334
통신저자:송 석 환
서울시 영등포구 여의도동 62
가톨릭대학교 의과대학 성모병원 정형외과 Tel:02-3779-1192ㆍFax:02-783-0252 E-mail:[email protected]
Address reprint requests to:Seok-Whan Song, M.D.
Department of Orthopedic Surgery, St Mary’s Hospital, 62, Yeouido- dong, Yeongdeungpo-gu, Seoul 150-713, Korea
Tel:82-2-3779-1192ㆍFax:82-2-783-0252 E-mail:[email protected]
원위 요골 골절의 후방 금속판 내고정술 (Dorsal Plating for Distal Radius Fracture)
송 석 환
가톨릭대학교 의과대학 정형외과학교실
서 론
최근 원위 요골의 골절 부위를 수술적으로 내고정하기 위하여 전방도달법 (anterior approach)을 이용한 많은 금 속판들이 개발되어 사용되고 있다13,15,17,18)
. 그러나 전방도달 법 자체는 관절외 원위 요골 골편이나 원위 요골 전방 관 절면의 골편이 전방으로 전위된 경우 (소위 volar Barton 골절) 전방으로 전위된 골절편에 대한 지지판 (buttress)의 기능을 하기 위하여 이전부터 사용되어 오던 방법이나 최 근에는 골다공증이 동반된 불안정성 관절내 골절까지도 금 속판에 고정된 경사각을 가진 금속나사를 이용한 금속판 (fixed volar angle screw plate)으로 전방고정술을 이용하 는 것이 최근의 변화된 추세이다.
그러나 이러한 전방고정술은 흔히 염려하는 후방고정술 의 신전건 손상에 따른 합병증을 상쇄하고도 남는 많은 합 병증을 야기하며, 장무지 굴곡건 및 수지 굴곡건, 요골동맥 의 파열뿐만 아니라 후방의 장무지 신전건 및 수지 신전건 의 파열 등 그 또한 많은 합병증이 심심하지 않게 보고되 고 있음을 주지하여야 할 것이다2,4-6,16).
원위 요골 골절의 후방도달법에 의한 금속판-금속나사의 고정은 부착된 금속판의 후방으로 주행하는 수지 신전건의 손상을 야기하는 것으로 많은 논문이 보고되고 있으며1,8,11), 이 합병증을 방지하기 위하여 또한 많은 새로운 형태의 금 속판이 개발-보고되고 있다7,21).
그러나 저자는 1994년 이래로 원위요골의 심한 분쇄골절 과 수근관절의 류마티스 관절염 혹은 외상 후 관절염에 대 하여 일반적으로 사용되는 “T”형 금속판 혹은 소형 재건 금속판 (small reconstruction plate)-금속나사를 이용하여 후방도달법으로 골절부위의 고정과 수근관절 유합술에도 합병증 없이 고정하여 왔으며, 10년 이상 현재까지 수지의
신전건 손상이 없었음을 보고하고, 통상적인 방법이기는 하나 본원에서 현재 사용하고 있는 수술적 방법을 상술하 고자 한다.
