서 론
고혈압은 일반적으로 노화에 따라 유병률이 증가하는 만성질환 중 하나이며 당뇨와 밀접한 관련이 있다는 것은 잘 알려진 사실이다.
현재 우리나라 30세 이상 당뇨병 환자는 약 10%이며 이 중 거의 절반 에 가까운 환자들이 고혈압을 동반하고 있는 것으로 알려져 있다.1) 1차성 고혈압의 원인은 명확히 밝혀져 있지 않으나 심박출량 증가나 말초혈관의 저항성 증가에 의한 것으로 생각되고 있다.2) 당뇨 환자에
Original Article
당뇨가 없는 60세 이하 성인에서 공복혈당 및 당화혈색소의 구간에 따른 고혈압 유병률과의 관계
이재일, 윤진희, 김선호, 박영민*
연세대학교 의과대학 가정의학교실
Association between Hemoglobin A1c and Fasting Glucose Levels and the Prevalence of Hypertension in Nondiabetic Adults
Jae Il Lee, Jin Hee Yoon, Sun Ho Kim, Young Min Park*
Department of Family Medicine, Yonsei University College of Medicine, Seoul, Korea
Background: Several studies have shown a significant association between glycosylated hemoglobin levels and cardiovascular disease. However, because only mean blood pressure was assessed in these studies, any analysis of the association between the prevalence of hypertension and glycated hemoglobin levels was limited. In particular, few studies have investigated the relationship between the prevalence of hypertension and glycosylated hemoglobin levels specifically in the Korean population. Furthermore, by analyzing the relationship between hypertension and fasting glucose levels, which are relatively easy to measure, one can consider the possibility of using glycosylated hemoglobin and fasting glucose levels in the treatment of hypertension.
Methods: National Health and Nutrition Examination Survey 5 data from 2010, 2011, and 2012 were used in this study. Participants younger than 20 years and older than 60 years, who were diagnosed with or receiving treatment for diabetes, taking cholesterol drugs, diagnosed with a malignant disease, or had hemoglobin A1c levels of 6.5% or higher or, fasting plasma glucose levels 126 mg/dL or higher were excluded. Therefore, data form a total of 6,399 subjects were excluded.
Results: The prevalence of hypertension increased significantly among subjects with glycosylated hemoglobin levels more than 5.7%, but after considering the effects of sex, drinking, smoking status, age, body mass index, and cholesterol levels, the relative risk of hypertension according to the group stratified by hemoglobin levels was non-significant. However, the prevalence and the relative risk of hypertension significantly increased in subjects with fasting glucose levels above 100 mg/dL.
Conclusion: The results of this show that glycosylated hemoglobin and fasting blood glucose levels are significantly associated with the prevalence and relative risk of hypertension suggesting that these two factors should be considered in the treatment of hypertension.
Keywords: Glycosylated Hemoglobin A; Blood Glucose; Diabetes Mellitus; Hypertension
http://www.kafm.or.kr/kjfp.2015.5.3.179pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3):179-183
KJFP
Korean Journal of Family PracticeReceived February 25, 2015 Accepted August 28, 2015 Corresponding author Young Min Park
Tel: +82-10-9105-2818, Fax: +82-31-900-0049 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Jae Il Lee, et al. Association between HbA1c and Glucose and Hypertension
Korean Journal of Family Practice
KJFP
서 높아진 인슐린저항성으로 인해 교감신경이 자극되고 이로 인한 혈관 수축이 고혈압의 원인이 될 수 있으며, 또한 당뇨로 인한 말초혈 관의 협착은 말초조직의 산소 포화도를 낮춤으로써 심박출량을 증 가시키고 고혈압의 원인이 될 수 있다.
많은 연구에서 당화혈색소는 심혈관질환의 위험요소와 유의한 연관관계를 보여주고 있다.3-6) 또한 당화혈색소의 증가에 따라 대사 증후군 유병률의 유의한 증가를 보고하는 연구도 많이 발표되었
다.4,6-8) 그러나 이들 연구에서 사용된 혈압은 당화혈색소의 특정 구
간에 따른 평균 혈압으로 고혈압 유병률의 차이를 보는 데 있으며, 특 히 한국인을 대상으로 한 당화혈색소에 따른 고혈압 유병률과의 관 계에 대한 연구는 부족한 상태이다. 더 나아가 비교적 임상에서 측정 하기 쉬운 공복혈당과 고혈압 유병률과의 관계를 함께 알아보는 것 또한 의미 있을 것이다. 당뇨가 없는 성인에서 고혈압의 유병률을 알 게 된다면, 당뇨가 없는 성인이 고혈압으로 이행할 위험률을 어느 정 도 짐작해 보는 데 도움이 될 수 있을 것이다.
