISSN 2508-4887•eISSN 2508-4895
Jaeyoung Park, MD, Minji Ko, MD, Byung Soo Kang, MD, Jihyun Park, MD, Hyun Sun Ko, MD, PhD, In Yang Park, MD, PhD Department of Obstetrics and Gynecology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Objective: To evaluate the cerebroplacental ratio (CPR) to predict adverse perinatal outcomes in small-for-gestational-age (SGA) pregnancies.
Methods: The study was a retrospective study of cases of pregnant women with SGA babies delivered between 32 and 41 weeks’ gestation, in Seoul St. Mary’s Hospital between January 2009 and December 2015. We analyzed the neonatal adverse outcomes and the risk of emergency cesarean section due to non-reassuring fetal heart rate in pregnancies with norrnal CPR and abnormal CPR in Doppler ultrasonography.
Results: The abnormal CPR in SGA pregnancies was significantly associated with neonatal intensive care unit admission (P=0.042) and neonatal seizure (P=0.042), in multivariate logistic regression analysis. In receiver operating characteristic curves, the area under the curve (AUC) of abnormal CPR and severe SGA (less than 5th percentile) was 0.59, with sensitivity of 28.4% and specificity of 90.6%
(P=0.038), in the emergency cesarean section due to non-reassuring fetal heart rate. However, bet- ween 32-36 weeks’ gestation, AUC of abnormal CPR was 0.7 with sensitivity of 70.6% and specificity of 69.2% (P=0.019) and AUC of abnormal CPR and severe SGA was 0.77, with sensitivity of 64.7% and specificity of 84.6% (P=0.001), in the emergency cesarean section due to non-reassuring fetal heart rate.
Conclusion: When SGA is expected after 32 weeks’ gestation, measurement of CPR might be useful in predicting neonatal adverse outcome. Abnormal CPR was highly predictive of cesarean section due to non-reassuring fetal heart rate, in severe SGA, between 32-36 weeks’ gestation.
Key Words: Doppler, Infant, small for gestational age, Pregnancy outcome
서론
태아발육지연이 의심될 경우 산전 평가에서 도플러 초음파검사는 태아 안녕을 평가하는 중요한 방법 중 하나로 사용되고 있다.1 특히, 제대동맥의 도플러 초음파에서 이완혈류 소실 또는 역류는 분만 결정에 영향을 미치는 주요인자이며, 태아 중간대뇌동맥(middle cerebral artery) 도플러를 평가하는 것은 태아 빈혈을 진단하는 방법 중 하나로 사용되어 왔다.
태아발육지연 의심 태아에서 제대동맥 또는 중간대뇌동맥의 박동지수(pulsatility index) 역시 태아의 혈류를 평가하는 지표로 시도되었으나 단독인자로서는 임상적인 유의성이 낮게 보고되어 왔다. 최근 중간대뇌동맥과 제대동맥의 박동지수의 비인 cerebroplacental ratio (CPR)가 임신의 불량 예후 예측에 의미가 있음이 보고되고 있는데, CPR은 산소 부 족 및 태반 혈류 저항 증가에 따른 보상 작용으로 뇌혈관 확장으로 이완혈류를 증가시킴 으로써 뇌혈류를 증가시키고, 제대동맥의 저항 증가로 이완혈류가 감소하는 초기 현상을 대변한다. CPR은 분만 후 나쁜 예후를 예측하는 중요한 도구로써, 부당경량아(small-for- gestational-age)와 만삭에 가까운 정상 체중아의 태아 상태를 평가하는데 의미가 있음이 Received: 13 March 2019
Revised: 21 June 2019 Accepted: 14 October 2019 Correspondence to Hyun Sun Ko, MD, PhD Department of Obstetrics and Gynecology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea
Tel: +82-2-2258-6176 Fax: +82-2-595-1549
E-mail: [email protected] Copyright© 2020 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any
Cerebroplacental Ratio to Predict Adverse
Perinatal Outcomes in Small-for-Gestational-
Age Pregnancies
량 예후와 연관성이 있는지에 대하여 알아보았다. 또한, 태아곤 란의증에 의한 제왕절개 수술의 예측에 있어 CPR 값의 영향을 분석하였다.