본 론
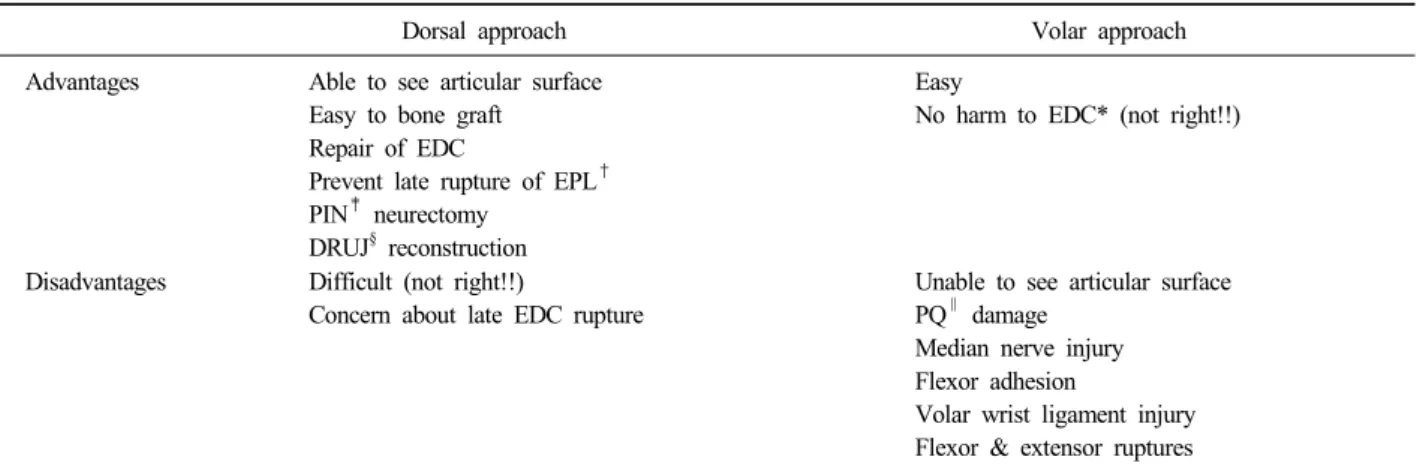
1. 후방금속판 고정의 장-단점
흔히 짐작하는 후방금속판 고정의 단점은 신전건의 손상 에 의한 파열이나 건초염으로 많은 논문에서 보고되고 있 으나 이는 수술자의 술기의 세련됨과 관련이 있다. 장무지 신전건이나 수지 신전건을 직접 보고 손상을 피하게 할 수 있으며, 관절면의 분쇄 골절 시에 관절면을 직접 보고 그 정복의 정도를 판단할 수 있고, 심하게 분쇄되어 골 이식 이 필요한 부분인 후방 골피질을 직접 보고 골 이식을 적 정하게 할 수 있다는 등의 더 많은 장점 또한 논의되고 있 어24) 후방도달법의 장점 또한 간과할 수 없는 것이다 (Table 1).
최근 사용되고 있는 전방도달법을 이용한 금속판 고정 시 후방 골 이식 혹은 요수근관절의 관절면 관찰을 위하여 요골 전방의 연부조직과 골막, 원위 요-척골 사이의 골간막 등의 심각한 손상을 초래할 수 있는 광범위 박리를 권하고 있어18), 비록 고정된 각도의 금속 나사 고정으로 조기의 관절 운동을 할 수 있다는 장점을 부각시키기는 하나 연부 조직 박리를 최소화할 수 있는 방법의 개발이 요구된다.
2. 수술 술기
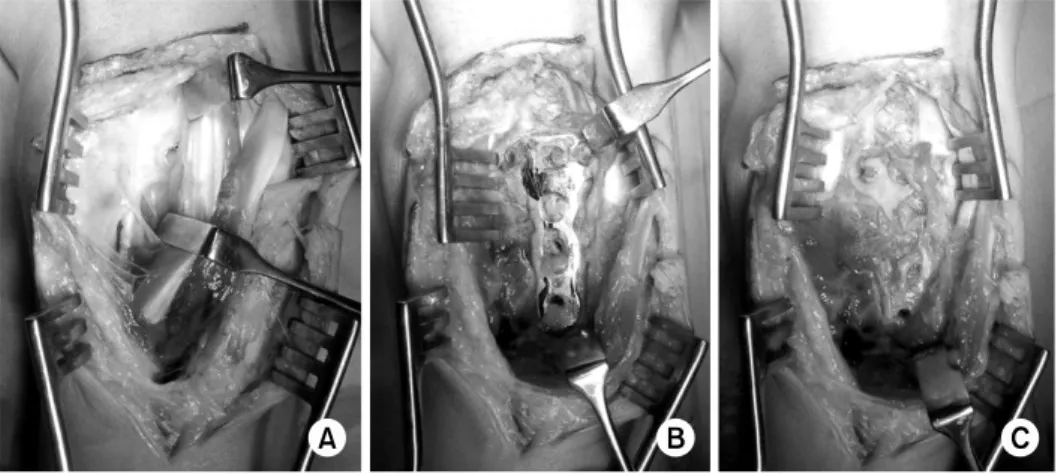
Lister 결절을 확인한 후 수근관절 배부의 중간 축 (midline)으로 골절의 범위에 따라서 zigzag 형태의 약 6∼
Fig. 1. (A) The zigzag midline incision over the dorsal wrist joint, centered on Lister tube- rcle, was designed.
