골다공증성 척추 골절의 방사선적 진단
원광대학교 의과대학 정형외과학교실, 방사선학교실
1채수욱․김강득
1Radiographic Diagnosis of the Osteoporotic Vertebral Fractures
Soo Uk Chae, Gang Deuk Kim
1Department of Orthopedic Surgery,
1Department of Radiology, School of Medicine, Wonkwang University Hospital, Iksan, Korea
Osteoporotic vertebral fractures are associated with increased morbidity and mortality. Morbidity associated with these fractures includes pain and decreased physical function, which have a significant impact on the quality of life. The detection of osteoporotic vertebral fracture is based mainly on the identification of vertebral collapse, but this can be misleading in the presence of a fracture without radiologic collapse. And the diagnosis of vertebral fractures in simple radiographs is difficult because of normal variants and degenerative change of vertebrae. We review the various methods for evaluating osteoporotic vertebral fractures based on simple radiography or dual-energy X-ray absorptiometry (DXA).
The preferred method may be Genant’s semiquantitative method which was developed in an attempt to reduce subjectivity associated with visual diagnosis of osteoporotic vertebral fracture. Recently, vertebral fracture assessment (VFA) by DXA can be used to detect vertebral fractures in asymptomatic patients undergoing routine BMD measurements. Yoshida’s classification is useful alternative method in the incidental vertebral fracture diagnosis with a morphological change in the anterior bone cortex.
Key Words: Osteoporosis, Spinal fractures, Radiography
Received: February 18, 2013 Revised: April 23, 2013 Accepted: March 15, 2013
Corresponding Author: Gang Deuk Kim, Department of Radiology, School of Medicine, Wonkwang University, 895 Muwang-ro, Iksan, Jeonlabuk-do 570-711, Korea
Tel: +82-63-472-5100, Fax: +82-63-472-5688, E-mail: gdkim@wku.ac.kr
* 본 논문은 2011년도 원광대학교 교내 연구비 지원으로 이루어졌음.
척추 압박 골절은 골다공증 환자에서 가벼운 외상 으로도 쉽게 발생되며 고령화의 가속화로 발생 빈도 가 증가되고 있다. 골절 자체의 통증과 보행 제한 등 의 신체적 활동 감소와 골절 후 잔존하는 척추 변형 에 의해 삶의 질 감소 및 사망률에 많은 영향을 초 래하여 사회 경제적으로 많은 문제점이 야기된다.
1임상적으로 방사선적 추체 붕괴여부에 따라 3개의 범주로 나눌 수 있는데 (1) 추체가 붕괴되면서 발생 하는 통증이 있는 급성(acute) 골절 (2) 추체 붕괴가
동반되나 무증상의 진구성(old) 골절 (3) 방사선적 추체 붕괴 없이 증상이 동반되는 잠재성(occult) 골 절이다.
2척추 골절의 진단은 추체의 붕괴나 변형으로 단순
방사선 사진으로 가능하나, 추체의 붕괴와 변형이
심하지 않은 경우에 과소 진단(underdiagnosis) 되는
경향이 있다. 또한 추체의 정상적인 변이 소견들과
퇴행성 척추 변화에 의한 형태적인 추체 변형이 압
박골절로 과진단(overdiagnosis) 되기도 한다.
3,4골절
의 진단이 늦어질수록 추체의 붕괴가 진행되어 신경 증상과 척추의 변형이 발생하여 심각한 장애가 초래 되고, 골절과 골다공증에 대한 치료 지연으로 인해 척추부와 고관절부 등의 타부위에 추가 골절이 발생 되어 나쁜 결과를 초래 할 수 있다. 현재까지 보고된 척추 골절의 방사선적 평가 방법들은 추체의 붕괴와 변형에 대해 시각적이며 직관적인 방법으로 주관적 편차가 많이 있으며, 추체의 붕괴와 변형이 경미한 경우엔 객관적인 진단 기준이 없는 실정이다.
5-10잠 재성 골다공증성 척추 골절과 골다공증 검사 시 우 연히 발견되는 경미한 척추 골절은 대부분 추체의 붕괴 소견이 없어 방사선적 진단에 어려움이 있다.