본 연구에서는 hemoglobin A1c (HbA1c) 6.5 미만, fasting glucose 126 미만, 60세 이하의 성인을 연구대상으로 제한하여, 실제적으로 당뇨 가 없는 성인들에서 fasting glucose와 HbA1c의 구간에 따른 고혈압 유병률의 상관관계에 대해 알아봄으로써 고혈압 예방을 위해 당뇨 전 단계부터 적극적인 혈당관리의 필요성에 대해 알아보고자 한다.
방 법
1. 연구대상
본 연구는 국민건강영양조사 5기 2010, 2011, 2012년 자료를 통합하 여 사용하였다. 분석대상은 20세 이상 60세 미만으로 하였고, 당뇨병 으로 진단받았거나 치료 중인 경우, 콜레스테롤 약제를 복용 중인 경우, 악성 질환(위암/간암/대장암/유방암/자궁경부암/폐암/갑상샘 암/기타 암/신부전/간경변증 유병 여부 해당)을 앓고 있는 경우, 당화 혈색소가 6.5% 이상, 공복혈당이 126 mg/dL 이상인 경우는 배제하였 다. 연구변수에 결측값이 없는 경우만 최종 대상자로 확정하였으며, 이는 총 6,399건이 해당되었다.
2. 고혈압의 정의
2014 Eighth Joint National Committee on Hypertension Guidelines에 따라 60세 이하 성인에서 당뇨나 chronic kidney disease 유무에 상관 없이 systolic blood pressure (SBP)>140 or diastolic blood pressure (DBP)>90일 경우 고혈압 양성으로 판단하였다. 고혈압 약을 복용 중 인 경우 측정된 혈압과 상관없이 고혈압 양성으로 판단하였다.
3. 분석방법
분석 프로그램은 IBM SPSS ver. 22.0 (IBM Co., Armonk, NY, USA) 를 사용하였고, 통계처리 내용은 다음과 같다. 첫째, 조사대상자의 일반적 특성을 확인하기 위해 고혈압, 당화혈색소 구간, 공복혈당 구 간, 성별, 음주, 흡연상태, 소득, 운동실천 여부의 빈도/백분율을 제시 하고 카이제곱검정(chi-square test)을 실시하였으며, 수축기혈압, 이완 기혈압, 당화혈색소, 공복혈당, 나이, 체질량지수, 총 콜레스테롤, high density lipoprotein (HDL), low density lipoprotein (LDL)의 평균, 표준 오차를 제시하고 분산분석(analysis of variance, ANOVA)을 실시하였 다. 둘째, 고혈압에 따른 당화혈색소 구간, 공복혈당 구간의 빈도/백 분율을 제시하고 카이제곱검정을 실시하였다. 셋째, 고혈압에 대한 당화혈색소 구간, 공복혈당 구간의 영향 및 상대 위험도를 확인하기 위해 각각 다변량 이항 로지스틱 회귀분석을 실시하였다. 보정변수 로서 성별, 음주, 흡연상태, 소득, 운동실천 여부, 나이, 체질량지수, 총 콜레스테롤, HDL, LDL을 같이 투입하였다.
결 과
먼저 조사대상자의 일반적 특성을 확인하기 위해 고혈압, 당화혈 색소 구간, 공복혈당 구간, 성별, 음주, 흡연상태, 소득, 운동실천 여부 의 빈도/백분율을 제시하고 카이제곱검정을 실시하였으며, 수축기혈 압, 이완기혈압, 당화혈색소, 공복혈당, 나이, 체질량지수, 총 콜레스테 롤, HDL, LDL의 평균, 표준오차를 제시하고 ANOVA를 실시하였다 (Table 1).