(B) The entire extensor retin- aculum was divided into the distal and proximal halves, and the 3rd extensor com- partment was opened. The 2nd and 4th extensor compar- tments were dissected.
(C) Fracture site was reduced, (D) and temporarily fixed with K-wires. After the con- firmation of proper reduction
“T”-plate was fixed.
(E) The half of extensor retinaculum was used to cover the transverse part of the plate, protecting the ex- tensor tendons from the plate and screws.
(F) The other half of extensor retinaculum was used to cover extensor tendon like as the original function of reti- naculum.
Advantages Able to see articular surface Easy to bone graft Repair of EDC
Prevent late rupture of EPL† PIN‡ neurectomy
DRUJ§ reconstruction
Easy
No harm to EDC* (not right!!)
Disadvantages Difficult (not right!!)
Concern about late EDC rupture
Unable to see articular surface PQ∥ damage
Median nerve injury Flexor adhesion
Volar wrist ligament injury Flexor & extensor ruptures
*EDC: Extensor digitorum communis tendon, †EPL: Extensor pollicis longus tendon, ‡PIN: Posterior interosseous nerve, §DRUJ: distal radioulnar joint, ∥PQ: Pronator quadrates muscle.
Fig. 3. (A) Left distal radius and ulnar styloid process were fractured in 74-year old female patient.
(B) Dorsal plating and autogenous iliac bone graft were done for distal radius, and K-wires were inserted into the distal ulna.
(C) Thirteen months after the operation the plate and screws were removed without any complications to the exte- nsor tendons.
Fig. 2. (A) After the union the patients are advised to remove the plate within 6 months to prevent the possible extensor tendon injury. Note the intact extensor tendons over the plate.
(B) After the removal of screws, (C) and plate. Over and under the plate there is some thick fibrous tissue pro- tecting the extensor tendons from injury.
Fig. 4. (A) Sixty-nine year old female patient had broken her right wrist, with severe intraarticular fracture of distal radius.
(B) Combined volar and dorsal plating were done to gather up the burst fracture fragments, and external fixation to reduce compressive pressure on the radial articular surface.
(C) Seven weeks after the operation external fixator was removed.
(D) Five months after the operation removal of plates and extensor tenolysis were done.
(E) Twenty months after the operation. There is no evidence of post-traumatic arthritis and soft tissue complications.
위부로 횡으로 이분하여 놓고 제3신전구획에서 종으로 절 개하여 장무지 신전건을 유리시키며, 신전지대를 제2 및 4 구획으로 박리하여 내-외측으로 신전지대판 (extensor reti- naculum flaps)을 형성한다 (Fig. 1B). 원위 요골 골절부위 를 노출시킨 후 추후 금속판을 부착하기 위한 후방 골표면 을 고르게 하고, 이미 분쇄가 되어 있는 Lister 결절을 절 제하기도 한다 (Fig. 1C). 골절 부위를 정복 후 일시적인 고정을 위하여 K-강선을 삽입한 후 투시 방사선 검사로 만 족한 정복이 되었는지 확인하며, “T”형의 금속판을 원위 요골 배부의 모양에 맞게 변형시키고 금속판 내고정을 한 다 (Fig. 1D). 골 이식술이 필요한 경우 자가장골의 해면 골을 이식한다.
금속판 고정 후 원위부와 근위부로 나누어져 있는 신전 지대를 금속판의 횡 부분 (“T” 자의 “ㅡ” 부분)에 삽입된 금속나사가 덮혀지도록 원위 혹은 근위 신전지대를 선택하 여 제2∼4신전건 밑으로 위치시켜 금속판을 덮으며 (Fig.
1E), 나머지 근위 혹은 원위 신전지대를 신전건 위로 봉합
보호하여 파열을 방지하고, 피하 및 피부 봉합을 한다. 골 유합이 확인되면 수술 후 약 6개월 이내에 금속판-금속나사 의 제거술을 실시한다 (Fig. 2).