대상 및 방법
이 연구는 서울성모병원에서 2009년 1월부터 2015년 12월 까지 32주 0일에서 41주 6일 사이에 부당경량아를 분만한 산모 들을 대상으로 시행한 후향적 연구로 가톨릭대학교 임상윤리연 구심의위원회의 승인을 받았다(KC17ZESI0171). 부당경량아는 한국 기준 재태 연령에 따른 출생 체중 곡선(Korean reference curves for the birth weight)을 따라 출생 시 체중 10백분위수 미만인 경우로 정의하였으며, 5백분위수 미만을 중증 부당경량 아로 정의하였다.3 제대동맥과 중간대뇌동맥의 도플러 초음파 검사 결과가 없거나 불완전한 경우, 사산, 다태아, 선천성 기형 이 있는 경우, 제대동맥 이완기 혈류 소실이나 역전된 경우에는 연구 대상에서 제외하였다.
초음파를 이용하여 중간대뇌동맥과 제대동맥의 박동지수를 측정하였다. CPR은 중간대뇌동맥의 박동지수와 제대동맥의 박 동지수의 비로 정의하였으며, 2015년 미국산부인과학회지에서 제시된 CPR calculator에 따라, 해당 주수 값의 5백분위수 미만 인 경우 비정상적인 것으로 보았다.2 CPR의 측정값은 분만진통 시작 전 또는 제왕절개 수술 시작 전 24시간 이내에 측정된 값을 분석에 이용하였다.
임상적 특성은 산모 나이, 태아 성별, 임신 전 체질량 지수, 분만 시 체질량 지수, 재태 연령, 출생 체중, 출산력, 만삭 전 조 기 양막파수, 임신성 당뇨, 임신 전 고혈압 등 임신과 동반된 합 병증, 제왕절개술 기왕력, 양수과소증(양수량지수 5 미만)에 대 하여 분석하였다. 주산기 예후는 호흡성 산증(제대동맥의 pH가 7.2 미만이지만 base deficit 10 mEq/L 미만인 경우), 대사성 산 증(제대동맥의 pH가 7.1 미만이거나 base deficit 10 mEq/L 이 상인 경우), 태아곤란의증으로 인한 제왕절개, 출생 후 아프가 점수(1분, 5분), 출생 후 48시간 이내에 신생아 중환자실 입원 율, 신생아 호흡장애 증후군, 출생 후 48시간 이내 기계적 인공 호흡기 적용, 패혈증, 경련, 두개내 출혈, 섭식 곤란, 양수 태변착 색에 대하여 분석을 진행하였다.
통계학적 분석은 SPSS version 18.0 (SPSS Inc., Chicago, IL, USA)을 이용하였으며 P-value가 0.05 미만인 경우 통계학적으 로 유의한 것으로 보았다. 산모 나이, 체질량 지수, 출산력, 임신 성 고혈압, 당뇨 같은 임신성 합병증을 동반한 경우, 신생아 성 별, 출생아 체중, 재태 연령을 포함하여 다변량 로지스틱 회귀분
석(logistic regression models)을 시행하였고 승산비(odds ratio, ORs)와 95% 신뢰구간을 계산하였다. Receiver operating cha- racteristic (ROC) 곡선을 이용하여 부당경랑아에서 CPR 값이 5백분위수 미만으로 비정상인 경우 신생아 중환자실 입원 예측 도와 제왕절개 예측도에 대하여 분석하였으며, 중증 부당경량 이면서 비정상 CPR 수치를 보이는 경우 예측도를 분석하였다.