11단순 방사선 사진에서 간과 될 수 있는 골다공증성 척추 골절을 골주사 검사(bone scan)나 자기공명 영 상(MRI) 촬영으로 확진 할 수 있으나, 일차 진료 시 기기 활용에 한계와 비용적인 측면에서 어려움이 있 다.
12이에 골다공증성 척추 골절의 진단과 분류의 여러 방사선적 측정 방법들에 대해 문헌 고찰하여 각각의 장단점과 임상적 활용성에 대해 알아보고자 한다.
골다공증 척추 골절의 방사선적 평가 방법
1. 정성적 방법(Subjective visual (Qualita-
tive) assessment)
척추 측면 방사선 사진으로 척추 골절을 직관적으 로 진단하는 간단한 방법이다. 방사선 영상의 선명 도가 많은 영향을 미치며 재현성(reproducibility)이 매우 낮고, 측정 간(intraobserver) 87%, 측정자 간 (interobserver) 75%의 신뢰도로 보고되고 있다.
9표준 화된 객관적인 지표가 없고 위음성(false negative)률 이 30% 이상 과소 진단이 많아 많은 훈련과 경험이 필요한 평가 방법이다.
32. 반정량적 방법(Standardized visual (Semi- quantitative) assessment)
표준화된 방사선적 척추 골절 평가 방법은 1960년 Smith 등
13이 골다공증 정도를 판단하기 위해 측면 흉 ․ 요추부 방사선 사진으로 추체 변형에 대해 한 단 계만 최초로 보고한 이후, Meunier 등
14이 정상 추체
의 1단계부터 골절 변형된 추체를 4단계까지 단계별 로 점수화(radiological vertebral index: RVI)하여 골절 된 추체의 합으로 평가하였고, Kleerekoper과 Nelson
15가 추체의 변형을 0에서 3까지 단계별로 점수화하여 척추변형점수(vertebral deformity score: VDS)로 분류 하였다. 추체의 변형은 추체의 전방이 압박 골절된 경우 설상 압박골절(wedge compression fracture), 추 체의 전 ․ 후방의 높이는 유지되나 중간 높이가 감소 된 경우 양요골절(biconcave fracture), 추체의 전, 후 방과 중간 높이가 모두 감소된 경우 압궤골절(crush fracture)로 구별하여 분류하였다. 그러나 정상 변이 (variation)의 추체 변형과 경도의 추체 종판 골절의 진단에 어려움이 있으며, 척추 골절 예후 예측에 한 계가 있었다. Genant 등
5,16이 척추 골절은 척추 변형 을 항상 동반한다는 개념으로 단순 방사선 사진상 골절된 추체의 압박 정도를 비율화 하여 반 정량적 인 분석 방법으로 구분하였다. 추체의 붕괴가 없는 정상을 0도, 20~25% 경도(mild) 붕괴가 있는 경우 1 도, 25~40%의 중증도(moderate) 붕괴가 있는 경우를 2도, 40% 이상의 심한(severe) 붕괴가 있는 경우를 3 도로 분류하였으며, 이와 더불어 20% 미만의 경미 한 붕괴가 있는 경우를 0.5도(borderline)로 분류하였 다(Fig. 1).
17이 분류는 특이성과 재현성이 높고 측정 간 93~99%, 측정자 간 90~99%의 신뢰도가 높아 역학조사, 약물 효과 조사, 골절 예후 예측 및 추적 관찰에 용이하여 현재 많이 사용되고 있다.
17,18이 분 류의 제한점은 여성 흉추의 중간부와 남성 흉 ․ 요추 부 추체가 타 부위보다 형태적으로 약간의 설상 모 양을 가지고 있어 진단과 분류에 어려움이 있으며, 경도의 추체 붕괴가 있는 0.5도에서 1도 사이의 골절 은 관찰자의 주관적 판단에 의존하여 진단에 오류가 발생한다. 그리고 이 분류는 정상 추체를 사각 모양 으로 규정하고 있어 잠재성 척추 골절 진단과 추체 함몰이 없는 종판 변형된 골절 진단에 어려움이 있 는 단점이 있다.