3. 증례분석
1994년 3월부터 본원에서 원위요골 골절 후 심한 분쇄 골절 부위를 고정하기 위하여 후방도달법에 의한 금속판- 금속나사 고정술을 받고 6개월 이상 추시가 가능하였던 52 예 (여/남:38/14)의 평균 나이는 53세 (24∼78세)였으며, 평균 추시 기간은 11개월 (6∼64개월)이었다. 수술 후 평 균 5.7개월 (3∼16개월)만에 금속판-금속나사를 제거하였으 며, 19예는 6개월 이상 추시되었으나 금속판-금속나사의 제 거술을 받지 않았다. 본 증례들에서 수술에 의하여 삽입된 금속판-금속나사의 영향으로 신전건 파열이 발생한 증례는 없었다.
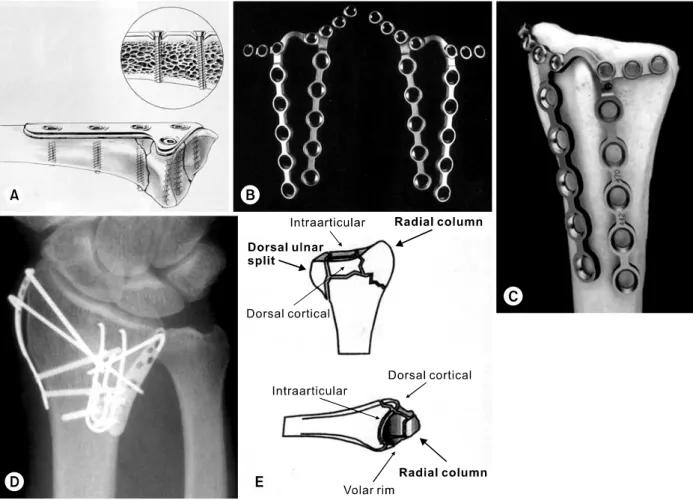
Fig. 5. Low profile plates for dorsal plating.
(A) Forte plateⓇ (Zimmer, Warsaw, IN, USA) is thinner than the conventional AO plate, and the screw head sinks into the screw hole.
(B) Pi (π) plateⓇ (Synthes, Paoli, PA) is thin and easily malleable to adapt to the complicated dorsal surface of distal radius.
Left or right preference can be chosen.
(C) Lister tubercle can be saved.
(D) Trimed SystemⓇ (Trimed, Valencia, CA) was applied to the severely comminuted distal radius fracture.
(E) Trimed and 2.4-mm AO plate (Synthes, Paoli, PA) import the concept of “column” from Melone’s classification of comminuted intraarticular fracture of distal radius, and give the opportunity to fix each fragment with specifically designed small plates.
1) 증례 1
74세 여자가 넘어져서 수상한 좌측 원위 요골 및 척골 골절로 내원하였다. 관절면은 포함하지 않았으나 후방 골 피질의 심각한 손상으로 불안정성 골절이었으며, 척골의 경상 돌기는 기저부에서 골절되어 전위되어 원위 요척관절 의 안정성을 위하여 수술적인 치료가 요구되었다 (Fig.
3A). 후방도달법으로 골절부위를 정복한 후 자가장골 이식 을 하였으며, 척골 경상돌기도 관혈적 정복 및 K-강선 내 고정을 하였다 (Fig. 3B). 원위 요골 및 척골의 K-강선은 수술 후 약 6주에 제거하였으며, 원위 요골에 부착되어 있 었던 금속판 금속나사는 수술 후 약 1년 1개월에 제거하였
다 (Fig. 3C). 최종 추시 시 굴곡 60도, 신전 70도, 회내전 70도, 회외전 80도였으며, 수지 신전건 및 굴곡건의 손상은 없었다.