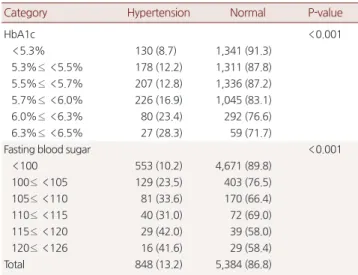
당화혈색소 구간, 공복혈당 구간에 따른 고혈압의 유병률 차이를 확인하기 위해 카이제곱검정을 실시하였다(Table 2). 당화혈색소 구 간의 차이가 유의하였다(P<0.001). 당화혈색소가 높아질수록 고혈 압의 유병률이 증가하였다. 공복혈당 구간의 차이가 유의하였다 (P<0.001). 정상군(100 미만)에 비해 공복혈당이 증가할수록 고혈압 의 유병률이 증가하였으나 비율은 약간의 차이가 있었다.
고혈압에 대한 당화혈색소 구간, 공복혈당 구간의 영향 및 상대 위 험도를 확인하기 위해 각각 다변량 이항 로지스틱회귀분석을 실시 하였다. 보정변수로서 성별, 음주, 흡연상태, 소득, 운동실천 여부, 나 이, 체질량지수, 총 콜레스테롤을 같이 투입하였다. 모든 분석에서 종 속변수인 고혈압의 기준범주는 정상으로 하였다. 따라서 오즈비 (odds ratio)는 정상군에 비해 고혈압군에 속할 확률을 의미한다.
전체 대상자에서 당화혈색소를 예측변수로 한 결과(Table 3), 당화 혈색소를 예측변수로 한 결과, 구간별 당화 혈색소의 영향은 유의한 경우가 없었다. 하지만 공복혈당을 예측변수로 한 결과(Table 4), 100 미만일 때에 비해 100-105 미만일 때 고혈압군에 속할 확률이 1.430
이재일 외. 공복혈당 및 당화혈색소와 고혈압의 연관성 Korean Journal of Family Practice
KJFP
배로 유의하게 높았다(P<0.05). 100 미만일 때에 비해 105-110 미만일 때 고혈압군에 속할 확률이 2.046배로 유의하게 높았다(P<0.001). 그 리고 100 미만일 때에 비해 115-120 미만일 때 고혈압군에 속할 확률 이 2.060배로 유의하게 높았다(P<0.05).
고 찰
최근 심혈관질환, 대사증후군과 관련하여 당화혈색소와의 연과 Table 1. Characteristics of study subjects
Variable Category Male Female P-value Hypertension Hypertension 482 (65.3) 366 (34.7) <0.001
Normal 2,069 (48.4) 3,315 (51.6) HbA1c <5.3% 608 (51.7) 881 (48.3) <0.001
5.3%≤ <5.5% 644 (51.7) 899 (48.3) 5.5%≤ <5.7% 577 (54.8) 694 (45.2) 5.7%≤ <6.0% 159 (54.4) 213 (45.6) 6.0%≤ <6.3% 41 (56.2) 45 (43.8) 6.3%≤ <6.5% 522 (44.4) 949 (55.6)
FBS <100 291 (63.5) 241 (36.5) <0.001
100≤ <105 147 (64.0) 104 (36.0) 105≤ <110 74 (70.7) 38 (29.3) 110≤ <115 46 (78.5) 22 (21.5) 115≤ <120 23 (56.5) 22 (43.5) 120≤ <126 1,970 (47.9) 3,254 (52.1) Drinking (1 y) Never 280 (29.0) 1,028 (71.0) <0.001
1 or less/mo 231 (38.3) 519 (61.7)
1/mo 801 (59.5) 800 (40.5)
2-4/mo 713 (76.8) 299 (23.2)
2-3/wk 262 (80.5) 78 (19.5)
4 or more/wk 264 (30.4) 957 (69.6) Smoking Smoker 1,205 (85.7) 235 (14.3) <0.001
Former 811 (80.8) 220 (19.2)
Never 535 (21.6) 3,226 (78.4)
Income Low 566 (50.2) 838 (49.8) 0.949
Mid-low 640 (50.3) 927 (49.7) Mid-high 673 (51.1) 948 (48.9)
High 672 (50.9) 968 (49.1)
Physical activity No 1,320 (47.1) 2,065 (52.9) <0.001
Yes 1,231 (54.4) 1616 (45.6)
Systolic blood pressure
117.96± 0.35 110.29± 0.31 <0.001
Diastolic blood pressure
79.31± 0.28 72.89± 0.21 <0.001
HbA1c (%) 5.48± 0.01 5.43± 0.01 <0.001
FBS (mg/dL) 92.56± 0.23 89.81± 0.18 <0.001
Age (y) 38.51± 0.29 39.16± 0.22 0.039
body mass index (kg/m2)
24.19± 0.09 22.84± 0.08 <0.001
Total cholesterol (mg/dL)
189.33± 0.96 186.71± 0.73 0.018
High density lipoprotein (mg/dL)
47.06± 0.28 53.71± 0.25 <0.001
Low density lipoprotein (mg/dL)
112.02± 0.82 112.65± 0.60 0.507
Total 2,551 (50.6) 3,681 (49.4)
Values are presented as mean± standard error or number (weighted %). P-value was calculated by chi-square test or analysis of variance.