결과
1. 임상적 특징
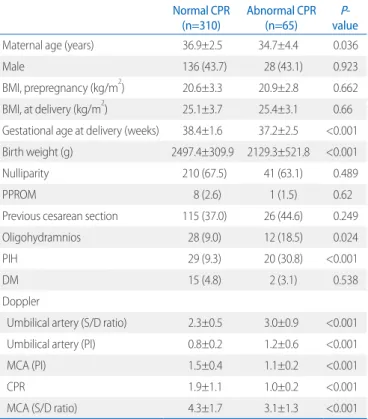
총 375명의 단태아 중에서 CPR 수치에 따라 310명의 정상 CPR군과 65명의 비정상 CPR군으로 분류되었고, 산모와 신생 아의 임상적 특성을 분석하였다(Table 1). 두 군에서 태아 성별, 산모의 분만 시 체질량 지수, 초산모 비율, 만삭 전 조기 양막파 수, 양수과소증, 임신성 당뇨, 임신성 고혈압, 제왕절개 수술의 과거력 등에서 유의한 차이를 보이지 않았다(Table 1). 산모 나 이, 출산 당시 임신 주수, 신생아 출생 체중은 정상 CPR군에서
Table 1. Demographic and Clinical Characteristics according to CPR Normal CPR
(n=310) Abnormal CPR
(n=65) P-
value
Maternal age (years) 36.9±2.5 34.7±4.4 0.036
Male 136 (43.7) 28 (43.1) 0.923
BMI, prepregnancy (kg/m2) 20.6±3.3 20.9±2.8 0.662
BMI, at delivery (kg/m2) 25.1±3.7 25.4±3.1 0.66
Gestational age at delivery (weeks) 38.4±1.6 37.2±2.5 <0.001 Birth weight (g) 2497.4±309.9 2129.3±521.8 <0.001
Nulliparity 210 (67.5) 41 (63.1) 0.489
PPROM 8 (2.6) 1 (1.5) 0.62
Previous cesarean section 115 (37.0) 26 (44.6) 0.249
Oligohydramnios 28 (9.0) 12 (18.5) 0.024
PIH 29 (9.3) 20 (30.8) <0.001
DM 15 (4.8) 2 (3.1) 0.538
Doppler
Umbilical artery (S/D ratio) 2.3±0.5 3.0±0.9 <0.001
Umbilical artery (PI) 0.8±0.2 1.2±0.6 <0.001
MCA (PI) 1.5±0.4 1.1±0.2 <0.001
CPR 1.9±1.1 1.0±0.2 <0.001
MCA (S/D ratio) 4.3±1.7 3.1±1.3 <0.001
Values are presented as mean±standard deviation or number (%).
Abbreviations: CPR, cerebroplacental ratio; BMI, body mass index; PPROM, preterm premature rupture of membrane; PIH, pregnancy-induced hypertension; DM, diabetes mellitus; S/D ratio, systolic/diastolic ratio; PI, pulsatility index; MCA, middle cerebral artery.
프가 점수, 호흡성 산증, 신생아 호흡장애 증후군, 신생아 패혈 증, 기계적 인공호흡기 적용, 섭식 곤란, 양수혼탁과 같은 신생 아 이환율과 비정상적 CPR 수치는 유의한 관련이 없었다. 그 러나 대사성 산증(P=0.023), 태아곤란의증에 의한 제왕절개술 (P=0.002), 신생아 경련(P=0.004), 신생아 중환자실 입원(P<
0.001), 신생아 두개내 출혈(P=0.008)은 정상 CPR군에 비하여 비정상 CPR군에서 유의하게 높게 나타났다. 로지스틱 회귀분 석에서 비정상 CPR은 다변량 분석에서도 신생아 중환자실 입 원율(P=0.042)과 신생아 경련(P=0.042)의 유의한 위험인자로 서 각각 2.187배, 3.571배 위험도를 증가시키는 독립적 요인으 로 나타났지만 대사성 산증, 태아곤란의증에 의한 제왕절개술, 신생아 두개내 출혈은 다변량 분석에서 유의하지 않은 인자로 나타났다(Table 3).
2) ROC 곡선(ROC curves)
ROC 곡선에서 5백분위수 미만의 중증 부당경량아이면서 비 정상 CPR 수치를 보이는 경우 신생아 중환자실 입원 예측도는 area under the curve (AUC) 0.7 (P<0.001, sensitivity 60.9%
and specificity 80%)로 나타났다(Fig. 1). 임신 32-41주 사이에 중증 부당경량아이면서 비정상 CPR 수치를 보이는 경우 태아 곤란의증에 의한 응급제왕절개 예측도는 AUC 0.59 (P=0.038, sensitivity 28.4% and specificity 90.6%)였다(Fig. 2A). 이를 37주를 기준으로 구분하였을 때, 32-36주 출생의 중증 부당 경량아 단독의 AUC는 0.73 (P=0.007, sensitivity 76.5% and specificity 69.2%), 비정상 CPR 단독의 AUC는 0.7 (P=0.001, sensitivity 70.6% and specificity 69.2%), 중증 부당경량아이 면서 비정상 CPR 수치를 보이는 경우에는 AUC 0.77 (P=0.001, sensitivity 64.7% and specificity 84.6%)로 높게 나왔으나(Fig.