2) 증례 2
69세 여자가 산행 도중 넘어져 우측 손목관절의 골절로 내원하였다. AO 분류 C3형으로 심한 관절 내 골절을 동반 하였다 (Fig. 4A). 관절면을 모아놓기 위하여 전방 및 후방 도달법으로 전-후방의 금속판을 부착하였으며, 관절면의 압 박을 피하기 위하여 외고정 기기를 사용하였고, 골 결손부 위는 자가장골 이식을 하였다 (Fig. 4B). 수술 후 7주에 외
건 박리술을 실시하였다 (Fig. 4D). 수상 후 1년 8개월 현 재 외상 후 관절염의 소견은 없으며 (Fig. 4E), 굴곡 15도, 신전 40도, 회외전 80도, 회내전 45도이나 건측에 비교하 면 63%의 관절운동을 회복하였다.
4. 새롭게 개발된 후방고정을 위한 금속판
Low profile plate라고 불리우는, 금속판의 두께가 얇거 나 원위 요골의 후방 골표면에 밀착되고, 금속나사의 머리 가 작거나 낮아 수지신전건을 자극하지 않도록 개발된 금 속판을 몇 가지 소개하면, Forte plateⓇ (Zimmer, Warsaw, IN, USA) (Fig. 5A)는 기존의 금속판과 모양은 유사하나 두께가 얇고 나사못의 머리가 금속판 속으로 낮게 위치하 여 그 위를 지나가는 신전건의 자극을 피하기 위하여 개발 되었다3,7,10,19). Pi (π) plateⓇ (Synthes, Paoli, PA) (Fig.
5B, 5C)는 얇고 가늘은, 미리 구부러진 금속판으로 좌측 혹은 우측의 요골에 선택하여 사용할 수 있으며, 요골 후 방의 골표면에 적응하여 비교적 쉽게 구부릴 수 있도록 고 안되어 있다9,12,14,16,22,23)
. Pi plate를 사용하기 위하여는 위 에서 제시한 Lister 결절을 제거하지 않아도 된다는 장점을 제시하고 있으나 사실 이미 심하게 손상된 Lister 결절이 골절 부위에 얼마나 안정성을 부여할지는 의문이다.
Trimed SystemⓇ (Trimed, Valencia, CA)과 AO의 2.4 mm 금속판 (Synthes, Paoli, PA)은 각각의 골절편을 각각 따로 고정하는 지주고정(columnar fixation)의 개념20,24)을 도입한 고정 방법이다 (Fig. 5D, 5E). 원위 요골은 요골 경 상돌기의 요골주 (radial column), 월상골와의 전방주와 후 방주로 구분되며, 이들 골편을 고정하기 위한 각각의 모양 이 고안되어 있다.
이러한 노력에도 불구하고 각각의 금속판에 따른 신전건 손상과 금속판의 골절 등 합병증에 대한 보고는 없어지지 않고 있으므로 심한 분쇄 골절의 원위 요골 골절의 치료를 위한 완벽한 내고정물은 아직 없다고 보여진다.
결 론
원위 요골 골절의 수술적 치료 시 후방 도달법에 의한 금속판-금속나사의 내고정은 후방의 수지 신전건 손상을 초래하는 것으로 보고되고 있다. 그러나 적정한 수술 술기 로 후방으로 전위된 관절면을 포함한 심한 분쇄골절도 외 고정기기와 골 이식술을 동반한 금속판 내고정술로 적절한 치료를 제공할 수 있고, 합병증을 최소화할 수 있으며, 골 유합이 확인되면 조기에 금속판-금속나사를 제거하여 그
참 고 문 헌
1) Axelrod TS, McMurtry RY: Open reduction and internal fixation of comminuted, intraarticular fractures of the dis- tal radius. J Hand Surg Am, 15: 1-11, 1999.
2) Bell JS, Wollstein R, Citron ND: Rupture of flexor pol- licis longus tendon: a complication of volar plating of the distal radius. J Bone Joint Surg Br, 80: 225-226, 1998.
3) Carter PR, Frederick HA, Laseter GF: Open reduction and internal fixation of unstable distal radius fractures with a low-profile plate: a multicenter study of 73 fractures.
J Hand Surg Am, 23: 300-307, 1998.
4) Cross AW, Schmidt CC: Flexor tendon injuries following locked volar plating of distal radius fractures. J Hand Surg Am, 33: 164-167, 2008.