HbA1c, hemoglobin A1c; FBS, fasting blood sugar.
Table 2. Prevalence of hypertension according to fasting glucose &
HbA1c
Category Hypertension Normal P-value
HbA1c <0.001
<5.3% 130 (8.7) 1,341 (91.3)
5.3%≤ <5.5% 178 (12.2) 1,311 (87.8) 5.5%≤ <5.7% 207 (12.8) 1,336 (87.2) 5.7%≤ <6.0% 226 (16.9) 1,045 (83.1) 6.0%≤ <6.3% 80 (23.4) 292 (76.6) 6.3%≤ <6.5% 27 (28.3) 59 (71.7)
Fasting blood sugar <0.001
<100 553 (10.2) 4,671 (89.8)
100≤ <105 129 (23.5) 403 (76.5) 105≤ <110 81 (33.6) 170 (66.4) 110≤ <115 40 (31.0) 72 (69.0) 115≤ <120 29 (42.0) 39 (58.0) 120≤ <126 16 (41.6) 29 (58.4)
Total 848 (13.2) 5,384 (86.8)
Values are presented as number (weighted %). P-value was calculated by chi- square test.
HbA1c, hemoglobin A1c.
Table 3. Relative risk for hypertension according to HbA1c
Category OR 95% Confidence interval
P-value
Lower Upper
HbA1c*
<5.3% 1.000
5.3%≤ <5.5% 1.021 0.751 1.387 0.895
5.5%≤ <5.7% 0.901 0.672 1.208 0.487
5.7%≤ <6.0% 0.949 0.702 1.284 0.735
6.0%≤ <6.3% 1.011 0.658 1.554 0.960
6.3%≤ <6.5% 1.076 0.570 2.029 0.822
P-value and OR was calculated by multivariate binomial logistic regression.
OR, odds ratio; HbA1c, hemoglobin A1c.
*Adjustment factor: sex, drinking, smoking, income, physical activity, age, body mass index, total cholesterol, high density lipoprotein, low density lipoprotein.
Table 4. Relative risk for hypertension according to fasting glucose
Category OR 95% Confidence interval
P-value
Lower Upper
Fasting blood sugar*
<100 1.000
100≤ <105 1.430 1.054 1.939 0.022
105≤ <110 2.046 1.418 2.950 <0.001
110≤ <115 1.518 0.921 2.502 0.102
115≤ <120 2.060 1.073 3.957 0.03
120≤ <126 1.917 0.792 4.639 0.148
P-value and OR was calculated by multivariate binomial logistic regression.
OR, odds ratio.
*Adjustment factor: sex, drinking, smoking, income, physical activity, age, body mass index, total cholesterol, high density lipoprotein, low density lipoprotein.
Jae Il Lee, et al. Association between HbA1c and Glucose and Hypertension
Korean Journal of Family Practice
KJFP
성에 대한 연구들이 활발히 진행되고 있다. 고혈당 자체만으로도 심 혈관계의 강력한 위험요인으로 평가되며, 평균적으로 당뇨가 없는 군에 비해 남성은 2-3배, 여성은 3-4배 정도 그 위험도가 증가되는 것 으로 알려져 있다.8,9) 최근에는 당뇨가 없는 군 안에서 당화혈색소와 심혈관질환 및 대사증후군 간의 상관관계에 대한 연구들이 많이 진 행되었다.2-7) 그 결과 많은 연구들이 유의성을 보고하였지만, Emerg- ing Risk Factors Collaboration 등10)이 연구한 논문에서 당화혈색소를 심혈관계 위험 예측인자로 사용하는 것에는 기존의 것에 비해 추가 적인 benefit이 없다고 보고하였다.
