= 증례보고 = 접수번호 : 50-09-10-16
뇌하수체선종으로 인한 단안 무광각 환자에서 수술 후 정상시력 회복을 보인 1예
김상현⋅석경원⋅이주은 메리놀병원 안과
목적: 뇌하수체선종으로 인한 단안 무광각 환자에서 수술 후 정상 시력 회복을 보인 1예를 경험하였기에 보고하고자 한다.
증례요약: 내원 1년 전 뇌하수체선종 수술의 과거력이 있는 53세 남자 환자가 7주 전 시작된 좌안 시력저하를 주소로 내원하였다.
내원 시 최대교정시력은 우안 1.2, 좌안 무광각이었고 좌안의 대광반사가 소실되어 있었다. 시유발전위검사상 좌안에 일관된 파가 관찰 되지 않았고 뇌자기공명영상검사(MRI)상 3×3.5 cm 크기의 뇌하수체선종이 확인 되었다. 신경외과에서 경접형동 접근법으로 뇌하수 체선종 제거술 및 감마나이프 수술을 시행하였고 수술 후 6주째 좌안 최대교정시력 1.0으로 회복되었다.
결론: 뇌하수체선종으로 인한 압박 시신경 병증에 의해 시력이 무광각 상태에 이르더라도 시력회복의 가능성을 염두에 두고 적극적으로 치료에 임해야 하겠다.
<대한안과학회지 2009:50(9):1437-1441>
■ 접 수 일: 2008년 10월 16일 ■ 심사통과일: 2009년 6월 9일
■ 책 임 저 자: 이 주 은
부산광역시 중구 대청동 4가 12번지 메리놀병원 안과
Tel: 051-461-2469, Fax: 051-462-3534 E-mail: [email protected]
* 본 논문의 요지는 2008년 대한안과학회 제99회 춘계학술대회에서 포스터로 발표되었음.
뇌하수체선종은 전체 두개강내 종양의 10~15%를 차지 하는 종양으로 최대 직경이 10 mm 이상인 거대선종은 시 신경로에 위치하여 시신경을 압박할 수 있다.1,2 이러한 시 신경의 압박으로 인해 압박 시신경병증이 발생할 경우 시야 이상, 시력저하, 시신경 위축 등의 소견을 가져올 수 있다.2 종양에 의한 장기간의 시신경 압박은 시력저하를 심화시켜 실명에 이르게 할 수 있으며, 실명상태에 이르면 수술로 병 변을 제거한다고 하더라도 시력회복은 매우 드문 것으로 알려져 있다.3,4하지만 저자들은 뇌하수체선종으로 인한 시 신경 압박에 의해 시력이 무광각으로 저하된 환자에서 선종 제거술 후 정상 시력으로 회복된 증례를 경험하였기에 이를 문헌 고찰과 함께 보고 하고자 한다.
증례보고
53세 남자환자가 7주 전부터 시작된 좌안의 시력저하를 주소로 내원하였다. 환자는 외항 선원이었으며 1년 전 타병 원에서 뇌하수체선종 제거술을 받은 과거력 외에는 특이사
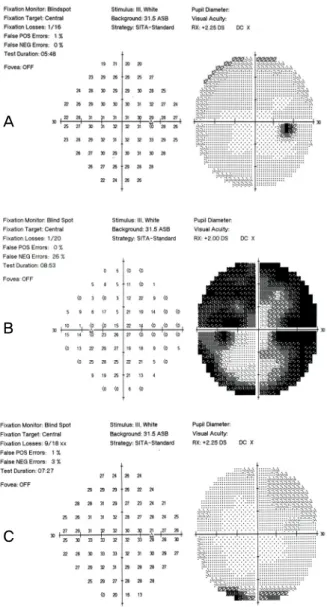
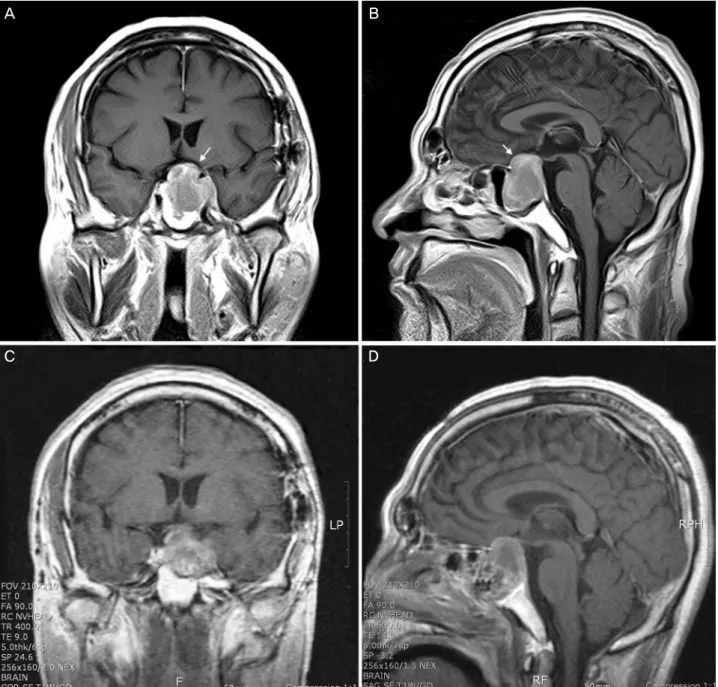