63. 알고리즘을 이용한 정성적 방법(algorithm- based gualitative assessment)
모든 척추의 골절이 추체의 가장 약한 부위의 종
판 중간부에서 먼저 발생한다는 가정하에 추체의
0: normal unfractured vertebrae:
0.5: uncertain or questionable vertebrac;
1: a MILD deformity with a 20-25% reduction in anterior. middle. and/or posterior height (relative to the same or adjacent vertebrae) accompanied by a reduction in area of approximately 10-20%;
2: a MODERATE deformity with a >25-40% reduction in any height and an approximate 20-40% reduction in area;
3: a SEVERE deformity with a reduction of >40% in any height and accompanying area;
Anterior Middle
Severe Fractures Posterior
Anterior Middle
Moderate Fractures Posterior
Anterior Middle
Mild Fractures Posterior
Normal / Uncertain
Wedge fracture Biconcave fracture Crush fracture
Fig. 1. Schematic diagram of the Genant semiquantitative grading scale for vertebral fracture, is classified into four grades (from 0 to 3) according to the degree of collapse (From Genant et al
17).
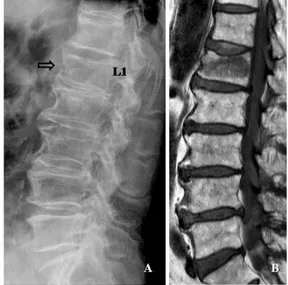
Fig. 2. A 77- year- old woman with osteoporotic com- pression fracture of L1. There is a depression in the central endplate (blank arrow) within the vertebral ring (arrow).
높이의 변화보다 중심부 종판의 형태로 골절을 진 단하는 방법으로 정상, 골다공증성 골절(추체 종판 함몰)과 비 골절 추체 변형(종판 함몰 없이 15% 내외 의 추체 높이 감소와 정상 변이)의 3가지 유형으로 분류하였다(Fig. 2).
6이 분류에 의하면 설상과 압궤 골절은 종판이 오목한(concave) 유형의 골절로 척추 의 가장 자리(vertebral ring)내에서 추체의 종판이 함 몰된 골절 유형이며, 특히 설상 골절은 추체 전방 피질골의 골절로 추체 전방 함몰이라 기술하였다.
미리 정해놓은 순서도에 의해 주관적인 오차를 낮 추고, 측정자 간 재현성에 좋은 결과를 보이는 정성 적 평가 방법이나,
19측정자에게 많은 숙달이 요구되 며, 종판 판단을 위해서는 정확한 척추 측면 방사선 이 우선되어야 하는 어려움이 있다. 또한 알고리즘 에 대한 설명서와 참고 그림을 같이 사용하여야 하 며, 종판의 정상적인 변이 소견들과 감별이 어려워
위양성 소견이 많아 현재 임상적으로 많이 이용되 고 있지는 않다.
18Fig. 3. Six-point placement in quantitative vertebral mor- phometry (Ha: nterior height, Hm: middle central) height, Hp: posterior height).
Fig. 4. The morphological Yoshida classification.
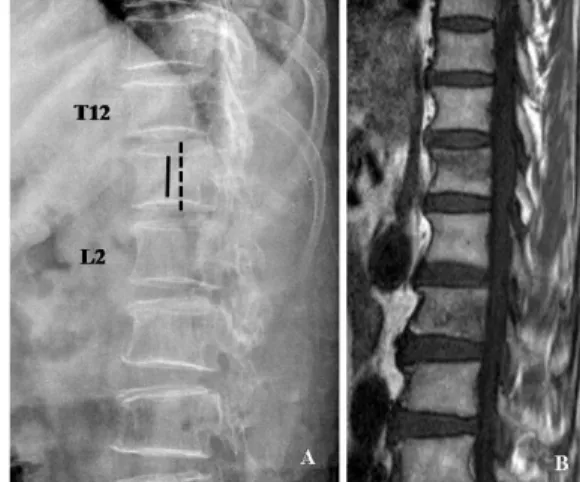
Fig. 5. A 87- year- old woman with occult osteoporotic vertebral fractures of L2 (A), confirmed by MRI (B). Radiograph shows nearly equal vertebral height with adjacent vertebrae (black line), but L2 has a change of anterior cortex morphology (protruding type of Yoshida’s classification) (arrow).