5) Dao KD, Venn-Watson E, Shin AY: Radial artery pseu- doaneurysm complication from use of AO/ASIF volar dis- tal radius plate: a case report. J Hand Surg Am, 26:
448-453, 2001.
6) Douthit JD: Volar plating of the dorsally comminuted fractures of the distal radius: a 6-year study. Am J Orthop, 34: 140-147, 2005.
7) Finsen V, Aasheim T: Initial experience with Forte plate for dorsally displaced distal radius fractures. Injury, 31:
445-448, 2000.
8) Fitoussi F, Ip WY, Chow SP: Treatment of displaced in- tra-articular fractures of the distal end of the radius with plates. J Bone Joint Surg Am, 79: 1303-1312, 1997.
9) Hahnloser D, Platz A, Amgwerd M, Trentz O: Internal fixation of distal radius fractures with dorsal dislocation:
pi-plate or two 1/4 tube plates? A prospective randomized study. J Trauma, 47: 760-765, 1999.
10) Herron M, Faraj A, Craigen MA: Dorsal plating for displaced intra-articular fractures of the distal radius.
Injury, 34: 497-502, 2003.
11) Hove LM, Nilsen PT, Furnes O, Oulie HE, Solheim E, Mölster AO: Open reduction and internal fixation of dis- placed intraarticular fractures of the distal radius. 31 pa- tients followed for 3∼7 years. Acta Orthop Scand, 68:
59-63, 1997.
12) Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: a brief report. J Hand
Surg Am, 23: 737-741, 1998.
13) Keating JF, Court-Brown CM, McQueen MM: Internal fixation of volar-displaced distal radius fractures. J Bone Joint Surg Br, 76: 401-405, 1994.
14) Lowry KJ, Gainor BJ, Hoskins JS: Extensor tendon rupture secondary to the AO/ASIF titanium distal radius plate without associated plate failure: a case report. Am J Orthop, 29: 789-791, 2000.
15) Musgrave DS, Idler RS: Volar fixation of dorsally dis- placed distal radius fractures using 2.4-mm locking com- pression plates. J Hand Surg Am, 30: 743-749, 2005.
16) Nunley JA, Rowan PR: Delayed rupture of the flexor pollicis longus tendon after inappropriate placement of the pi plate on the volar surface of the distal radius. J Hand Surg Am, 24: 1279-1280, 1999.
17) Orbay JL: The treatment of unstable distal radius frac- tures with volar fixation. Hand Surg, 5: 103-112, 2000.
18) Orbay JL, Touhami A: Current concepts in volar fixed- angle fixation of unstable distal radius fractures. Clin Orthop Relat Res, 445: 58-67, 2006.
19) Osada D, Viegas SF, Shah MA, Morris RP, Patterson
RM: Comparison of different distal radius dorsal and vol- ar fracture fixation plates: a biomechanical study. J Hand Surg Am, 28: 94-104, 2003.
20) Peine R, Rikli DA, Hoffmann R, Duda G, Regazzoni P:
Comparison of three different plating techniques for the dorsum of the distal radius: a biomechanical study. J Hand Surg Am, 25: 29-33, 2000.
21) Ring D, Jupiter JB, Brennwald J, Büchler U, Hastings H Jr: Prospective multicenter trial of a plate for dorsal fixation of distal radius fractures. J Hand Surg Am, 22:
777-784, 1997.
22) Schnur DP, Chang B: Extensor tendon rupture after in- ternal fixation of a distal radius fracture using a dorsally placed AO/ASIF titanium pi plate. Arbeitsgemeinschaft für Osteosynthesefragen/Association for the Study of Internal Fixation. Ann Plast Surg, 44: 564-566, 2000.
23) Suckel A, Spies S, Münst P: Dorsal (AO/ASIF) pi-plate osteosynthesis in the treatment of distal intraarticular radi- us fractures. J Hand Surg Br, 31: 673-679, 2006.
24) Tavakolian JD, Jupoiter JB: Dorsal plating for distal ra- dius fractures. Hand Clin, 21: 341-346, 2005.