2B), 37-41주 만삭 출생에서는 중증 부당경량아, 비정상 CPR 모두 태아곤란의증에 의한 응급제왕절개 예측에 유의하지 않 았다(Fig. 2C).
유의하게 높게 나타났으며, 양수과소증과 임신성 고혈압의 경 우 비정상 CPR군에서 유의하게 높게 나타났다.
2. 주산기 예후(perinatal outcomes)
1) 부정적 신생아 예후(adverse neonatal outcomes)
비정상 CPR에 따른 주산기 예후를 분석하였을 때(Table 2), 제대동맥과 제대정맥의 혈액 가스분석 수치, 분만 당시 낮은 아
Table 2. Perinatal Outcomes according to Abnormal CPR Normal CPR
(n=310) Abnormal CPR (n=65) P-
value Umbilical artery gas analysis
pH 7.3±0.0 7.2±0.1 0.291
pCO (mmHg) 51.4±13.4 53.8±13.4 0.187
HCO3(mEq/L) 22.2±2.5 22.8±2.8 0.121
Base excess -5.2±3.7 -5.5±5.0 0.712
Umbilical vein pH 7.3±0.1 7.3±0.1 0.604
Respiratory acidosis 143 (46.1) 29 (44.6) 0.824
Metabolic acidosis 47 (15.1) 3 (4.6) 0.023
C/S due to non-reassuring fetal status 29 (9.3) 15 (23.1) 0.002 1 minute Apgar score, less than <5 12 (3.9) 4 (6.2) 0.404 5 minutes Apgar score, less than <5 1 (0.3) 0 (0) 0.647
NICU admission 60 (19.3) 34 (52.3) <0.001
RDS 9 (2.9) 2 (3.1) 0.937
Mechanical ventilation 15 (4.8) 5 (7.7) 0.349
Sepsis 16 (5.1) 3 (4.6) 0.859
Seizure 9 (2.9) 7 (10.8) 0.004
Any intracranial hemorrhage 10 (3.2) 7 (10.8) 0.008
Feeding difficulties 8 (2.6) 3 (4.6) 0.374
Meconium stained amniotic fluid 18 (5.8) 4 (6.2) 0.909 Values are presented as mean±standard deviation or number (%).
Abbreviations: CPR, cerebroplacental ratio; C/S, cesarean section; NICU, neonatal intensive care unit; RDS, respiratory distress syndrome.
Table 3. Logistic Regression of Abnormal Cerebroplacental Ratio for Adverse Perinatal Outcomes
Univariate analysis Multivariate analysis
OR 95% CI P-value aOR 95% CI P-value
Metabolic acidosis 0.27 0.08-0.90 0.023 0.37 0.10-1.30 0.123
C/S due to non-reassuring fetal status 2.91 1.46-5.83 0.002 1.61 0.71-3.63 0.247
NICU admission 4.58 2.61-8.05 <0.001 2.18 1.03-4.64 0.042
Seizure 4.05 1.45-11.31 0.004 3.57 1.04-12.19 0.042
Any intracranial hemorrhage 3.63 1.33-9.93 0.008 0.54 0.10-2.88 0.476
Multivariate analysis was adjusted by maternal age, gestational age, prepregnancy maternal body index, birth weight, parity, neonatal sex, maternal diabetes, pregnancy induced hypertension, and premature rupture of membrane.
Abbreviations: OR, odd ratio; CI, confidence interval; C/S, cesarean section; NICU, neonatal intensive care unit.