4. 형태학적 정량적 분류(Quantitative mor- phometric assessment)
단순 측면 방사선 사진에서 추체 전방(Ha), 중간 (Hm), 후방(Hp)에 상하로 각각 6개의 점을 찍어 높 이를 측정하여 설상 압박 비율(Ha/Hp), 양요 비율 (Hm/Hp), 압궤 비율(Hpi/Hpi-1)(1는 위 ․ 아래 척추와 의 비교)을 계산하여 정상치에서 3 표준편차 이하 이거나 세 개 중 최소 한 개의 추체 상하의 높이가 15%이상 감소된 경우를 골절로 정의하는 방법이다 (Fig. 3).
10,20그러나 추체 상하의 기준점을 설정할 때
측정자의 주관적 요소와 종판 변형으로 전 ․ 후 종판 이 평행하지 않을 경우(시차 효과(parallax effect)) 어 려움이 있다. 척추 측만증 환자나 골다공증이 있는 노인에서 사면 촬영이 되는 등 정확한 방사선 사진 을 얻기에 어려움이 있고, 다른 원인에 의한 척추 변 형과 구별이 힘들다는 단점이 있다. 이에 형태학적 분류를 사용할 때 단독으로 사용하기보다는 정량적 인 방법을 같이 사용하여 진단하는 것이 좋다.
5. Yoshida 분류법
2000년에 Yoshida에 의해 추체의 붕괴가 심하지 않는 우연히 발견되는 척추 골절(incidental fracture) 에 대해 추체의 전방 피질골과 종판의 변화에 대해 분류를 시행하였다. 추체의 전방 피질골의 형태학적 인 분류로 전방 피질골이 돌출되는 형(protruding type), 전방 피질골이 분열되어 톱니 모양으로 후방 전위되는 형(indented type)과 전방 전위되는 형(end plate slippage type), 종판이 골절되어 함몰되는 종판 함몰형(endplate compression type)으로 분류하였다 (Fig. 4, 5).
7이 분류는 전방 피질골의 형태적 변화에 의한 돌출형과 톱니 모양형은 골절 진단의 정확도가 높으나 종판의 형태 변화에는 진단의 정확도가 낮은 단점이 있다. 그러나 추체의 함몰에 의한 높이 변화
protruding type
indented type
end plate slippate type
end plate
compression type
Fig. 6. A 87- year- old man with occult osteoporotic vertebral fracture of L1 (A), confirmed by MRI (B). Radiograph shows confusion by degene- rative bony spurs (arrow).
가 없는 잠재성 척추 골절 진단에 추체의 전방 피질 골의 변화를 주의 깊게 관찰한다면 많은 도움을 줄 것으로 생각된다.
6. 이중에너지 방사선 흡수법(Dual-energy X- ray absorptiometry (DXA) assessment) 이중에너지 방사선 흡수 장치(DXA)는 골다공증 진단을 위한 골밀도 측정 기본 검사이지만 척추 골 절에 대해 정량적으로 진단할 수도 있다. 우리나라 에서는 주로 이용되고 있지 않지만 흉추부와 요추부 을 동시에 정량적으로 측정할 수 있으며, 고관절부 에서도 형태 계측법으로 임상에 적용이 가능하다.
DXA을 이용하여 척추 골절을 진단하는 형태 계측 법을 총괄하여 VFA (Vertebral Fracture Assessment)로 부르고 있다. 방사선 노출 정도(3 micro-Sieverts (μ Sv))도 흉 ․ 요추부 외측 단순 방사선 촬영(600μSv) 보다 적으며, 추체 종판과 평행하게 팬빔(fan beam) 이 투과하여 일반 방사선 영상의 확대(magnifica- tion), 왜곡(distortion) 없이 촬영 시간을 줄이고 해상 도 높은 양질의 영상으로 척추 형태를 측정할 수 있 는 장점이 있다. 그러나 척추 측만증이나 중증의 다 발성 퇴행성 추간판 질환에서는 측정에 어려움이 있 다. DXA 방법으로 형태 계측법은 골다공증 검사를 시행하면서 무증상 척추 골절 진단에 많은 도움이 될 것으로 전망된다.