항은 없었다. 다른 신체증상은 호소하지 않았고, 내원시 최 대교정시력은 우안 1.2 좌안 무광각이었으며 안압은 양안 13 mmHg이었다. 직접 대광반사는 우안에서 약간 느리게 나타났으며 좌안에서는 소실되어 있었다. 전안부 검사상 이 상소견은 관찰되지 않았으며, 안저검사상 우안에 비해 좌안 의 시신경 유두가 창백해 보이는 것 외에는 특이소견이 없 었다(Fig. 1). 형광안저 촬영상 양안 모두 특이 소견 보이지 않았으며 시유발전위검사상 좌안에 일관된 파가 관찰되지 않았고 우안은 정상이었다(Fig. 2). 시야 검사는 우안은 정 상이었으며 좌안은 시력이 무광각이었기 때문에 시행할 수 없었다(Fig. 3A). 뇌자기공명영상검사에서 시신경로를 압박 하는 직경 3×3.5 cm 크기의 뇌하수체선종이 발견되었다 (Fig. 4A, B). 신경외과에서 경접형동 접근법으로 뇌하수 체선종 제거술을 시행하였으며(Fig. 4C, D), 술 후 1개월째 감마나이프 방사선 수술을 추가적으로 시행하였다.
경접형동 뇌하수체선종 제거술 후 3주째 안과에 방문하 여 측정한 최대 교정시력은 우안 1.2 좌안 0.8로 좌안 시력 이 급격히 향상되었으며, 전안부 및 안저검사상 특별한 변 화는 관찰되지 않았다. 직접 및 간접 대광반사는 양안에서 정상 소견을 보였으며 상대구심성 동공운동장애도 관찰되 지 않았다. 첫 수술 후 6주째 안과 방문시 좌안 최대교정시 력은 1.0으로 더욱 상승되었다. 시야 검사에서 좌안은 전반 적으로 시야가 좁아져 있었으며, 우안은 중심주시가 잘 되 지 않았으나 시야협착은 보이지 않았다(Fig. 3B, C).
A B
Figure 1. Preoperative fundus photographs show a relatively pale optic disc in the left eye.
A B
Figure 2. Preoperative flash visual evoked potential (FVEP) of the right (A) and the left eye (B). No consistent wave is detected in the left eye compared with normal latency seen in the right eye.
고 찰
뇌하수체선종은 전체 두개강내 종양에서 세 번째로 흔한 종양으로서 전신적인 내분비 장애로 무월경, 유루증, 거인증
등의 증상이 나타날 수 있고, 최대 직경이 10 mm 이상인 거대선종의 경우 종괴 효과에 의하여 시신경로가 압박되면 시력저하, 시야변화, 두통 등의 증상을 일으킬 수 있다. 시야 변화는 가장 흔하게 나타나는 증상으로 시신경 압박 부위에
A
B
C
Figure 3. Humphrey visual field test of the right eye (A) preoperatively and the left (B) and the right eye (C) 6 weeks after transsphenoidal pituitary adenoma resection. Postoperatively, generalized reduction in the sensitivity and constricted visual field is found in the left eye.