높다는 것을 보고한 바 있다.5 그러나 이번 연구에서 만삭 임신 만을 대상으로 분석한 결과는 중증 부당경량이면서 비정상 CPR 을 보이는 경우에도 태아곤란의증에 의한 제왕절개 수술 예측 에 유의하지 않은 결과를 보였다. 본 연구와 유사하지만 전향 적으로 진행된 37주 이상의 만삭 출생 부당경량아에서 비정상 CPR의 기준을 5백분위수 미만으로 정의하고 주산기 예후를 분 석한 세 연구 중에서, 한 연구는 비정상 CPR과 ‘태아곤란의증에 의한 제왕절개 수술’, ‘대사성 산증’, ‘신생아 중환자실 입원’, ‘복 합 주산기 불량 예후(composite adverse outcome)’와 유의한 상관관계를 나타내었고,6 다른 한 연구는 ‘태아곤란의증에 의한 제왕절개 수술’, ‘대사성 산증’과 유의한 연관성을 보고하였으 며,7 한 연구는 ‘복합 주산기 불량 예후’8와 유의한 연관성을 보 고하였다. 만삭 임신에서의 자궁내 태아발육지연 의심 시 CPR 의 의미에 대해서는 좀 더 연구가 필요할 것으로 생각된다.
2018년 보고된 메타분석에서는 CPR에 대한 연구들의 디자 인, 비정상 CPR의 기준점과 대상(부당경량아 또는 정상 체중 아), 출생 주수(32주 미만의 매우 이른 조산, 32-36주의 늦은 조산, 37주 이후 만삭) 등에 따라 민감도와 특이도가 매우 다양 하다는 것을 지적하였으나, CPR의 불량 주산기 예후에 대한 예 측 정확도에 있어 ‘태아곤란의증에 의한 제왕절개 수술’ 및 ‘복 합 주산기 불량 예후’에 있어서는 제대동맥보다 정확도가 높다 고 분석하였다.4 32주 이전의 자궁내 태아발육지연 의심 시에는 제대동맥과 정맥관의 혈류가 임상적으로 중요하지만 32주 이 후의 늦은 자궁내 태아발육지연에서는 CPR도 임상적 가치가 있을 것으로 평가된다.2,4 그러나 현재까지 보고된 32주 이후의 늦은 자궁내 태아발육지연에서 CPR의 ‘불량 주산기 예후 예측 인자’로써 민감도는 8-71%, 특이도는 47-98%로 다양하게 보 고되기 때문에2,4,9-12 이에 대한 전향적 연구들의 필요성이 강조
고찰
이 연구에서는 임신 32주 이후 부당경량아(10백분위수 미만) 들이 출산 전에 5백분위수 미만의 비정상 CPR을 보인 경우 신 생아 중환자실 입원율 및 경련과 같은 주산기의 부정적인 예후 와 관련이 있다는 사실을 알 수 있었다. 그리고 32주 이후의 중 증 부당경량아에서 CPR이 비정상적으로 나타났을 때 태아곤란 의증에 의한 응급제왕절개 예측도를 분석하였을 때, 32주에서 36주 사이의 부당경량아에서는 5백분위수 미만의 비정상 CPR 이 유의한 예측인자였지만 37주 이상의 부당경량아에서는 비 정상 CPR이 제왕절개에 대한 유의한 예측인자는 아니었다.
CPR은 아직까지 임상적 결정의 지표나 명확한 적용 기준은 확립되지 않았으나 기존의 도플러 지수와 병합하여 유용성을 평가받고 있고,4 특히 자궁내 태아발육지연 의심 시 생체물리 학 계수, 제대동맥 도플러 지수, 중간대뇌동맥 도플러 지수보 다 주산기 불량 예후 예측의 조기인자로 대두되고 있다.2 본 연 구 결과에서도 임신 32-41주에 출생한 부당경량아에서 출생 전 CPR이 비정상인 경우 신생아 중환자실 입원율 및 경련의 위 험이 증가하였는데, 임신 32-36주에서 자궁내 태아발육지연이 5백분위수 미만으로 중증이면서 CPR이 비정상인 경우 자궁내 태아곤란의증에 의한 응급제왕절개 예측의 특이도는 80% 이상 으로 높게 나타나(Fig. 2B), 비정상 CPR을 동반한 중증의 자궁 내 태아발육지연이 동반된 임신에서 분만 방법 및 분만 진행 중 집중 모니터의 필요성을 시사하였다. 본 연구진의 과거 후향적 연구에서도 5백분위수 미만의 중증 태아발육지연 임신에서 비 정상 CPR이 제대동맥의 비정상 박동지수와 함께 동반되는 경 우 분만 진행 중 태아곤란의증에 의한 제왕절개 수술의 위험이
Fig. 1. Receiver operating characteristic (ROC) curves of severe small-for-gestational-age (SGA) (birth weight less than 5th percentile), abnormal cerebroplacental ratio (CPR), or both, for predicting admission to in tensive care unit in neonates between 32 and 41 gestational weeks with SGA. AUC, area under the curve.