하지만 이들 연구에서 이용된 혈압은 당화혈색소의 특정 구간에 따른 평균 혈압으로 고혈압 유병률과의 관계를 살펴보기에 한계가 있었으며, 특히 한국인을 대상으로 한 당화혈색소에 따른 고혈압 유 병률에 대한 연구는 부족한 상태이다. 비록 predict factor로 사용하 는 것에는 아직 이견이 있을 수 있으나 당뇨가 없는 성인에서 당화혈 색소 측정을 통해 고혈압에 대한 상대위험도를 예측해 보며, 추가적 으로 비교적 쉽게 측정할 수 있는 공복혈당과의 관계에 대해서도 살 펴보는 것에 이 논문의 의의를 둘 수 있을 것이다.
당화혈색소의 경우 5.7% 이상에서 유병률 자체는 유의하게 증가 하나 성별, 음주, 흡연상태, 나이, 체질량지수, 총 콜레스테롤 등을 보 정하였을 때 구간에 따른 고혈압의 상대적 위험도는 통계적 의미가 없었다. 그러나 공복혈당은 100 이상에서 혈당의 증가에 따라 유의 한 고혈압 유병률 증가를 보였고, 구간에 따른 상대위험도 증가 또한 유의하게 나타났다.
당뇨가 없는 성인에서 공복혈당의 구간에 따른 고혈압 상대위험 도 증가가 통계적 유의함을 보인 것은 의미 있는 결과이다. 하지만 구 간의 설정에 있어 공복혈당의 정상 수치인 100을 기준으로 전후 구 간에서 너무나 확연한 유병률 차이를 보이며, 공복혈당 100-125인 구 간은 당뇨는 아니지만 공복혈당장애로 볼 수 있는 구간으로 100 미 만에서도 좀 더 세분화해 살펴보지 못한 것이 이 연구의 제한점이라 고 볼 수 있다. 또한 당화혈색소 및 공복혈당의 구간설정에 있어 n 수 의 차이를 고려해 다른 방법으로 구간을 설정한다면 더 의미 있는 결과가 나올 수도 있지 않았을까 하는 아쉬운 면이 있다.
그럼에도 불구하고, 당뇨가 없는 성인의 고혈압 유병률이 당화혈 색소 5.7% 이상에서 평균에 비해 유의하게 증가하고, 공복혈당이 100 이상인 구간에서 고혈압의 상대위험도가 구간에 따라 유의하게 증 가한다는 결과는, 비록 당뇨가 없더라도 공복혈당장애나 내당능장 애가 의심될 경우 약물 치료의 적응증은 되지 않지만 식이조절과 운 동요법을 통해 적극적인 혈당관리를 시작하는 것이 당뇨로의 진행뿐 만 아니라 고혈압의 예방에도 도움을 줄 수 있음을 보여준다 하겠다.