따라 양쪽귀 반맹 또는 한쪽귀 반맹이 주로 나타나며 특히 시 신경 압박 증상이 장기간 지속될 경우 시야 변화뿐 아니라 영구적인 시력의 소실도 가져올 수 있다.1-6
본 증례의 환자는 내원 전 점진적인 시력변화가 있다가 내원 7주 전부터 시작된 갑작스런 시력저하를 주소로 내원 하였는데 외항 선원인 관계로 시력 저하가 심했음에도 불 구하고 병원에 바로 방문할 수 없었다. 내원 시에는 이미 좌안 최대 교정시력이 무광각이었고 직접 대광반사도 소실 되어 있었다. 뇌자기공명영상촬영에서 시신경로를 압박하 는 직경 3×3.5 cm 크기의 뇌하수체선종이 발견되었는데
이것에 의한 압박 시신경 병증으로 시력의 감소가 나타났 다고 판단할 수 있었다.
일반적으로 종괴에 의한 압박성 시신경 병증인 경우에 수술로 종괴를 제거하면 술 후 시력이 유의하게 증가될 수 는 있으나. 술 전 시력이 무광각 상태라면 술 후 시력의 회 복은 어려운 것으로 생각된다.4,7 하지만, 실명상태에서도 종양 제거술 후 시력의 회복을 보이는 경우가 보고된 바가 있으며,8-10 Suri et al9의 연구에 의하면 뇌하수체 종양에 의해 시력이 무광각에 이른 79명의 97안 중 23명(29%), 27안(27.8%)에서 시력의 회복을 보였고 안전수지 이상의 시력은 7명(8.9%), 8안(8.2%)에서 보인다고 하였다. 이 보고에서 실명 기간이 짧을수록 시력이 회복되는 경우가 많으며 또한 시력의 향상도 높게 된다고 하였고, 시력의 회 복이 잘되는 인자로 남자, 4주 이하의 짧은 실명기간, 뇌하 수체 졸중(Pituitary apoplexy)의 존재 등을 제시하였다.
하지만 본 증례에서와 같이 실명기간이 4주 이상인 경우에 는 뇌종양 제거술을 하더라도 안전수지 이상의 시력으로 회복되는 경우는 57명 중 한 명 밖에 없었다고 보고하였다.
일반적으로 시신경 교차에 압박이 일어나게 되면 1주일 내에 시신경에 광범위한 탈수초화가 일어나 신경 전도의 저하를 가져오게 된다. 또한 압박에 의해 시신경 축삭이 손 상 받게 되면 시신경 유두의 창백함이 나타나고 손상이 진 행되면서 시신경 유두의 위축소견이 보이게 되는데 이 단 계에서의 시력은 대부분 무광각이며 신경의 회복은 비가역 적인 것으로 생각된다.4,5,11,12종괴에 의한 시신경 압박상태 에서 종괴제거술 후 시력 회복의 기전은 크게 두 가지로 알 려져 있는데 첫째, 수술 후 즉시 혹은 1주일 내에 나타나는 시신경 압박의 해소로 인한 생리적인 신경전도의 회복과 둘째, 수주에서 길게는 몇 년에 걸쳐서 일어나는 시신경 섬 유의 재수초화에 의한 것이다.13,14본 증례에서도 시력 회복 이 위와 같은 기전에 의해서 일어나는 것으로 보이는데 시 력은 비록 무광각이고 시신경 유두는 다소 창백해 보였지만 좌안 시신경의 압박이 비가역적인 위축을 일으키는 단계까지 는 이르지 않았다고 생각할 수 있다.9 또한 술 후 3주째 상 대구심성 동공운동장애는 회복되었지만 술 후 6주째 시야 의 전반적인 협착이 남아있었는데, 이것은 시신경 이상에서 동공 반응과 시야검사 결과가 항상 일치하지만은 않기 때 문으로 생각된다.14
국내에서 아직까지 뇌하수체선종 제거술 후 술 전 시력이 무광각 상태에서 수술 후 정상 시력으로의 회복을 보인 예가 없기에 이를 보고하는 바이며, 뇌하수체 병변으로 인한 압박 시신경병증 환자에서 비록 시력이 무광각 상태이더라도 시력 회복의 가능성을 항상 염두에 두어야 하며 즉각적인 치료가 필요할 것이다.