되고 있다.
이 논문의 제한점은 이 연구가 후향적 연구로서 산모의 기저 질환과 같은 혼란 변수와 정보 편향(information bias)을 조정 하는 데 어려움이 있었던 것이다. 이를 보정하기 위하여 영향인
자들에 대한 보정 후 로지스틱 회귀분석을 시행하였다. 또한 모 든 산모에 대한 생체물리학 계수 점수가 평가되지 않음으로 인 하여 생체물리학 계수와 CPR 점수 중 신생아 예후에 미치는 영 향의 중요도를 평가하지는 못하였다. 본 기관에서는 산전 초음 A
B
C
Fig. 2. Receiver operating characteristic (ROC) curves of severe small-for-gestational-age (SGA) (birth weight less than 5th percentile), abnormal cerebroplacental ratio (CPR), or both, for pre- dicting the emergency cesarean section due to non- reassuring fetal heart rate. (A) Between 32 and 41 gestational weeks. (B) Between 32 and 36 gestational weeks. (C) Between 37 and 41 gestational weeks. AUC, area under the curve.
파에 자궁내 태아발육지연이 의심되는 경우 미국 산부인과 교 과서에 기재된 알고리즘에 따라,13 34주 이전에는 태아 폐성숙 을 위한 스테로이드 요법을 시행하면서 태아의 심음감시장치, 생체물리학적 계수, 도플러 초음파검사를 시행하고, 제대동맥 의 이완기 혈류 역전, 태아곤란의증, 급박한 분만을 요하는 산과 적 적응증 등이 없다면 태아의 심음감시는 입원을 한 경우 매일, 입원을 하지 않은 경우 주 1-2회 측정하고, 도플러 초음파와 생 체물리학적 계수는 주 1-2회 측정을 시행한다. 34주 이후부터 만삭까지의 임신 종결 기준은 제대동맥의 이완기 혈류 소실 또 는 역전, 양수과소, 태아곤란의증, 급박한 분만을 요하는 산과적 적응증이며, 기준에 해당하지 않는 경우 태아의 심음감시는 입 원을 한 경우 매일, 입원을 하지 않은 경우 주 1-2회 측정하고, 도플러 초음파와 생체물리학적 계수는 주 1-2회 측정을 시행 한다.13 알고리즘과의 차이는 초음파를 이용한 태아 체중의 계 측을 2-3주마다 시행하고, 32주 이후 태아 성장이 2주 이상 거 의 없을 경우 분만을 고려한다. 분만의 방법은 제왕절개 수술의 산과적 적응증이 없는 경우 유도분만이 기본 방법이지만 유도 분만 시작 전 또는 진행 중에 태아 심음감시장치에서 태아곤란 이 의심되는 심음이 관찰될 경우 제왕절개 수술을 시행한다. 이 논문의 또 다른 제한점으로 과거 제왕절개 수술력이 있거나 둔 위, 태반 위치 이상 등의 제왕절개 수술을 요하는 다른 산과적 요인으로 인하여 제왕절개 수술을 시행한 산모들을 포함하였 으나, 연구에서 평가하고자 한 변수는 전체 제왕절개 수술의 위 험도를 본 것이 아니라 응급 수술을 요하는 태아곤란의증에 의 한 제왕절개 수술의 위험도만을 본 것이었고, 두 군 간 제왕절개 수술 과거력이 있는 산모의 비율은 차이가 없었기 때문에 결과 에 유의한 영향을 미치지는 않았을 것으로 생각된다. 비록 본 연 구는 후향적 연구였으나 32-36주 사이의 부당경량아에서 비정 상 CPR이 응급 제왕절개의 유의한 예측인자임을 확인하였다.