요 약
연구배경:
많은 연구에서 당화혈색소와 심혈관질환의 유의한 연관 성을 보여주는 논문이 발표되었다. 그러나 이들 연구에서 사용된 혈 압은 당화혈색소에 따른 평균 혈압으로 고혈압 유병률의 차이를 보 는 데 한계가 있으며, 특히 한국인을 대상으로 한 당화혈색소에 따른 고혈압 유병률과의 관계에 대한 연구는 부족한 상태이다. 더 나아가 비교적 임상에서 측정하기가 쉬운 공복혈당과 고혈압 유병률과의 관계를 함께 알아봄으로써, 고혈압 예방을 위해 당뇨 전 단계부터 적 극적인 혈당관리의 필요성에 대해 알아보고자 한다.방법:
국민건강영양조사 5기 2010, 2011, 2012년 자료를 통합하여 사 용하였다. 분석대상은 20세 이상 60세 미만으로 하였고, 당뇨병으로 진단받았거나 치료 중인 경우, 콜레스테롤 약제를 복용 중인 경우, 악성 질환을 앓고 있는 경우, 당화혈색소가 6.5% 이상, 공복혈당이 126 mg/dL 이상인 경우는 배제하여 총 6,399건이 해당되었다. 당화혈 색소와 공복혈당을 각각 6그룹으로 나누고 그룹에 따른 고혈압의 유 병률과 상대위험도를 비교하였다. 2014 Eighth Joint National Com- mittee on Hypertension Guidelines에 따라 60세 이하 성인에서 당뇨나 chronic kidney disease 유무에 상관없이 systolic blood pressure>140 or diastolic blood pressure>90일 경우 고혈압 양성으로 판단하였고, 고 혈압 약을 복용 중인 경우 측정된 혈압과 상관없이 고혈압 양성으로 판단하였다.결과:
당화혈색소의 경우 5.7% 이상에서 유병률 자체는 유의하게 증 가하나 성별, 음주, 흡연상태, 나이, 체질량지수, 총 콜레스테롤 등을 보정하였을 때 구간에 따른 고혈압의 상대적 위험도는 통계적 의미 가 없었다. 그러나 공복혈당은 100 이상에서 혈당의 증가에 따라 유 의한 고혈압 유병률 증가를 보였고, 구간에 따른 상대위험도 증가 또 한 유의하게 나타났다.결론:
당화혈색소와 공복혈당이 고혈압 유병률 및 상대위험도와 유 의한 상관관계가 있다는 결과는, 비록 당뇨가 없더라도 공복혈당장 애나 내당능장애가 의심될 경우 약물 치료의 적응증은 되지 않지만 식이조절과 운동요법을 통해 적극적인 혈당관리를 시작하는 것이 당뇨로의 진행뿐만 아니라 고혈압의 예방에도 도움을 줄 수 있음을 보여준다 하겠다.중심단어:
당화혈색소; 공복혈당; 당뇨; 고혈압 REFERENCES1. Korean Diabetes Association. Diabetes fact sheet in Korea 2012. Seoul: Ko-
이재일 외. 공복혈당 및 당화혈색소와 고혈압의 연관성 Korean Journal of Family Practice
KJFP
rean Diabetes Association; 2012.
2. Verdoia M, Schaffer A, Cassetti E, Barbieri L, Di Ruocco MV, Perrone-Filardi P, et al. Glycosylated hemoglobin and coronary artery disease in patients without diabetes mellitus. Am J Prev Med 2014;47:9-16.
3. Kim JH, Choi SR, Lee JR, Shin JH, Lee SJ, Han MA, et al. Association of he- moglobin A1c with cardiovascular disease risk factors and metabolic syn- drome in nondiabetic adults. Korean Diabetes J 2008;32:435-44.
4. Blake GJ, Pradhan AD, Manson JE, Williams GR, Buring J, Ridker PM, et al.
Hemoglobin A1c level and future cardiovascular events among women.
Arch Intern Med 2004;164:757-61.
5. Dilley J, Ganesan A, Deepa R, Deepa M, Sharada G, Williams OD, et al. Asso- ciation of A1C with cardiovascular disease and metabolic syndrome in Asian Indians with normal glucose tolerance. Diabetes Care 2007;30:1527-32.
6. Kwon YJ, Lee KM, Chung SP. Association of HbA1c with metabolic syndrome in nondiabetic adults. Korean J Fam Pract 2012;2:140-7.
7. Sung KC, Rhee EJ. Glycated haemoglobin as a predictor for metabolic syn- drome in non-diabetic Korean adults. Diabet Med 2007;24:848-54.
8. Kannel WB, McGee DL. Diabetes and cardiovascular disease: the Framing- ham study. JAMA 1979;241:2035-8.
9. Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from cor- onary heart disease in subjects with type 2 diabetes and in nondiabetic sub- jects with and without prior myocardial infarction. N Engl J Med 1998;339:
229-34.
10. Emerging Risk Factors Collaboration, Di Angelantonio E, Gao P, Khan H, Butterworth AS, Wormser D, et al. Glycated hemoglobin measurement and prediction of cardiovascular disease. JAMA 2014;311:1225-33.