A B
C D
Figure 4.Preoperative coronal (A) and sagittal (B) enhanced T1-weighted MR image showed peripheral enhancing sellar and suprasellar mass markedly compressing the optic chiasm (arrow). Postoperative coronal (C) and sagittal (D) enhanced T1-weighted MR image showed decreased degree of optic chiasm compression by the partial tumor resection.
참고문헌
1) Asa SL, Kovacs K. Clinically non-functioning human pituitary adenomas. Can J Neurol Sci 1992;19:228-35.
2) Melen O. Neuro-opthalmologic features of pituitary tumors. Endo- crinol Metab clin North Am 1987;16:585-608.
3) Jallu A, Kanaan I, Rahm B, Siqueira E. Suprasellar meningioma and blindness: a unique experience in Saudi Arabia. Surg Neurol 1996;45:320-3.
4) Kang SM, KimJH, Cheong JH. Relationship between location and size of pituitary adenoma and visual field change. J Korean
Ophthalmol Soc 2005;46:1690-6.
5) Elkington SG. Pituitary adenoma. Preoperative symptomatology in a series of 260 patients. Br J Ophthalmol 1968;52:322-8.
6) Dekkers OM, de Keizer RJ, Roelfsema F, et al. Progressive improvement of impaired visual acuity during the first year after transsphenoidal surgery for non-functioning pituitary macro- adenoma. Pituitary 2007;10:61-5.
7) Bampoe J, Ranalli P, Bernstein M. Postoperative reversal of complete (monocular) blindness in skull base meningioma: case report. Can J Neurol Sci 2003;30:72-4.
8) McGirt MJ, Cowan JA Jr, Gala V, et al. Surgical reversal of
=ABSTRACT=
A Case of Complete Visual Recovery From No Light Perception After Resection of Pituitary Adenoma
Sang Hyun Kim, MD, Kyung-Won Suk, MD, Joo Eun Lee, MD, PhD
Department of Ophthalmology, Maryknoll Hospital, Busan, Korea
Purpose: We report a case of a patient with no preoperative light perception who achieved complete visual recovery after transsphenoidal resection of a pituitary adenoma.
Case summary: A 53-year-old man with a history of pituitary adenomectomy visited our clinic complaining of decreased vision of 7 weeks ducation. His best-corrected visual acuity was 1.2 in his right eye, and he had no light perception (NLP) in his left eye. Light reflex was absent in the left eye, and no consistent wave was detected in the left eye on flash visual evoked potential (FVEP). A pituitary adenoma 3×3.5 cm in diameter was found following magnetic resonance imaging (MRI), and was removed using a transsphenoidal approach and gamma knife radiosurgery. Six weeks postoperatively, his best corrected visual acuity improved to 1.0 in the left eye.
Conclusions: Prompt management should be initiated in patients with no light perception vision, due to compressive optic neuropathy.
J Korean Ophthalmol Soc 2009;50(9):1437-1441
Key Words: Blindness, Pituitary adenoma, Recovery vision
Address reprint requests to Joo Eun Lee, MD, PhD Department of Ophthalmology, Maryknoll Hospital
#12 Daecheong-dong 4-ga, Jung-gu, Busan 600-730, Korea
Tel: 82-51-461-2469, Fax: 82-51-462-3534, E-mail: [email protected] prolonged blindness from a metastatic neuroblastoma. Childs Nerv Syst 2005;21:583-6.
9) Suri A, Narang KS, Sharma BS, Mahapatra AK. Visual outcome after surgery in patients with suprasellar tumors and preoperative blindness. J Neurosurg 2008;108:19-25.
10) Clifford-Jones RE, Landon DN, McDonald WI. Remyelination during optic nerve compression. J Neurol Sci 1980;46:239-43.
11) Smith EJ, Blakemore WF, McDonald WI. Central remyelination restores secure conduction. Nature 1979;280:395-6.
12) Kerrison JB, Lynn MJ, Baer CA, et al. Stages of improvement in visual fields after pituitary tumor resection. Am J Ophthalmol 2000;130:813-20.
13) Gnanalingham KK, Bhattacharjee S, Pennington R, et al. The time course of visual field recovery following transphenoidal surgery for pituitary adenomas: predictive factors for a good outcome. J Neurol Neurosurg Psychiatry 2005;76:415-9.
14) Bremner FD, Pupil assessment in optic nerve disorders. Eye 2004;18:1175-81.