태아 안녕평가 요소로 제대동맥과 중간대뇌동맥 도플러를 사 용해왔고, 특히 이 두 가지 요소를 함께 사용한 CPR이 태아 안녕 평가에 있어 점점 더 중요한 도구로 대두되고 있다. 향후 전향적 연구를 통하여 CPR검사의 적응 대상 및 유용성에 대한 평가가 추 가적으로 이루어져야 하겠으나 특히 임신 32-36주에 부당경량 아가 예상되는 경우 CPR 값이 비정상이라면 분만 방법의 결정 및 분만 중 태아 모니터에 보다 주의가 필요할 것으로 생각된다.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
References
1) Srikumar S, Debnath J, Ravikumar R, Bandhu HC, Maurya VK. Doppler indices of the umbilical and fetal middle cerebral artery at 18-40 weeks of normal gestation: a pilot study. Med J Armed Forces India 2017;73:
232-41.
2) DeVore GR. The importance of the cerebroplacental ratio in the evalua- tion of fetal well-being in SGA and AGA fetuses. Am J Obstet Gynecol 2015;213:5-15.
3) Lee JK, Jang HL, Kang BH, Lee KS, Choi YS, Shim KS, et al. Percentile dis- tributions of birth weight according to gestational ages in Korea (2010- 2012). J Korean Med Sci 2016;31:939-49.
4) Vollgraff Heidweiller-Schreurs CA, De Boer MA, Heymans MW, Schoon- made LJ, Bossuyt PMM, Mol BWJ, et al. Prognostic accuracy of cerebro- placental ratio and middle cerebral artery Doppler for adverse perinatal outcome: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2018;51:313-22.
5) Jo JH, Choi YH, Wie JH, Ko HS, Park IY, Shin JC. Fetal Doppler to predict cesarean delivery for non-reassuring fetal status in the severe small-for- gestational-age fetuses of late preterm and term. Obstet Gynecol Sci 2018;61:202-8.
6) Garcia-Simon R, Figueras F, Savchev S, Fabre E, Gratacos E, Oros D. Cer- vical condition and fetal cerebral Doppler as determinants of adverse perinatal outcome after labor induction for late-onset small-for-gesta- tional-age fetuses. Ultrasound Obstet Gynecol 2015;46:713-7.
7) Cruz-Martínez R, Figueras F, Hernandez-Andrade E, Oros D, Gratacos E.
Fetal brain Doppler to predict cesarean delivery for nonreassuring fetal status in term small-for-gestational-age fetuses. Obstet Gynecol 2011;
117:618-26.
8) Figueras F, Savchev S, Triunfo S, Crovetto F, Gratacos E. An integrated model with classification criteria to predict small-for-gestational-age fetuses at risk of adverse perinatal outcome. Ultrasound Obstet Gynecol 2015;45:279-85.
9) Bligh LN, Alsolai AA, Greer RM, Kumar S. Cerebroplacental ratio thresholds measured within 2 weeks before birth and risk of cesarean section for intrapartum fetal compromise and adverse neonatal outcome. Ultra- sound Obstet Gynecol 2018;52:340-6.
10) Dunn L, Sherrell H, Kumar S. Review: systematic review of the utility of the fetal cerebroplacental ratio measured at term for the prediction of adverse perinatal outcome. Placenta 2017;54:68-75.
11) Meher S, Hernandez-Andrade E, Basheer SN, Lees C. Impact of cerebral redistribution on neurodevelopmental outcome in small-for-gesta- tional-age or growth-restricted babies: a systematic review. Ultrasound Obstet Gynecol 2015;46:398-404.
12) Gordijn SJ, Beune IM, Thilaganathan B, Papageorghiou A, Baschat AA, Baker PN, et al. Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound Obstet Gynecol 2016;48:333-9.
13) Cunningham FG, Leveno KJ, Bloom SL, Dashe JS, Hoffman BL, Casey BM, et al. Williams obstetrics. 25th ed. New York (NY): McGraw-Hill Education, 2018:855.