8,21,22골다공증 척추 골절 방사선적 진단 시 고려 사항
1. 잠재성 골다공증성 척추 골절(Occult osteo- porotic vertebral fracture)
천골이나 대퇴골 경부에서 흔히 발생하는 잠재성 또는 부전(occult or insufficiency) 골절처럼 방사선 사진상에 척추의 함몰 없이 발생하는 척추 골절로 정의한다(Fig. 5). 잠재성 척추 골절의 진단은 (1) 급 성 통증과 운동 제한 등의 증상이 동반되는 급성 골 절 (2) 최초 방사선 사진상 정상 추체 소견(Genant 분류상 0도)이며 자기공명영상(MRI)이나 골주사 검 사(bone scan)로 급성 골절이 확진된 골절 (3) 골다공 증(BMD <80 mg/cm
3과 T-점수 <-2.5)이 동반되고
다른 기저질환이 없는 경우를 모두 포함한 경우로 정의하였다.
11,12초기 방사선 사진상 정상이지만 시간이 지난 후 지연성 척추 붕괴가 발생하는 원인은 골절의 발생 부위가 대부분 요추부로, 이는 생역학적 스트레스가 다소 작은 부분으로 일시적으로 초기에 추체의 높이 가 보존된 것이 아닌가 추정하였다.
11또한 추체 내 부에 가스 붕괴와 함께 지연 붕괴가 발생하는 점을 들어 Kummell씨 병의 첫 단계로 보는 경우도 있다.
12잠재성 척추 골절은 MRI상 추체 부종과 출혈에 의 해 척추골의 신호 이상 소견이 전이성 종양 등의 전 신 질환과 감별이 필요하다.
2. 정상적인 변이(Normal variations)및 감별 진단
척추 골절의 방사선 진단 시 통상적으로 흉추 4번 부터 요추 4번까지의 범위에서 발생된 골절 진단에 유용하다. 흉추 4번 이상 부위에서 단독 골절은 거의 없으며, 견갑골과 견관절에 의해 음영이 뚜렷하지 않다. 요추 5번 또한 시차 효과에 의해 진단에 어려 움이 있다.
16,23추체의 정상적인 형태 변이, 퇴행성 척추 변화에
의한 골극 형성(Fig. 6)과 방사선 촬영 시 자세와 방
Fig. 7. A 70- year- old woman with occult osteoporotic vertebral fractures of T12 and L2 (A), con- firmed by MRI (B). Radiograph shows potential pitfall of overdiagnosing osteoporotic fracture of L1 that parallax can cause.
Fig. 8. A 77- year- old women with occult osteoporotic vertebral fractures of L1 (A), confirmed by MRI (B). Radiograph shows same shape and size compared with adjacent vertebrae.
사선 영상 자체의 왜곡과 확대, 관찰자의 편향된 시 선 등으로 척추 골절에 대해 정확한 진단과 감별에 혼동을 초래한다. 종판 부위에서 감별점은 시차 효 과로 종판의 높이 차이가 종판의 함몰로 오인되기가 쉬우며(Fig. 7), 정상적인 변이의 Cupid의 활(Cupid’s bow)과 limbus 척추, Scheuermann병(종판의 불규칙 성)과 Schmorl 결절(연골하 종판이 파괴되어 추간판 디스크 물질의 일부가 추체내로 이동)과 구별이 필
요하다.
19,24인접 추체와의 음영 차이와 크기 차이의
상대적인 비교에 시각적인 판단 오류와 흉추부 추체 의 정상적인 크기의 차이와 구별에 어려움이 있다 (Fig. 8).
결 론
단순 방사선 사진에서 골다공증성 척추 압박골절 의 진단은 숙달된 훈련과 많은 경험이 필요하며, 정 성적 방법과 반정량적 방법 중 Genant의 반정량적 방법이 임상적으로 많이 사용되고 있으나 잠재성 골 절 등의 추체의 형태 변화가 없을 때 진단에 어려움 이 있다. 최근 DXA로 골밀도 측정 시 고해상도의 사진으로 추체 형태 측정이 용이하여 무증상의 척추 골절 진단에 유용하게 사용될 수 있으며, 잠재성 척 추 골절에 대해 추체 전방 피질골의 형태적 변화와
종판의 변화에 대한 Yoshida 분류법이 진단의 한 방 법으로 이용할 수 있을 것으로 사료된다.
참 고 문 헌